
Abstract
Abstract
Background:
Conservative nonsurgical treatment has traditionally been applied to lymphedema. Early surgical procedures were invasive and disfiguring and their long-term success was often limited. In contrast, contemporary surgical techniques are much less invasive and have been shown to be effective in reducing excess limb volume, the risk of cellulitis, and the need for compression garments. Microsurgical procedures such as lymphovenous anastomosis and vascularized lymph node transfer can treat the excess fluid component of lymphedema and are gaining in popularity. In this study, we first evaluate the possibility of generating lymphedema in the hind limb of a rabbit and then describe its treatment with microsurgical lymph node transfer without lymph vessel transfer.
Methods and Results:
In experimental rabbit models, animals first underwent surgery in which the popliteal lymph node was removed to create lymphedema in the hind limb. After 15 days, another operation was performed to excise the contralateral popliteal lymph node and transfer it to the limb with lymphedema. Our model showed that lymph node transfer was able to reduce lymphedema in the rabbit's hind limb; intervened hind limb: basal volume (51.94 ± 11.23), volume day transfer (73.40 ± 26.47), and final volume (50.13 ± 12).
Conclusion:
We have developed a feasible model to microsurgically induce and treat lymphedema by lymph node transfer that shows promising results.
Introduction
Lymphedema is a chronic disease characterized by massive lymphatic fluid stasis, inflammation, and fibroadipose deposition. It commonly affects people after lymphatic injury during the course of cancer treatment. In these individuals, progressive adipose deposition and tissue fibrosis result in increasing limb volume, heaviness, functional difficulties, increased susceptibility to infections, and rare but deadly secondary tumors. 1 Several clinical findings suggest that the pathology of lymphedema is a multistep sequence in which lymphatic injury is the initiator of these events. This hypothesis is supported by the fact that lymphedema develops only in a subset of patients who undergo lymphadenectomy rather than uniformly in all patients who suffer lymphatic injury. 2 In addition, some patients develop lymphedema even after apparent trivial injury to the lymphatic system, suggesting that even minor disturbances in lymphatic function can initiate the pathological sequence. 3 Finally, in most patients, lymphedema develops slowly, usually months to years after the initial surgical injury, suggesting that intervening secondary events are necessary for development of this pathological process. 4
The treatment of lymphedema has traditionally been conservative and nonsurgical. However, surgical options for the condition have been reported for over a century; early surgical procedures were invasive and disfiguring and their long-term success was often limited. In contrast, contemporary surgical techniques are much less invasive and have been shown to be effective in reducing excess limb volume, the risk of cellulitis, the need for compression garment use, and subsequent treatment. Microsurgical procedures such as lymphovenous anastomosis, vascularized lymph node transfer, and lymphatic–lymphatic bypass can treat the excess fluid component of lymphedema swelling that presents as pitting edema. Today, these surgical techniques are becoming increasingly popular.
The most recent advance in surgical lymphedema treatment is vascularized lymph node transfer. Healthy lymph nodes, an artery, and a vein are transplanted from the axilla, groin, or submental region to the affected area.5–9 One hypothesis is that the transferred lymph nodes act as a pump and suction pathway for lymphatic clearance. 7
Research into prevention and treatment of lymphedema requires animal models to determine the pathophysiology of the disease process and to identify the ideal timing and specific interventions for these patients. 10 Obviously, generating chronic and consistent lymphedema in experimental animals is highly problematic. Historically, efforts to replicate human untreated lymphedema in animals through surgery, radiation, and toxicology have been fraught with difficulties. The main obstacles to creation of satisfactory animal models include an inability to reproduce chronic disease in a format that is reproducible and stable over time. 10 Murine models have been created to evaluate the results of lymph node transfer, including clinical outcome and histology and immunohistochemistry.11–13 In a sheep model, vascularized lymph node transplants were found to achieve greater lymphatic transfer than avascular lymph node transplants. 14 For this reason, we have created an experimental rabbit model, 15 which is able to induce lymphedema similar to that in humans and lasts long enough to allow treatment with a variety of techniques.
