Bioimpedance spectroscopy (BIS) is an established tool for the measurement of extracellular fluid in lymphedema. This study assesses the validity of BIS measurements using the l-Dex® for evaluating the effectiveness of interventions to treat lymphedema. Measurements are correlated with limb volume, assessment of pitting edema, physiologic measures of lymphatic function, and response to surgical intervention. Three l-Dex BIS metrics are compared.
Methods and Results:
This retrospective study of prospectively collected data identified consecutive patients with lymphedema. l-Dex BIS measurements, limb volume measurements using perometry, transport index (TI) evaluation using radioisotope lymphoscintigraphy, staging using indocyanine green (ICG) fluorescent lymphography, and clinical evaluation of degree of pitting edema were compared to examine correlations. l-Dex BIS metrics included the l-Dex ratio, absolute difference between the affected and unaffected extremities, and their unadjusted ratio. The study included 26 patients with 70 sets of evaluations. There were significant correlations between the l-Dex ratio and limb volume ratio (LVR) using perometry, the degree of pitting edema, TI evaluation using lymphoscintigraphy, and staging using ICG lymphography. Of the l-Dex BIS metrics, the l-Dex ratio correlated most closely with all measures (ρ = 0.71–0.94, p < 0.0001). Following complete decongestive therapy, the mean decrease in the l-Dex ratio was 48.3% whereas the corresponding mean reduction in limb volume was 13.8% (ρ = 0.19; p = 0.65); subsequent physiological surgery including lymphovenous bypass and vascularized lymph node transfer resulted in an average reduction in l-Dex ratio of 36.1% and mean limb volume reduction of 25.2% (ρ = 0.38; p = 0.27).
Conclusions:
L-Dex BIS measurements demonstrate face, construct, and criterion validity, and correlate with clinical assessment, LVR, physiologic measures of lymphatic function, and response to conservative and surgical intervention. The L-Dex ratio correlates most closely with all measures and is the recommended metric when using BIS.
Background
Lymphedema is a chronic and debilitating condition. In the Western world, it most commonly occurs secondary to cancer treatment.1,2 Risk factors include regional lymphadenectomy and regional nodal irradiation.3 While the upper extremity is most frequently affected following breast cancer therapy, lymphedema may affect either the upper or lower extremities, or head and neck, secondary to surgery and adjuvant therapy for sarcoma, melanoma, gynecologic, or genitourinary carcinomas.4,5 Following these interventions, lymphatic fluid is mechanically obstructed, leading to stasis within the extremity. The inflammatory response results in progressive sclerosis and fibrosis of the lymphatic vessels and soft tissues and subsequent localized adipose tissue differentiation, leading to an irreversible chronic lymphedema phenotype.6–8 Early lymphedema is therefore characterized by accumulation of extracellular fluid, whereas established lymphedema is a condition of both extracellular fluid and excess subcutaneous fibroadipose tissue.
Diagnosis and longitudinal surveillance of lymphedema remain a challenge. Measurement modalities can be categorized into objective measurements of volume or extracellular fluid, and subjective physiological lymphatic vessel function. Limb volume measurements are the most commonly used modality for diagnosis and evaluation of lymphedema; these can be obtained from truncated cone calculations from circumferential measurements, water displacement, and volumetry using a perometer. The perometer, which uses mobile infrared optoelectronic volumetry, is valid and reliable in lymphedema.9–13 It is proposed that volume change between 5% and 10% is clinically diagnostic, with limb volume change (LVC) of 5% or more classified as mild lymphedema, and 10% or more as moderate to severe.5,10
Bioimpedance spectroscopy (BIS) measures extracellular fluid in an extremity, with sensitivity for diagnosing lymphedema at an early stage.11–23 The most common BIS device is the l-Dex machine, which employs multi-frequency bioimpedance analysis, allowing the impedance to be calculated when the current is extrapolated back to 0 Hz. At these low frequencies the cell membrane is an insulator, preventing the current from passing through the intracellular water, and the resistance at zero frequency (R0) is therefore a direct representation of extracellular water.11–15 The adjusted resistance in the affected limb is expressed relative to that of the unaffected limb using the l-Dex ratio. BIS is predominantly validated for evaluation of preclinical and early lymphedema; its value in established lymphedema and following conservative and surgical treatment interventions remains less clear.11–24
The gold-standard investigation for lymphatic physiological function is radioisotope lymphoscintography, allowing for evaluation of both the deep and superficial lymphatic systems and the draining lymph nodes.25–33 The transport index (TI) is valid for measuring lymphatic function,25,26 and staging scales using the dermal backflow pattern and severity have been described28–30 and validated.24 Indocyanine green (ICG) fluorescent lymphography, although predominantly used to localize lymphatic vessels for lymphovenous bypass (LVB) surgery, allows for detailed evaluation of the superficial lymphatic system. Staging systems based on dermal backflow severity and distribution correlate closely with the pathological condition of the lymphatic vessels.34–39
The purpose of this study was to analyze the face, construct, and criterion validity of BIS measurements using l-Dex in patients undergoing nonoperative and operative therapy for both early established, and chronic, upper and lower extremity lymphedema.
