
Abstract
Background:
The aim of this study was to investigate the Turkish adaptation, validity, and reliability of the Patient Benefit Index-Lymphedema (PBI-L) ensuring direct assessment of the benefit in patients with lymphedema (LE), lipedema, and lipolymphedema.
Methods and Results:
Eighty-one patients who were consulted for physiotherapy, whose diagnoses were LE, lipedema, and lipolymphedema, and who were treated or planned to be treated for these diagnoses, were included in this study. PBI-L was adapted to Turkish by considering the stages of the cultural adaptation process. Short Form-36 (SF-36) was applied for the validity of PBI-L. PBI-L was repeated after a 1-week interval for test–retest reliability. The mean age was 47.66 ± 14.23 years. The intraclass correlation coefficient (ICC) value was determined as 0.73 (p < 0.0001) for the total score. There was a moderate correlation between first (ICC = 0.63, p < 0.0001) and second subdimensions (ICC = 0.62, p < 0.0001). Cronbach's α values ranged between 0.83 and 0.89. Low correlations were found between total scores of PBI-L and mental health, physical function subdimensions of SF-36 (p < 0.05). The Kaiser Meyer Olkin value was 0.6, and it was found that the PBI-L was not consistent with factor analysis.
Conclusion:
The Turkish version of PBI-L is a valid and reliable tool in patients with LE, lipedema, and lipolymphedema. However, the reassessment validity of PBI-L would be suggested by using an LE-specific quality of life questionnaire.
Introduction
Lymphedema (LE) is a chronic disease characterized by the increase of tissue volume due to the accumulation of protein-rich fluid in the interstitial space and the development of adipose tissue and fibrosis as a result of inadequate functioning of the lymphatic system.1,2 LE is classified as primary or secondary. 3 LE is a chronic progressive disease with serious psychosocial and physical symptoms. 4 Some problems associated with LE are heaviness, tension, increase in extremity temperature, tingling sensation, limitations due to edema, pain, difficulty walking, and puffiness.5,6 Anxiety, depression, body image issues, lack of social confidence, sexuality, and economic concerns are the most frequently seen psychosocial problems.7,8 These symptoms and limitations affect quality of life (QoL) unfavorably.9,10
Health-related QoL (HRQoL) is the optimum state of social function, health perception, vitality, life satisfaction, and wellness that consists of mental and physical (workplace, parent, caretaker, etc.) role relationships. HRQoL measurement is crucial to assess the effect of chronic diseases on patients. Although two patients may have the same sign and symptoms, their role functions or emotional wellness states may be different from each other. 11
HRQoL questionnaires are used generally to assess QoL in clinics. General HRQoL questionnaires assess the effects of the treatment on QoL. 12 The disease-specific HRQoL should be preferred when determining the effect of the treatment of a specific chronic disease on the individual's QoL, since it is more sensitive and distinctive than general HRQoL questionnaires. 13 Both of these HRQoL types assess treatment outcomes from an indirect way. Hence, more specific methods excluding external factors were needed to assess the treatment results and the patient benefit received from the treatment.
Patient Benefit Index-Lymphedema (PBI-L) is a questionnaire used for patients diagnosed with upper and lower limb LE, lipedema, and lipolymphedema. It measures the significance of the treatment goals of these patients and the benefit level received from the treatment directly and objectively. 14
It is important to determine patients' treatment goals and benefits from their perspectives. Other factors affecting the QoL except from treatment should be excluded for direct assessment of benefit from treatment. 14 Although some disease-specific HRQoL questionnaires exist, there is no patient-reported outcome specific to the disease that directly assesses the benefit of treatment in LE patients, either developed in Turkish or adapted. The purpose of this study was to investigate the Turkish adaptation, validity, and reliability of PBI-L.
Materials and Methods
Permission was received on March 11, 2014 with the serial number of 77082166-604.01.02-6848 from the Gazi University Clinic Research Ethical Committee. Information was provided about the study and informed consent was obtained from voluntary participants.