The rabbit's body size permits the transfer of peripheral vascularized lymph nodes. In smaller mammals, this can only be performed with the mesenteric lymph node, which makes both the surgical approach and animal recovery difficult. The lymphatic anatomies of the hind limb and the blood supply of the rabbit popliteal node are well documented, and furthermore, the popliteal node is easily identified and can be explored with a minor procedure. 16
According to Suami et al., the lymphatic system of a rabbit has three or four lymphatic vessels in the paw with no clear separation between superficial and deep lymphatic vessels. This contrasts with lymphatic vessels in paws of dogs and in human feet, which are separated by deep fascia.17,18 However, it has been established that lymph from the lower limb is drained by two lymphatic systems: first, the superficial system comprising two sets of vessels, one of which drains the medial skin toward the inguinal nodes in the groin and the other drains the lateral skin to the popliteal node; and second, the deep lymphatic system, which drains the deep tissues of the foot and lower limb to the popliteal node. 19
In this study, we first evaluated the possibility of generating lymphedema in the hind limb of a rabbit, and then treated it with a microsurgical lymph node transfer without lymph vessel transfer. The rabbits first underwent surgery, in which the popliteal lymph node was removed to create lymphedema in the hind limb. After 15 days, another intervention was performed to excise the contralateral popliteal lymph node and transfer it to the limb with the developed lymphedema.
Materials and Methods
In the present study, eight male New Zealand White rabbits weighing 2.5–3 kg were used. The animals were housed at the Animal Experimentation Unit of the Research Institute at Santa Creu i Sant Pau Hospital (Barcelona).
All procedures performed were evaluated and approved by the Internal Animal Care and Use Committee and authorized by the external board of experts of the local government (Comissió d'Experimentació Animal—Generalitat de Catalunya), with the registration number: 6645.
For induction of lymphedema, the animals were anesthetized with ketamine (1 mg/kg) and medetomidine (0.5 mg/kg). All animals received a dose of prophylactic antibiotic (ceftiofur 0.1 mg/kg). Analgesia was controlled with a prior dose of meloxicam (1 mg/kg, i.m.) and local bupivacaine (0.75% s.c.) at the site of the incision. At the end of surgery, a single dose of buprenorphine (0.01 mg/kg) was administered to prevent postoperative pain. Animals were controlled daily to detect suffering or pain using a specific pain score.
To identify lymph channels and the popliteal lymph node, 0.3 cubic centimeters (cc) of patent blue V was infiltrated intradermally in the second and third interdigital spaces.
The back of the left hind limb was shaved and a 2-cm incision longitudinal to the long axis of the hind limb was made over the popliteal fossa. The fat layer under skin was removed to visualize lymph vessels (stained in blue), over the muscular fascia, and to find a single lymph node ∼0.8 mm in diameter in the fossa.
Distal to this lymph node are two principal lymph vessels running parallel to a central vein. These vessels reach the lymph node by the medial side, wrapping the node in a net of microvessels (Fig. 1).

Macroscopic view of popliteal lymph node and afferent lymphatica channel. Color images are available online.
To remove the lymph node, the medial artery (branch of the popliteal artery) and the lateral vein irrigating the node were ligated and proximal lymphatic vessels were cauterized. The internal tissue was sutured with 4/0 Vicryl® with continuous stitches and the skin was sutured with 3/0 silk with single invaginant stitches. The discarded lymph node was preserved as a control for further histological studies.
Following this procedure, each animal was its own control (right hind limb) for induction of lymphedema in the left hind limb (treated). After the lymph node transfer surgery and to compare volume reduction of the left hind limb (treated), the measures were compared with former values obtained in the control (right) hind limb, before removing the lymph node, during the first part of the study.
The day after the surgery, perimeters of the hind limbs of the rabbit were measured with a measuring tape from the ankle to the knee and every 2 cm to calculate the total volume of the leg using the truncated cone formula. All the measures were made by the same researcher in all animals. The volume evolution of the operated (left) and healthy (right) hind limbs was measured on days 0, 3, 7, 10, and 15 after removing the lymph node. Initial and final measurements were performed under anesthesia.
Fifty days after the surgery, the animals were anesthetized again and 0.3 mL of patent blue V was injected intradermally in the distal paw of each limb. The right lymph node was excised, as explained above, but the lateral vein and medial artery were preserved. An incision in the left hind limb was made in the popliteal fossa; the fibrotic tissue was removed, preserving the muscular fascia where the right lymph node was transferred. The node was transferred to the left hind limb with an anastomosis of the vein and artery.
The day after this surgery, the perimeter of both hind limbs was measured as explained above to evaluate reduction in volume of the lymphedema in the left leg and induction of lymphedema in the right leg.
Animals were humanely euthanized on day 30 of the study. The transferred lymph nodes were quickly harvested within the surrounding fat and, with their artery, vein, and lymph vessels, fixed and prepared for histology and immunochemistry evaluations.
The architecture of the transferred nodes was evaluated with hematoxylin–eosin and compared with the anatomy of the lymph nodes discarded after the first surgery.