Materials and Methods
A retrospective study of consecutive patients with lymphedema referred to a specialist lymphedema surgical service in a 6-month period from April to September 2017 was conducted. Patients with complete evaluations sets were included, consisting of l-Dex measurements, limb volume using perometry, evaluation of TI using radioisotope lymphoscintigraphy, staging using ICG fluorescent lymphography, and clinical evaluation of degree of pitting edema. The study was approved by the Institutional Review Board (Protocol number PA17-0977).
L-Dex BIS
BIS was performed using the L-Dex U400 (Impedimed, Carlsbad, CA) with standardized placement of electrodes on the surface of the skin allowing the entire extremity to be measured.14 Measurements were taken with patients in the supine position with arms by their side.13,16,40 Two trained medical assistants performed all measurements. The ratio of impedance at R0 in the affected versus the unaffected limb, adjusted for sex, upper/lower limb and right/left dominance, is expressed as the l-Dex ratio.41 Further, the absolute difference in impedances between the unaffected and affected limbs, and their unadjusted ratio, are calculated. An l-Dex ratio of −10 to +10 is considered normal, and above 10 diagnostic for lymphedema.15,18 An l-Dex ratio of zero represents the mean impedance ratio, and 10 is equal to a linear change of approximately three standard deviations.
Limb volume measurement using perometry
Two trained medical assistants performed all perometer volumetry measurements. A calibrated, vertically orientated perometer 400NT (Mitaka USA, Inc., Denver, CO) was used. Measurements were made from the wrist, identified using a bead to the most proximal point of the upper arm; this same length was used for all subsequent measurements. Three measurements were taken for each limb and the mean was calculated. The difference between the affected and unaffected limbs is expressed using the limb volume ratio (LVR). LVC is expressed over time using the LVC:
\documentclass{aastex}\usepackage{amsbsy}\usepackage{amsfonts}\usepackage{amssymb}\usepackage{bm}\usepackage{mathrsfs}\usepackage{pifont}\usepackage{stmaryrd}\usepackage{textcomp}\usepackage{portland, xspace}\usepackage{amsmath, amsxtra}\usepackage{upgreek}\pagestyle{empty}\DeclareMathSizes{10}{9}{7}{6}\begin{document}
\begin{align*}
{ \rm { LVC = } } { \frac { ( { { \rm { A } } _ { { \rm { followup } } } } { { { ^- } \rm { A } } _ { { \rm { baseline } } } } ) - ( { { \rm { U } } _ { { \rm { followup } } } } { { { ^- } \rm { U } } _ { { \rm { baseline } } } } ) } { { { \rm { A } } _ { { \rm { baseline } } } } } } \times 100 \%
\end{align*}
\end{document}
where A = the volume of the affected extremity, and U = the volume of the unaffected extremity.
Clinical evaluation of degree of pitting edema
The degree of pitting edema was evaluated by an experienced lymphedema specialist plastic surgeon at multiple points on either the forearm or lower leg by compression with the thumb for 1 minute.42,43 The affected and unaffected sides were compared. The degree of pitting edema was expressed using the pitting edema scale, with the highest measurement recorded (0, no pitting edema; 1+, 2 mm depression that disappeared rapidly; 2+, 4 mm depression that disappeared in 10–15 seconds; 3+, 6 mm depression lasting longer than a minute; 4+, severe depression lasting more than 2 minutes).
TI using technetium lymphoscintigraphy
The TI quantifies the visual findings with radioisotope lymphoscintigraphy to provide a measure of dynamic lymphatic function with high interobserver reliability.25,26 Several parameters are evaluated in serial scans, including lymphatic transport kinetics, radiocontrast distribution pattern, time to appearance of lymph nodes, and assessment of lymph nodes and lymph vessels. The total score of the TI ranges from 0 to 45.