Patients who were referred to the Bolu Abant Izzet Baysal University, Faculty of Health Sciences, Department of Physiotherapy and the Gazi University Faculty of Health Sciences Department of Physiotherapy and Rehabilitation for physiotherapy advices and applications for LE, lipedema, and LE diagnoses were informed about the study. The inclusion criteria were 18–75 years old; diagnosed with LE, lipedema, or lipolymphedema by a doctor; and have been treated or planned to be treated for these diagnoses. Patients who had chronic venous insufficiency, edema caused by organ failures (heart, kidney, lung, etc.), trauma-based and undiagnosed edema, cooperation and communication problems, illiterate, or unable to speak Turkish were excluded.
The study started with 102 patients. A total of 21 patients left the study. Six of them did not participate in the second assessment, and 15 of them did not want to be treated or did not come for the treatment. Therefore, this study was completed with 81 patients (Fig. 1).
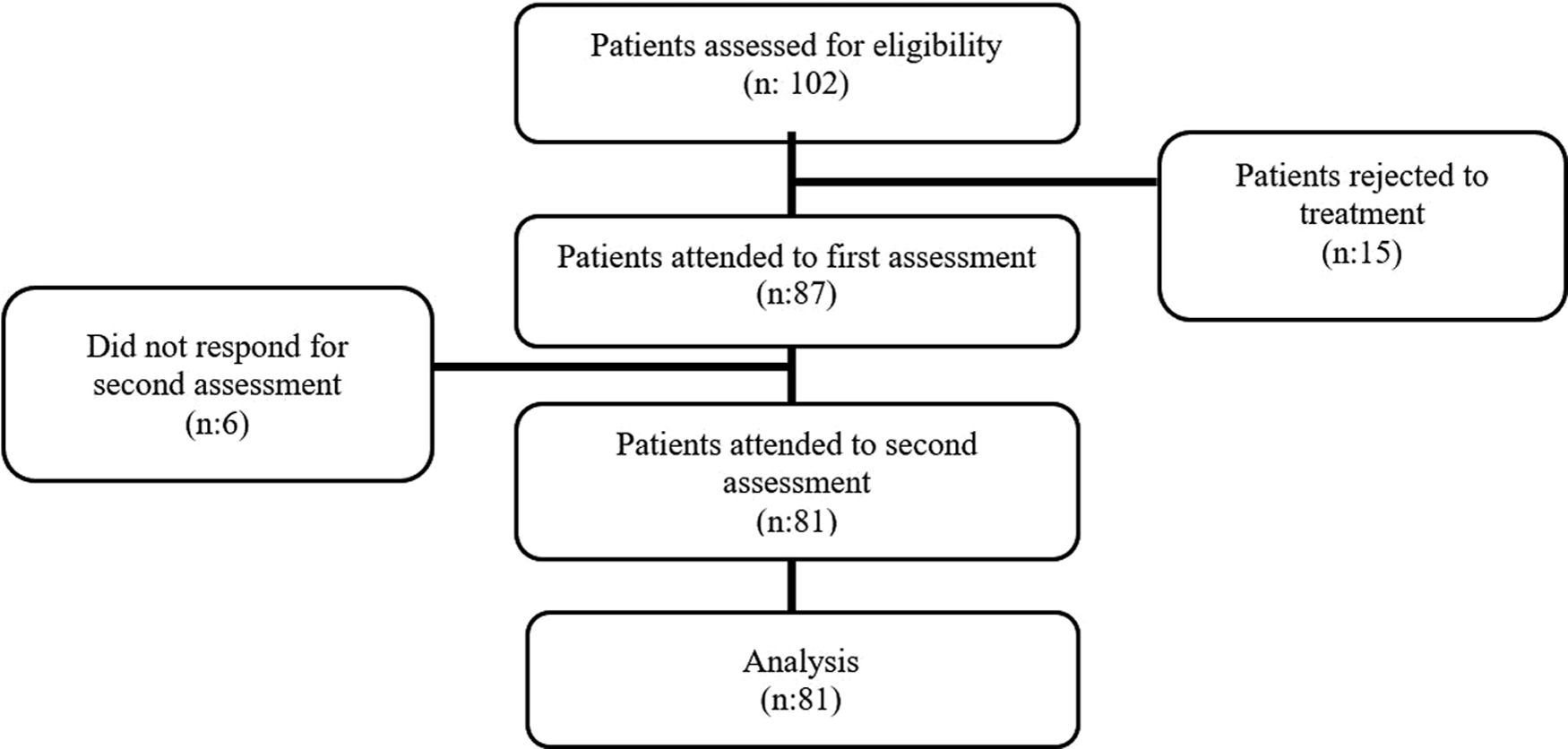
Flow chart of study.