Statistical analysis
The number of animals to be used in the procedure was calculated using the formula based on serial incidents. 20
The evolution of the lymphedema volume was performed by calculating the volume of the hind limbs. As this involved the addition of various truncated cones, the lower and upper radii were obtained by measuring each lower (closer to the ankle) and upper (closer to the knee) perimeter of the leg, and the height was the distance between measurements (2 cm).
To analyze differences in volume in both procedures (induction and treatment of lymphedema) in the same animal, the volumes obtained in the right and left hind limbs were reduced to three levels of repeated measures by group (induction and treatment): baseline (before lymphedema induction in the right and left hind limbs), lymph node transfer surgery, and end of the study. Values were analyzed by two-way analysis of variance (volume evolution and group treatment). Volume (in cc) is expressed as mean + SD. p-Values <0.05 were considered statistically significant.
The software used to process the data was IBM-SPSS (v25.0).
Results
Hind limb volume
The serial measurements obtained during the study showed a statistical increase (p < 0.05) of volume in the hind limb treated from baseline (51.94 ± 3.01 cc) to lymph node transfer day (73.4 ± 6.48 cc) and a statistical reduction (p < 0.05) of volume until the end of the study (50.14 ± 3.28 cc). This volume increase of the treated hind limb on lymph node transfer day was also statistically significant (p < 0.05) compared with the control hind limb (Fig. 2 and Table 1).
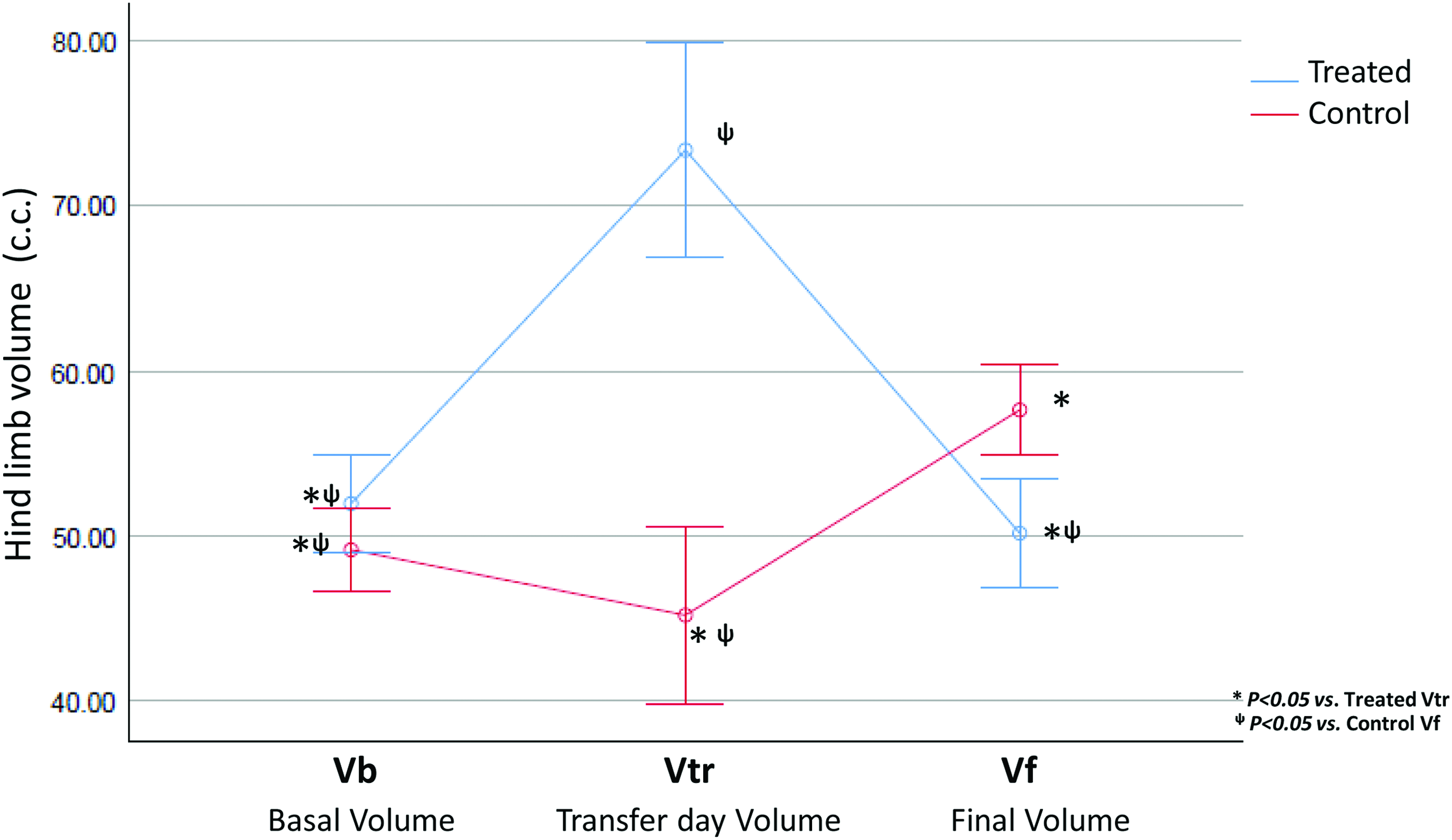
Hind volume evolution, after performing the volume calculations for a truncated cone, values were obtained in cc with their SD. Intervened hind limb: Vb (51.94 ± 11.23), VTr (73.40 ± 26.47), and Vf (50.13 ± 12) in relation to the control Vb (49.12 ± 4.67), volume day intervention (45 ± 4.74), and Vf (57, 63 ± 5.35). p < 0.05. cc, cubic centimeters; SD, standard deviation; Vb, basal volume; Vf, final volume; VTr, volume day transfer. Color images are available online.