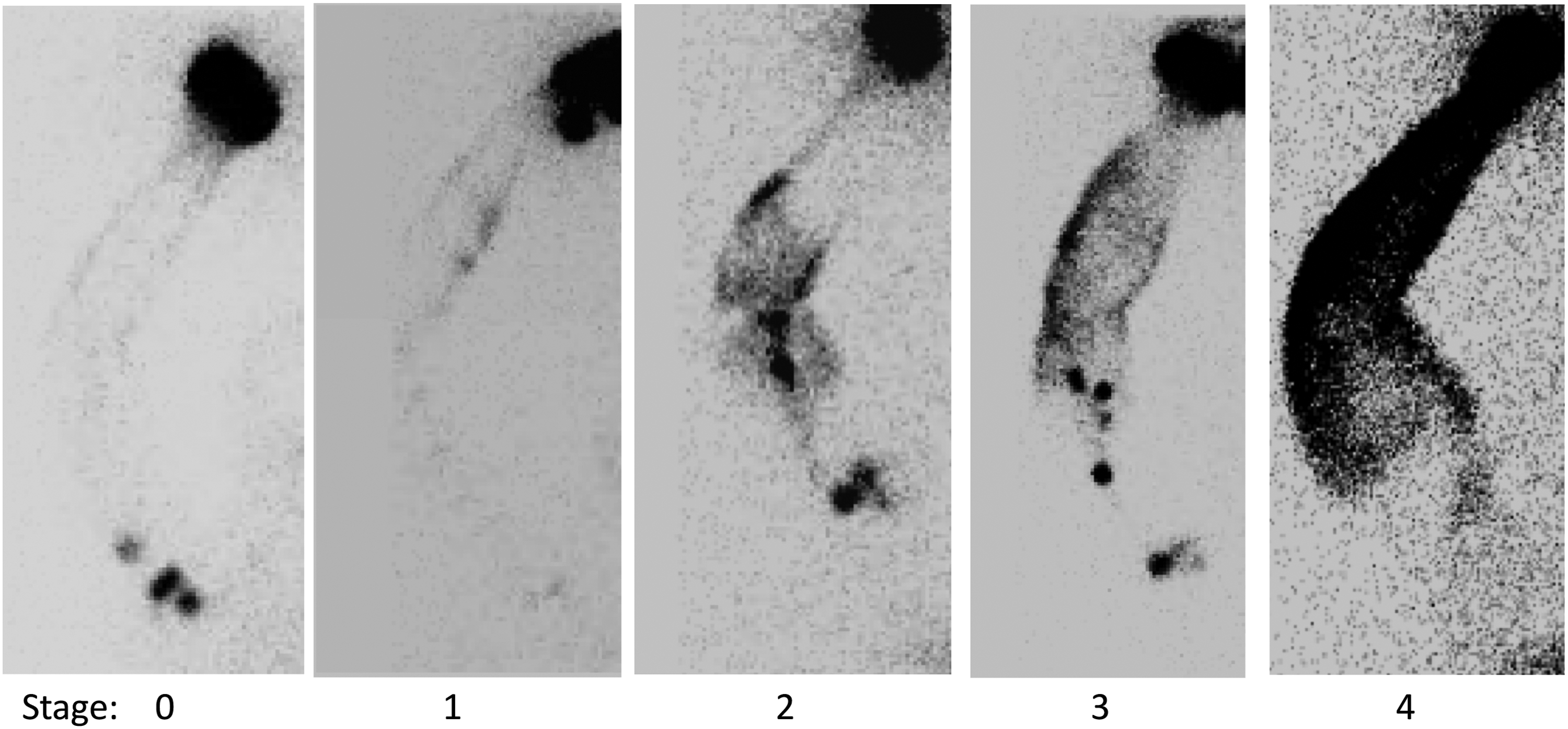
Patients underwent intradermal injection of 2 mCi of technetium-99m sulfur colloid into the digit webspaces. Serial hemibody scans of the tracer were acquired. The TI was evaluated by both an experienced radiologist (F.C.W.) and a lymphedema specialist plastic surgeon (M.V.S.). Further, the superficial and deep lymphatic function and distribution of dermal backflow were assessed and staged using the lymphoscintigraphy staging scale (LSS) (Fig. 1). All patients were confirmed to have normal lymphatic function in the unaffected extremity on lymphoscintigraphy.