Sociodemographic data were recorded. Patients were assessed by using the Visual Analogue Scale (VAS), Short Form-36 (SF-36), and PBI-L. The VAS was used to assess the level of the quality of treatment, satisfaction with treatment, general health condition, and disease-specific health status. A 10 cm line was drawn for the VAS assessment. It was considered that the beginning of the line was “very bad” and the end of the line was “very good.” The patients were asked to answer the questions about satisfaction with treatment, quality of care, general and disease-specific health conditions, and to mark the answer on the line. SF-36 was used to assess general HRQoL. SF-36 has a general characteristic among the QoL scales and provides multiple measurements. 15 The validity and reliability of the Turkish version were carried out by Kocyigit et al. 16 The major characteristic of SF-36 is a self-reported scale. The advantages of the scale are to be completed in a short period such as 5 minutes, and it allows responses not only for the positive aspects of health status but also for the negative aspects. 17 The scale consists of 8 dimensions and 36 items. These dimensions are physical function (10 items), social function (2 items), role limitations based on physical functions (4 items), role limitations based on emotional problems (3 items), mental health (5 items), energy vitality (4 items), pain (2 items), and general health perception (5 items). Each subdimension is estimated out of 100 points. Higher scores indicate better QoL. 16
Blome et al. 14 developed PBI-L to assess the efficiency of the treatment target and the benefit of the treatment directly in patients with LE. PBI-L consists of two subquestionnaires and two subdimensions. The first subdimension consists of 14 items and assesses the activities of daily life and psychological wellness. The second subdimension consists of nine items and assesses physical wellness status and abilities.
The first subquestionnaire of PBI-L is the Patients Needs Questionnaire (PNQ) questioning why the patient needs a treatment, and it consists of 23 items. The patients scored their own treatment needs in order of importance from (0) “not at all,” (1) “somewhat,” (2) “moderately,” (3) “quite,” to (4) “very.”
The second subquestionnaire of PBI-L is the Patient Benefit Questionnaire (PBQ). The same 23 items are scored as (0) “not at all,” (1) “somewhat” beneficial, (2) “moderately” beneficial, (3) “quite” beneficial, and (4) “very” beneficial. Furthermore, the patients could also mark an item as “doesn't apply to me” in both two subquestionnaires if the items were not applicable for them. PBI-L total score and subdimensions scores were calculated through the formulation shown in Figure 2. Possible scores range between “0” and “4.” “0” is the lowest score and means that the treatment is not beneficial. “4” means treatment is very beneficial for the patient. Sociodemographic assessment forms VAS and SF-36 were applied once, and PBI-L was applied twice with a 1-week interval.

Algorithm of the computation PBI-L benefit value with k preference items of Patient Need Questionnaire and Patient Benefit Questionnaire. PBI-L, Patient Benefit Index-Lymphedema.