Hind Limb Volume Evolution
p < 0.05 vs. VTr of treated hind limb.
p < 0.05 vs. Vf of control hind limb.
SE, standard error; Vb, basal volume; Vf, final volume; VTr, volume day transfer.
Histology
The transferred lymph nodes kept their architecture similar to the normal excised nodes, and the cortex and medulla of the transferred node kept the same relationship. More concentration of lymphatic and vascular vessels was observed in the cortex area, suggesting revascularization (Fig. 3).

Histological rabbit popliteal lymph node.
Discussion
Our experimental model showed that lymph node transfer can reduce lymphedema in the hind limb of a rabbit.
The transferred nodes are totally functional in the recipient leg because the amount of lymphatic fluid is reduced, their efferent and afferent lymphatic vessels generate new functional connections with the transferred node, and the lymph node maintains natural architecture after transfer.
Our results may provide answers to the three questions posed by Shesol et al. 21 : (1) the lymph node transferred constituted a continuity of the operated lymphatic vessels; (2) time is a consuming factor for success; and (3) there are vascular requirements for transplantation.
Using this rabbit model, we can confirm that the transferred node establishes new and spontaneous connections with lymph vessels that were present in the niche. We anastomosed only the artery and vein of the node, and the image of patent blue at the end of the study showed a continuity of lymph vessels from the paw to the inguinal region through the transferred popliteal node.
In our previous study, 15 we showed that in 3 weeks after induction of lymphedema, the edema was progressively reduced, but that the increase in volume was maintained because of the chronic status of the condition. This is why in this study, the surgery to transfer the lymph node was performed 15 days after lymphedema induction; we thus avoided a fibrotic status that complicates the surgery and well-being of the animals.
At least the main node artery and vein must be transferred with the lymphatic node to maintain its function and allow it to create lymphatic connections.
The study must be carried out over an extended period of time to corroborate that the lymph node maintains its function, to determine the evolution of the lymphedema, and to establish the best moment to perform the node transfer. However, even with leakages, this first approach to the surgery obtained promising results and allowed microsurgical training with a realistic lymphedema model. However, it should be borne in mind that lymphedema evolves faster in rabbits than in humans due to the fact that they are animals, their youthfulness, and their capacity for regeneration.22–24
The development of animal models for the study of the lymphatic system has led to an explosion of information on mechanisms governing lymphatic development and diseases associated with lymphatic dysfunction. 25 Using this rabbit model, the underlying mechanism of lymphedema can be studied in a practical and realistic setting.
Conclusion
In animal studies of lymphedema, there is a natural resolution of the edema over time, but not of total volume. Therefore, caution is in order when extrapolating findings from animal models to the clinical setting.
The procedure described here is less extreme than other methods published with interventions such as circumferential denuding of the soft tissue, compression banding, and radiation. The goal is to induce secondary lymphedema while causing minimal degree of morbidity to the animal.
The study sample is small but adequate given the resources available and the need to limit the animal lives used.
Future power calculations may be based on measurements used in this study to calculate study size.
Footnotes
Acknowledgments
This study was funded by Fondo de Investigación (FIS) en salud del Ministerio de Sanidad y Consumo de España, Instituto Carlos III. Fondo Europeo de Desarrollo Regional (FEDER). Project No. PI1302793. The authors thank Ignasi Gich, PhD, for statistical and methodological assistance and Dr. J. Oriol Juan-Babot for performing histopathological sections.
Author Disclosure Statement
No competing financial interests exist.