Technetium-99m sulfur colloid Lymphoscintigraphy Staging Scale. Stage 0: Normal lymphatic vessels clearly visualized, no dermal backflow, no delay, sentinel lymph nodes clearly visualized. Stage 1: Lymphatic vessels clearly visualized, small areas of patchy dermal backflow affecting the distal extremity. Stage 2: Faint visualization of lymphatic vessels, segmental dermal backflow affecting the distal and proximal extremity. Stage 3: Lymphatic vessels hardly recognizable, diffuse dermal backflow affecting the distal and proximal extremity. Stage 4: No lymphatic vessels visualized, severe diffuse dermal backflow in the entire extremity, no lymph nodes visualized; alternatively no flow is seen throughout the entire limb and no lymph nodes are visualized.
ICG fluorescent lymphography
Lymphatic function of the affected extremity was evaluated using ICG fluorescent lymphography intraoperatively. Approximately 0.01–0.02 mL of ICG (0.25–0.5 mg) was injected intradermally into each webspace. Lymphography was performed using a Hamamatsu PDE Neo II imager (Mitaka USA, Inc.). Lymphatic function, and the severity and distribution of the dermal backflow, were evaluated and staged using the ICG Fluorescent Lymphography Staging Scale (FLSS).39
Response to conservative or physiological surgical intervention
Changes in the l-Dex ratio and LVC were compared at baseline consultation, and again preoperatively for patients requiring intensive complete decongestive therapy (CDT) for presurgical optimization to reduce the pitting edema/extracellular fluid. Changes in the l-Dex ratio and LVC were compared preoperatively and at 6 months postoperatively for patients that underwent physiological surgeries including LVB and vascularized lymph node transfer.
Statistical analysis
Face validity pertains to the l-Dex BIS appearing to measure clinical lymphedema through correlation with limb volume and pitting edema. Criterion validity pertains to its correlation with established measures of physiological function and staging systems, radioisotope lymphoscintography, and ICG fluorescent lymphography. Spearman's correlation coefficients (ρ), were calculated to measure the correlations between evaluation methods; a correlation coefficient of 0.3–0.49 is considered a low correlation, 0.5–0.69 a moderate correlation, and 0.7 or more a strong correlation44; p-values were calculated. Change in l-Dex ratio was calculated as for LVC. Analyses were performed in SAS 9.3 (SAS Institute, Inc., Cary, NC) and R 3.0.2 (The R Foundation for Statistical Computing).
Validity
Face validity was evaluated by comparing l-Dex BIS to clinical limb volume measurements using perometry and clinical assessment of the degree of pitting edema. Construct validity was evaluated by determining the response of l-Dex BIS to conservative and surgical interventions. Criterion validity was evaluated by comparing l-Dex BIS to measures of physiological function of the lymphatic system using radioisotope lymphoscintography and ICG fluorescent lymphography.
Results
The study included 26 patients, with 70 sets of evaluations. All patients were diagnosed with unilateral lymphedema secondary to surgery for cancer. All 21 patients with upper extremity involvement had lymphedema secondary breast cancer treatment; 13 patients underwent mastectomy, and 8 segmental mastectomy. All of these patients underwent axillary lymphadenectomy, radiation, and chemotherapy; 19 patients received regional nodal irradiation. Among the five patients with lower extremity lymphedema, etiologies included radical hysterectomy, radical prostatectomy, and abdominoperineal resection, all with pelvic lymph node dissection. Mean age was 50.8 years (±11.8) and mean duration of lymphedema was 57.9 months (±81.7). Mean body mass index was 30.1 kg/m2 (±4.6).
For upper extremities, the mean baseline volume of the affected extremity was 2397.2 mL (±580.8), the mean volume of the unaffected extremity was 2096.8 cc (±389.1), and the mean LVD was 300.3 mL (±287.8) (mean 13.7% ± 10.9) and mean LVR 1.1 (±0.1). For lower extremities, the mean baseline volume of the affected extremity was 9687.8 mL (±1663.0), the mean volume of the unaffected extremity was 7689.7 mL (±539.7), and the mean LVD was 1998.1 mL (±1126.5) (mean 25.3% ± 12.4) and mean LVR 1.3 (±0.1). At baseline the mean impedance at R0 using BIS of the affected extremity was 286.0 (±64.3), and of the unaffected extremity was 332.5 (±50.4); the unadjusted mean ratio was 1.2 (±0.2). The corresponding mean l-Dex ratio was 17.2 (±15.0).
LVR correlated significantly with the TI, but not with ICG staging or degree of pitting edema (Table 1). Duration of lymphedema was significantly associated with LVR (ρ = 0.48; p = 0.001), l-Dex ratio (ρ = 0.57; p < 0.001), ICG staging (ρ = 0.63; p < 0.001), and TI (ρ = 0.48; p = 0.001), but not with degree of pitting edema (ρ = 0.17; p > 0.05). Although all l-Dex BIS metrics correlated significantly with each of these measures, the l-Dex ratio correlated most closely for all measures, (ρ = 0.71–0.94, p < 0.0001) (Table 1).