Translation
The protocol of Beaton et al. 18 was applied for the Turkish adaptation process of PBI-L. The first stage of the translation was to translate the original language (German) to the target language (Turkish). Three translators (T1, T2, and T3), who were unaware of each other, spoke two languages, did not see the questionnaire previously, and whose native language was the target language, translated the PBI-L from German to Turkish. T1, a physiotherapist, had command of the medical terms used in the content of the questionnaire. T2 and T3 did not have a medical or professional background concerned with the PBI-L. Inadequate terms and expressions were determined in the PBI-L generated by the three translators independently. The most appropriate words were selected. The translations of PBI-L were synthesized so that a single and mutual index was generated.
According to the original protocol, PBI-L was translated from Turkish to German again by two translators (T4 and T5) who did not have any knowledge of PBI-L. This process was continued by checking whether the questionnaire reflected the content in the original version. At this stage, the final assessment was carried out by all translators to ensure cultural equivalency and to minimize the difference between the target language and the source language. Synonyms, difficulties with idioms, grammar, and usage of the words fitting the lifestyle of the target culture were discussed, and the final state of PBI-L was achieved before the pilot study.
The final PBI-L was applied to 30 patients as a pilot study. Participants were asked whether they had any difficulty understanding. Unclear items were explained and repeated. All cultural adaptation procedures were completed, corrections were made, and the final state of the Turkish version of PBI-L was generated subsequently.
All of the translations and the final state of PBI-L were forwarded to the author who developed the questionnaire and was informed about the translation process.
Two separate applications under the same conditions were carried out on all patients for this purpose. The period between two measurements was determined as 1 week. This duration should be long enough to prevent them from remembering substantially; however, it should be short enough to not allow occurrence of changes that were measured.
General physiotherapy approaches for LE were applied to patients who participated in the study, since the questionnaire assesses treatment goals and benefits. Physiotherapy approaches consisted of one or several of the applications of self-drainage, exercise, compression socks, complex decongestive physiotherapy, and pneumatic compression devices. Moreover, patient education was added to treatments.
The application was carried out as given hereunder since the questionnaire consists of two subquestionnaires.
PNQ, which is the first subquestionnaire of PBI-L, was applied to patients before starting a treatment to assess their needs. It was repeated 1 week later. At the end of the treatment, PBQ, which is the second subquestionnaire of PBI-L, was applied to assess the benefits of treatment.
In patients who had received a treatment previously, PNQ and PBQ subquestionnaires (whole PBI-L) were applied. Both subquestionnaires were applied 1 week later.
Data analysis
The SPSS (version 18.0) program was used for the estimations. The descriptive statistics on the categorical and numerical variables were given as numbers, percentages, mean, and standard deviations, respectively.
The internal consistency was assessed by Cronbach's α. The test–retest reliability was assessed by intraclass correlation coefficient (ICC). The correlation between sociodemographic and clinic properties, VAS scores, subdimensions of SF-36, and PBI-L scores were analyzed by Spearman rank correlation analysis. The Kaiser Meyer Olkin (KMO) statistic was used to determine whether the questionnaire data set could be factored. p < 0.05 was accepted as significant.
Results
A total of 81 patients diagnosed with LE, lipedema, and lipolymphedema participated in this study. The mean age, height, weight, and BMI of the patients were 47.66 ± 14.23 years, 163.79 ± 9.54 cm, 80.26 ± 23.99 kg, and 30 ± 8.43 kg/m2, respectively.
Educational status, occupation, dominant limbs, disease stage, affected areas, edema localization, and duration of disease are given in Table 1.
Sociodemographic Features of Patients
Considering PBI-L score distributions, in the first applied PBI-L, two patients (2.4%) received 0 points, which was the lowest score; eight patients (9.9%) received 4 points, which was the highest score. The mean PBI-L score was 2.25 ± 0.71. In the second applied PBI-L, two patients (2.4%) received 0 points, which was the lowest score; five patients (6.2%) received 4 points, which was the highest score. The mean PBI-L score was 2.88 ± 0.6.
Reliability
Internal consistency of PBI-L was high. Chronbach's α values of PBI-L are given in Table 2.