Spearman's Correlation Coefficients (ρ) Between Measured Variables
l-Dex ratio
Limb volume ratio using perometry
Ratio of unaffected/affected impedances at R0 using l-Dex
Absolute difference in impedances at R0 using l-Dex
Limb volume ratio (LVR) using perometry
0.71 (p = 0)
—
0.63 (p = 0)
0.61 (p = 0.00001)
Staging using ICG Fluorescent lymphography
0.46 (p = 0.002)
0.26 (p > 0.05)
0.37 (p = 0.01)
0.36 (p = 0.016)
Transport index using lymphoscintigraphy
0.48 (p = 0.001)
0.43 (p = 0.004)
0.34 (p = 0.02)
0.35 (p = 0.02)
Clinical evaluation of degree of pitting edema
0.41 (p = 0.005)
0.19 (p > 0.05)
0.38 (p = 0.01)
0.39 (p = 0.0084)
l-Dex ratio
-
0.71 (p = 0)
0.94 (p = 0)
0.91 (p = 0)
ICG, indocyanine green.
Regarding face validity, there were significant clinical correlations between the l-Dex ratio and LVR (Fig. 2), and degree of pitting edema (Fig. 3). For criterion validity, there were significant correlations with physiologic TI (Fig. 4) and ICG staging (Fig. 5). Eight patients underwent CDT to reduce pitting edema before surgical intervention. In these patients the mean reduction in limb volume was 13.8%, whereas the mean decrease in the l-Dex ratio was 48.3% (p = 0.061), with no significant correlation between these (ρ = 0.19; p = 0.65). Ten patients underwent physiological surgical intervention for their lymphedema and maintained compliance at 6 months postoperatively; mean limb volume reduction was 25.2% and the corresponding l-Dex ratio decreased on average by 36.1% (p = 0.067), however, these were not significantly related (ρ = 0.38; p = 0.27).
Correlation between lymphedema index using l-Dex bioimpedance spectroscopy and limb volume ratio using perometry. Linear trendline is shown.
Box plot demonstrating the correlations between the l-Dex ratio and grade of pitting edema on clinical evaluation.
Box plot demonstrating the correlations between the l-Dex ratio and lymphedema transport index using technetium-99m sulfur colloid lymphoscintigraphy.
Box plot demonstrating the correlations between the l-Dex ratio and lymphedema stage using indocyanine green fluorescent lymphography.
Staging using the LSS significantly correlated with the TI (ρ = 0.69; p < 0.001) and ICG staging (ρ = 0.66; p < 0.001). All patients with no lymphatic transit and with no lymph nodes visualized on radionuclide lymphoscintigraphy had ICG FLSS stage IV lymphedema, with continuous dermal backflow from the hand proximally.
Discussion
Diagnosis, staging, and longitudinal surveillance of lymphedema remains challenging due to the often poor correlation between clinical examination findings and physiological lymphatic function, and issues of reliability and validity of the measurement tools currently available. This study compared BIS measurements using the l-Dex with limb volume, measures of lymphatic function, and response to intervention in patients with early and chronic lymphedema of the upper or lower extremities, and has found the following: First, the l-Dex ratio demonstrated face, construct, and criterion validity; it correlated significantly with all measures, including a strong correlation with LVR using perometry (ρ = 0.71; p < 0.001). Second, the l-Dex ratio correlated more closely with all measures than both the unadjusted ratio and the absolute differences in the impedance at R0 between the affected and unaffected extremities. Third, LVR using perometry correlated with the TI using lymphoscintigraphy, but not with staging using ICG fluorescent lymphography. Fourth, following nonsurgical or surgical intervention, there were no significant correlations between the reduction in the l-Dex ratio and limb volume. Finally, the LSS correlated closely with both the TI using lymphoscintigraphy (ρ = 0.69; p = 0) and staging using ICG lymphography (ρ = 0.66; p = 0).
The l-Dex allows measurement of the extracellular water within an extremity, and in patients with unilateral lymphedema, the difference in extracellular water between the affected and unaffected extremities can be used to measure the severity of the lymphedema.11–13 This can be represented as the absolute difference between the impedances, the unadjusted ratios between these, or an adjusted ratio: the l-Dex ratio. There is disagreement as to which of these measures is most useful for diagnosis and longitudinal evaluation of lymphedema. In this study, the l-Dex ratio significantly correlated with all measures, most closely with LVR using perometry,11–13 and the correlations were higher than for the other measures. The results of this study suggest that the l-Dex ratio is the most accurate metric of the three for evaluating lymphedema, with the adjustments for sex, upper/lower limb and right/left dominance inherent in the calculation improving all correlations when compared with the unadjusted ratio.
Limb volume measurement is the most commonly used modality for diagnosing and monitoring lymphedema, for which the perometer is widely used. Interestingly, this study found that LVR using perometry correlated significantly with only two of the measures, and following conservative and surgical interventions the l-Dex ratio was more responsive to change than LVC measured using perometry. Taken together, these results demonstrate that the l-Dex ratio correlates with limb volume and measures of lymphatic function, and should be used together with limb volume measurement for longitundinal monitoring of lymphedema, in particular when evaluating the responses to conservative and surgical interventions.45
This study has the following limitations: First, all analysis are retrospective, though data were obtained from a prospectively maintained database. Second, the majority of patients, and all included upper extremity cases, were secondary to breast cancer treatment. Further, data were obtained from a single surgeon; results may therefore not be generalizable to all forms of lymphedema and all practice settings. Finally, construct validity was limited to concurrent validity, where l-Dex BIS was correlated to other existing measures; future study will analyze its predictive validity and association with patient-reported outcome measures.
Conclusions
The l-Dex ratio correlated with limb volume and clinical assessment of pitting edema, and physiologic measures of lymphatic function, and demonstrated face, construct, and criterion validity in response to intervention. These findings support the adjunctive use of the l-Dex ratio with limb volume measurements for objective diagnosis, evaluation of lymphedema severity, longitudinal serial evaluation of lymphedema, and response to conservative and surgical interventions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
1.
MoffattCJ. Lymphoedema: An underestimated health problem. QJM, 2003; 96:731–738.
2.
RocksonSG. Estimating the population burden of lymphedema. Ann N Y Acad Sci, 2008; 1131:147–154.
3.
ShaitelmanSF, ChiangYJ, GriffinKD, DeSnyderSM, SmithBD, SchaverienMV, WoodwardWA, CormierJN. Radiation therapy targets and the risk of breast cancer-related lymphedema: A systematic review and network meta-analysis. Breast Cancer Res Treat, 2016; 162:201–215.
4.
CormierJN, AskewRL, MungovanKS, XingY, RossMI, ArmerJM. Lymphedema beyond breast cancer: A systematic review and meta-analysis of cancer-related secondary lymphedema. Cancer, 2010; 116:5138–5149.
5.
VossRK, CromwellKD, ChiangYJ, ArmerJM, RossMI, LeeJE, GershenwaldJE, StewartBR, ShaitelmanSF, CormierJN. The long-term risk of upper-extremity lymphedema is two-fold higher in breast cancer patients than in melanoma patients. J Surg Oncol, 2015; 112:834–840.
6.
MiharaM, HaraH, HayashiY, NarushimaM, YamamotoT, TodokoroT, IidaT, SawamotoN, ArakiJ, KikuchiK, MuraiN, OkitsuT, KisuI, KoshimaI. Pathological steps of cancer-related lymphedema: Histological changes in the collecting lymphatic vessels after lymphadenectomy. PLoS One, 2012; 7:41126.
7.
ZampellJC, YanA, ElhadadS, AvrahamT, WeitmanE, MehraraBJ. CD4+ cells regulate fibrosis and lymphangiogenesis in response to lymphatic fluid stasis. PLoS One, 2012; 7:49940.
8.
AvrahamT, DaluvoyS, ZampellJ, YanA, HavivYS, RocksonSG, MehraraBJ. Blockade of transforming growth factor-beta1 accelerates lymphatic regeneration during wound repair. Am J Pathol, 2010; 177:3202–3214.
9.
LeeMJ, BolandRA, CzerniecS, KilbreathSL. Reliability and concurrent validity of the perometer for measuring hand volume in women with and without lymphedema. Lymphat Res Biol, 2011; 9:13–18.
10.
SpechtMC, MillerCL, RussellTA, HorickN, SkolnyMN, O'TooleJA, JammalloLS, NiemierkoA, SadekBT, ShenoudaMN, FinkelsteinDM, SmithBL, TaghianAG. Defining a threshold for intervention in breast cancer-related lymphedema: What level of arm volume increase predicts progression?. Breast Cancer Res Treat, 2013; 140:485–494.
11.