Internal Consistency of Patient Benefit Index-Lymphedema
The results of test–retest analysis showed moderate correlation between the total score of PBI-L (ICC = 0.73, p < 0.0001). There was moderate correlation between the first and second subdimensions (ICC = 0.63, p < 0.0001, ICC = 0.62, p < 0.0001).
Validity
PBI-L subdimension scores, total score, and the correlation values between the subdimensions of SF-36 are given in Table 3. A low negative correlation was found between the total scores of PBI-L and mental health (r = −0.24, p = 0.03) and the physical function (r = −0.25, p = 0.02) subdimensions of SF-36.
The Relationship Between Patient Benefit Index-Lymphedema Subdimension Scores, Total Score, and Short Form-36 Subdimension Scores
p < 0.05.
Values in bold were calculated with Spearman's rank correlation coefficient.
r, Spearman's rank correlation coefficient.
There was no correlation detected between general health condition, disease-specific health status, quality of treatment, satisfaction with the treatment, and PBI-L (p > 0.05). Correlation between PBI-L subdimensions and some parameters is given in Table 4. There was a positive correlation obtained between satisfaction with the treatment and quality of treatment (r = 0.75, p < 0.05)
The Relationship Between the General Health Condition, Disease-Specific Health Status, Quality of Treatment, Satisfaction with the Treatment, and Patient Benefit Index-L Subdimensions
p < 0.05.
Values in bold were calculated with Spearman's rank correlation coefficient.
min, minimum; max, maximum; SD, standard deviation; VAS, Visual Analogue Scale; r, Spearman's rank correlation coefficient.
A factor analysis was not conducted since the KMO value of this study was 0.60. Because according to the KMO test, the values <0.60 were explained as “miserable,” values between 0.60 and 0.70 were “mediocre,” values between 0.70 and 0.80 were “middling,” values between 0.80 and 0.90 were “meritorious,” and values between 0.90 and 1 were explained as “marvelous,” and it stated that the data set could not be factored. 19
Conclusions
This study has demonstrated that the Turkish version of PBI-L is a valid and reliable tool that objectively assesses treatment goals and treatment benefits of patients with LE, lipedema, and lipolymphedema. PBI-L is the first and only Turkish questionnaire directly measuring the benefit gained according to the patients' perspective.
Patient's perspective started to gain importance for the assessment of treatment criteria and the requirement for considering the benefits and gains of treating the indemnity of medication or medical spending during recent years in many countries. The criteria related to the patients have been considered in their payments. 20 However, until recently, the benefit of the treatment as assessed by the patient was being ignored in clinical research. The gains of the patient and how they benefited from the treatment were being assessed by health professionals. 21 However, the benefit received from the treatment must absolutely be asked to the patient since there may be a difference between the physician and patient assessments. 20 The methodology of PBI-L presents the gained benefit from the patient perspective objectively.
HRQoL questionnaires are appropriate to assess the benefits defined by the patient and need to be based on self-report. In particular, disease-specific HRQoL questionnaires have become important since they reflect the effects of the disease and treatment on daily life activities. 22 There are numerous questionnaires in the literature assessing disease-specific HRQoL in patients diagnosed with LE.23–30 However, a general disadvantage of these questionnaires is that they cannot assess the treatment purposes that are crucial for the patient, despite the sustainment of patient perspective. 20 Patients generally benefit from a treatment fulfilling their individual needs. Patient's priorities are important for treatment plans. Treatments that cannot meet the expectation are generally in the second plan. Nevertheless, combining the treatment outcomes and patient preferences is extremely important for the assessment of the effectiveness of the treatment. 31 PNQ, which is the subquestionnaire of PBI-L, measures objectively what symptoms are important for the patient. Moreover PBQ, which is the other subquestionnaire of PBI-L measures how much effective these treatment is on symptoms. This questionnaire enables the assessment of disease-specific symptoms clearly. It is an important advantage that PBI-L can be used in various clinical groups, including lipedema, lipolymphedema, and primary and secondary LE in upper and lower extremities.