AdriaenssensN, BuylR, LievensP, FontaineC, LamoteJ. Comparative study between mobile infrared optoelectronic volumetry with a Perometer and two commonly used methods for the evaluation of arm volume in patients with breast cancer related lymphedema of the arm. Lymphology, 2013; 46:132–143.
12.
BundredNJ, StocktonC, KeeleyV, RichesK, AshcroftL, EvansA, SkeneA, PurushothamA, BramleyM, HodgkissT; Investigators of BEA/PLACE studies. Comparison of multi-frequency bioimpedance with perometry for the early detection and intervention of lymphoedema after axillary node clearance for breast cancer. Breast Cancer Res Treat, 2015; 151:121–129.
13.
JainMS, DanoffJV, PaulSM. Correlation between bioelectrical spectroscopy and perometry in assessment of upper extremity swelling. Lymphology, 2010; 43:85–94.
14.
WardLC, DylkeE, CzerniecS, IsenringE, KilbreathSL. Confirmation of the reference impedance ratios used for assessment of breast cancer-related lymphedema by bioelectrical impedance spectroscopy. Lymphat Res Biol, 2011; 9:47–51.
15.
BarrioAV, EatonA, FrazierTG. A prospective validation study of bioimpedance with volume displacement in early-stage breast cancer patients at risk for lymphedema. Ann Surg Oncol, 2015; 22:370–375.
16.
WardLC, CzerniecS, KilbreathSL. Quantitative bioimpedance spectroscopy for the assessment of lymphoedema. Breast Cancer Res Treat, 2009; 117:541–547.
17.
SoranA, OzmenT, McGuireKP, DiegoEJ, McAuliffePF, BonaventuraM, AhrendtGM, DeGoreL, JohnsonR. The importance of detection of subclinical lymphedema for the prevention of breast cancer-related clinical lymphedema after axillary lymph node dissection; a prospective observational study. Lymphat Res Biol, 2014; 12:289–294.
18.
FuMR, ClelandCM, GuthAA, KayalM, HaberJ, CartwrightF, KleinmanR, KangY, ScagliolaJ, AxelrodD. L-Dex ratio in detecting breast cancer-related lymphedema: Reliability, sensitivity, and specificity. Lymphology, 2013; 46:85–96.
19.
ShahC, ArthurDW, WazerD, KhanA, RidnerS, ViciniF. The impact of early detection and intervention of breast cancer-related lymphedema: A systematic review. Cancer Med. 2016; 5:1154–1162.
20.
ViciniF, ShahC, LydenM, WhitworthP. Bioelectrical impedance for detecting and monitoring patients for the development of upper limb lymphedema in the clinic. Clin Breast Cancer, 2012; 12:133–137.
21.
ShahC, ViciniF, BeitschP, LaidleyA, AnglinB, RidnerSH, LydenM. The use of bioimpedance spectroscopy to monitor therapeutic intervention in patients treated for breast cancer related lymphedema. Lymphology, 2013; 46:184–192.
22.
ChoiYH, SeoKS. Correlation among bioimpedance analysis, sonographic and circumferential measurement in assessment of breast cancer-related arm lymphedema. Lymphology, 2014; 47:123–133.
23.
WardLC, CzerniecS, KilbreathSL. Operational equivalence of bioimpedance indices and perometry for the assessment of unilateral arm lymphedema. Lymphat Res Biol, 2009; 7:81–85.
24.
DylkeES, WardLC, MeerkinJD, NeryL, KilbreathSL. Tissue composition changes and secondary lymphedema. Lymphat Res Biol, 2013; 11:211–218.
25.
KleinhansE, BaumeisterRG, HahnD, et al.Evaluation of transport kinetics in lymphoscintigraphy: Follow-up study in patients with transplanted lymphatic vessels. Eur J Nucl Med, 1985; 10:349–352.
26.
WeissM, BaumeisterRG, HahnK. Post-therapeutic lymphedema: Scintigraphy before and after autologous lymph vessel transplantation: 8 years of long-term followup. Clin Nucl Med, 2002; 27:788–792.
27.
MaclellanRA, ZurakowskiD, VossS, GreeneAK. Correlation between lymphedema disease severity and lymphoscintigraphic findings: A clinical-radiologic study. J Am Coll Surg, 2017; 225:366–370.
28.
MikamiT, HosonoM, YabukiY, YamamotoY, YasumuraK, SawadaH, ShizukuishiK, MaegawaJ. Classification of lymphoscintigraphy and relevance to surgical indication for lymphaticovenous anastomosis in upper limb lymphedema. Lymphology, 2011; 44:155–167.
29.
AkitaS, MitsukawaN, KazamaT, KuriyamaM, KubotaY, OmoriN, KoizumiT, KosakaK, UnoT, SatohK. Comparison of lymphoscintigraphy and indocyanine green lymphography for the diagnosis of extremity lymphoedema. J Plast Reconstr Aesthet Surg, 2013; 66:792–798.
30.
SzubaA, StraussW, SirsikarSP, RocksonSG. Quantitative radionuclide lymphoscintigraphy predicts outcome of manual lymphatic therapy in breast cancer-related lymphedema of the upper extremity. Nucl Med Commun, 2002; 23:1171–1175.
31.
PeckingAP, AlbériniJL, WartskiM, EdelineV, CluzanRV. Relationship between lymphoscintigraphy and clinical findings in lower limb lymphedema (LO): Toward a comprehensive staging. Lymphology, 2008; 41:1–10.
32.
YuanZ, ChenL, LuoQ, ZhuJ, LuH, ZhuR. The role of radionuclide lymphoscintigraphy in extremity lymphedema. Ann Nucl Med, 2006; 20:341–344.
33.
GoluekePJ, MontgomeryRA, PetronisJD, MinkenSL, PerlerBA, WilliamsGM. Lymphoscintigraphy to confirm the clinical diagnosis of lymphedema. J Vasc Surg, 1989; 10:306–312.
34.
MiharaM, HaraH, ArakiJ, KikuchiK, NarushimaM, YamamotoT, IidaT, YoshimatsuH, MuraiN, MitsuiK, OkitsuT, KoshimaI. Indocyanine green (ICG) lymphography is superior to lymphoscintigraphy for diagnostic imaging of early lymphedema of the upper limbs. PLoS One, 2012; 7:38182.
35.
HaraH, MiharaM, SekiY, TodokoroT, IidaT, KoshimaI. Comparison of indocyanine green lymphographic findings with the conditions of collecting lymphatic vessels of limbs in patients with lymphedema. Plast Reconstr Surg, 2013; 132:1612–1618.
36.
YamamotoT, YamamotoN, DoiK, OshimaA, YoshimatsuH, TodokoroT, OgataF, MiharaM, NarushimaM, IidaT, KoshimaI. Indocyanine green-enhanced lymphography for upper extremity lymphedema: A novel severity staging system using dermal backflow patterns. Plast Reconstr Surg, 2011; 128:941–947.
37.
NarushimaM, YamamotoT, OgataF, YoshimatsuH, MiharaM, KoshimaI. Indocyanine green lymphography findings in limb lymphedema. J Reconstr Microsurg, 2016; 32:72–79.
38.
YamamotoT, NarushimaM, YoshimatsuH, YamamotoN, KikuchiK, TodokoroT, IidaT, KoshimaI. Dynamic indocyanine green (ICG) lymphography for breast cancer-related arm lymphedema. Ann Plast Surg, 2014; 73:706–709.
39.
ChangDW, SuamiH, SkorackiR. A prospective analysis of 100 consecutive lymphovenous bypass cases for treatment of extremity lymphedema. Plast Reconstr Surg, 2013; 132:1305–1314.
40.
SmootBJ, WongJF, DoddMJ. Comparison of diagnostic accuracy of clinical measures of breast cancer-related lymphedema: Area under the curve. Arch Phys Med Rehabil, 2011; 92:603–610.
41.
CzerniecSA, WardLC, RefshaugeKM, BeithJ, LeeMJ, YorkS, KilbreathSL. Assessment of breast cancer-related arm lymphedema—comparison of physical measurement methods and self-report. Cancer Invest, 2010; 28:54–62.
42.
SeidelHM, BallJW, DainsJE, BenedictGW. Heart and blood vessels. In: SchreferS, ed. Mosby's Guide to Physical Examination, 3rd ed. St. Louis, MO: Mosby; 1995:419.
43.
BrodoviczKG, McNaughtonK, UemuraN, MeiningerG, GirmanCJ, YaleSH. Reliability and feasibility of methods to quantitatively assess peripheral edema. Clin Med Res, 2009; 7:21–31.
44.
HinkleDE, WiersmaW, JursSG. Applied Statistics for the Behavioral Sciences. 5th ed. Boston, MA: Houghton Mifflin; 2003.
45.
DylkeES, SchembriGP, BaileyDL, BaileyE, WardLC, RefshaugeK, BeithJ, BlackD, KilbreathSL. Diagnosis of upper limb lymphoedema: Development of an evidence based approach. Acta Oncol, 2016; 55:1477–1483.