The internal consistency values of the Turkish version of PBI-L ranged between 0.83 and 0.89. Blome et al. 14 reported that PBI-L's Cronbach's α value was >0.8. Similarly, we also found that subdimensions and the total PBI-L had high reliability.
Medium correlation between test and retest results was interpreted as the preference difficulty that was effected by considering the sociocultural states (48% of patients were primary school graduates) of the patients between the two middle neighboring items. In addition to this, application of the questionnaires by two different methods may have been the reason for differences. For example, patients may have marked concerned items at the beginning as “quite” before the treatment. After 1 week, the patient may have marked this item as “moderately” if he or she had sufficient improvement with regard to the concerned item. Perhaps more consistent outcomes could have been obtained if the treatment had not been applied during the 1-week period. Moreover, the PBI-L was applied retrospectively to patients who were treated previously. Patients answered the questionnaire about their past treatment experience. They might not have remembered their condition in the first and second applications of PBI-L. Nevertheless, according to the reliability results of the test–retest between the total scores of the questionnaire, the consistency level was found as good. Blome et al. 14 did not evaluate the test–retest reliability of PBI-L. Differing from Blome et al., the reliability of the test–retest of the Turkish version was carried out in this study.
SF-36, which is a HRQoL questionnaire, was used to determine validity of PBI-L. Moreover, it has been reported that the usage of SF-36 on LE patients was more appropriate than usage of Nottingham Health Profile (NHP). In the literature, it was stated that the NHP could not assess the changes and symptoms that are associated with limb volume. 32 In this study, SF-36 had to be used since there was not a Turkish LE-specific questionnaire when PBI-L's Turkish validity and reliability had been carried out. In contrast, the Turkish version of the Lymphedema Quality of Life Questionnaire and Lymphedema Functioning, and Disability and Health Questionnaire were published recently.33,34
Blome et al. 14 could not find correlation between the general HRQoL questionnaire and PBI-L. However, they were able to do a more specific assessment by using Freiburg Life Quality Assessment in Lymphedema, which is a disease-specific HRQoL questionnaire. English version of PBI-L was also conducted by Blome et al. 14 According to the results of English version, there was no correlation between the general HRQoL questionnaire and PBI-L, but there was low negative correlation between disease-specific HRQoL questionnaire and PBI-L. Differently from English and German versions, a low negative correlation was found between some subdimensions of SF-36 and PBI-L. This difference may have occurred due to different questionnaires. Nevertheless, in our opinion, the benefit gained from the treatment was not able to be reflected fully by the general HRQoL questionnaires.
The strongest aspect of this study was that PBI-L is a tool that could be used in all LE, lipedema, and lipolymphedema patients without differentiating the affected side, and etiology. Furthermore, providing information about the benefit from the treatment to the patient directly and excluding the external factors that could affect the treatment are strong aspects as well.
The most significant limitation of this study was that it had to use a general HRQoL questionnaire since there was no disease-specific HRQoL questionnaire for LE when this study was carried out. The general HRQoL questionnaire may not have reflected the condition of the patients exactly. Another limitation was sociocultural diversity in our patients' profiles. This situation may have affected the perspective of patients concerning the treatment. The number of patients with lipolymphedema and lipedema was fewer than the number of patients with LE. Although this seems to be a limitation, it may not be a problem for the questionnaire to be administered because lymphatic system damage is present in the etiology of all these diseases. Also the needs and treatments are similar for all.
The Turkish version of PBI-L, which assesses the needs and treatment benefits from the patient's perspective, has been added to the literature for the use of health professionals responsible for LE treatments. PBI-L's validity and reliability were carried out and determined to be a valid and reliable tool. It was proposed that its validity may be assessed by disease-specific HRQoL questionnaires for LE.
Footnotes
Acknowledgments
We thank Blome et al. for permission to translate and validate this tool and Keith Carver for proof reading.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Author Disclosure Statement
No competing financial interests exist.