
Abstract
Abstract
Introduction:
Vascularized lymph node transfer (VLNT) has become the established treatment for secondary lymphedema. The proposed mechanisms of VLNT include lymphangiogenesis and absorptive action of transplanted lymphatic tissue. Therefore, in theory, the lymph node content of lymph node flap is crucial to clinical response. The supraclavicular lymph node flap (SCLNF) has been described as one of the flap options for VLNT. However, its lymph node content has not been fully studied. The aim of this study is to find out the lymph node content of SCLNF with histological examination.
Methods:
Patients who required radical neck dissection or modified radical neck dissection due to cervical lymph node metastasis from head and neck cancer were included in this study. The SCLNF harvesting was performed as the first part of neck dissection. After flap harvesting, neck dissection was continued. The fresh SCLNF specimens were then sent for histological study.
Results:
Twelve SCLNFs were studied. The mean age of patients was 67.5 (range, 54–84) years. There were 10 males and 2 females. Seven flaps were harvested from the left side of neck, while five flaps were harvested from the right side of neck. The mean width, height, and thickness of SCLNF were 5.9 ± 0.6, 4.0 ± 0.5, and 1.8 ± 0.2 cm, respectively. The mean number of lymph nodes per flap was 8 ± 4.7 (range, 3–15).
Conclusion:
The lymph node content of SCLNF was confirmed. Its lymph node content is comparable to other lymph node flaps used in VLNT.
Introduction
Vascularized lymph node transfer (VLNT) has become an established treatment of secondary lymphedema. Various donor sites have been described, which include neck, axilla, groin, and intraabdominal donor sites.1–8
The use of supraclavicular lymph node flap (SCLNF) for the treatment of secondary lymphedema has been described in clinical studies.6,9,10 However, its lymph node content has not been fully investigated.
The aim of this study is to confirm the lymph node content of SCLNF. Histological examination was performed on fresh skinless SCLNF specimens. The number of lymph nodes inside the flap was counted under microscope. The flap harvesting technique is also described in this article.
Materials and Methods
Study design
This was a collaborative study among the Division of Plastic and Reconstructive Surgery and Department of Ear, Nose, and Throat (ENT) in our institute.
Patients who required radical neck dissection or modified radical neck dissection due to cervical lymph node metastasis from head and neck cancer were included. The presence of cervical lymph node metastasis was confirmed with fine needle aspiration cytology. Ultrasonography and computed tomography or magnetic resonance imaging were ordered routinely to define the location of metastatic lymph nodes. Patients with metastasis to level V lymph node were excluded to avoid interfering with the histological study.
The SCLNF harvesting was performed as the first part of neck dissection by the first author (H.-L.L.), who is a plastic surgeon. After flap harvesting, neck dissection was continued by the second author (J.C.-K.C.), who is an ENT surgeon. The fresh SCLNF specimens were then sent for histological study.
Institutional review board approval was obtained for this study. Written consents were obtained for both operation and study. All operative procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Patients
Between June 2017 and April 2018, 12 patients with head and neck cancer, who required neck dissection, were included in this study. The mean age was 67.5 (range, 54–84) years. There were 10 males and 2 females.
Four patients had laryngeal cancer, three patients had oral cancer, and two patients had oropharyngeal cancer. Other cancer types include cancer of the lower alveolus and salivary gland cancer. No patient received radiotherapy before neck dissection.
Neck dissection technique
McFee skin incision was used for neck dissection. A subplatysmal plane was then elevated. Level I–V lymph nodes, the tail of parotid gland, and submandibular gland were removed. Depending on the type of modified radical neck dissection, structures like sternocleidomastoid muscle (SCM), internal jugular vein, and spinal accessory nerve might be sacrificed.
For the purpose of study, the SCLNF harvesting was performed as the first part of neck dissection. SCLNF was dissected out separately instead of being delivered en bloc with the neck dissection specimen. After flap harvesting, neck dissection was carried on in the usual manner.
Flap harvesting
The flap was based on transverse cervical artery (TCA). The posterior triangle of neck was first defined by marking the posterior border of SCM, the anterior border of trapezius muscle, and clavicle. The target lymphatic tissue was located at the base of the posterior triangle (Fig. 1).
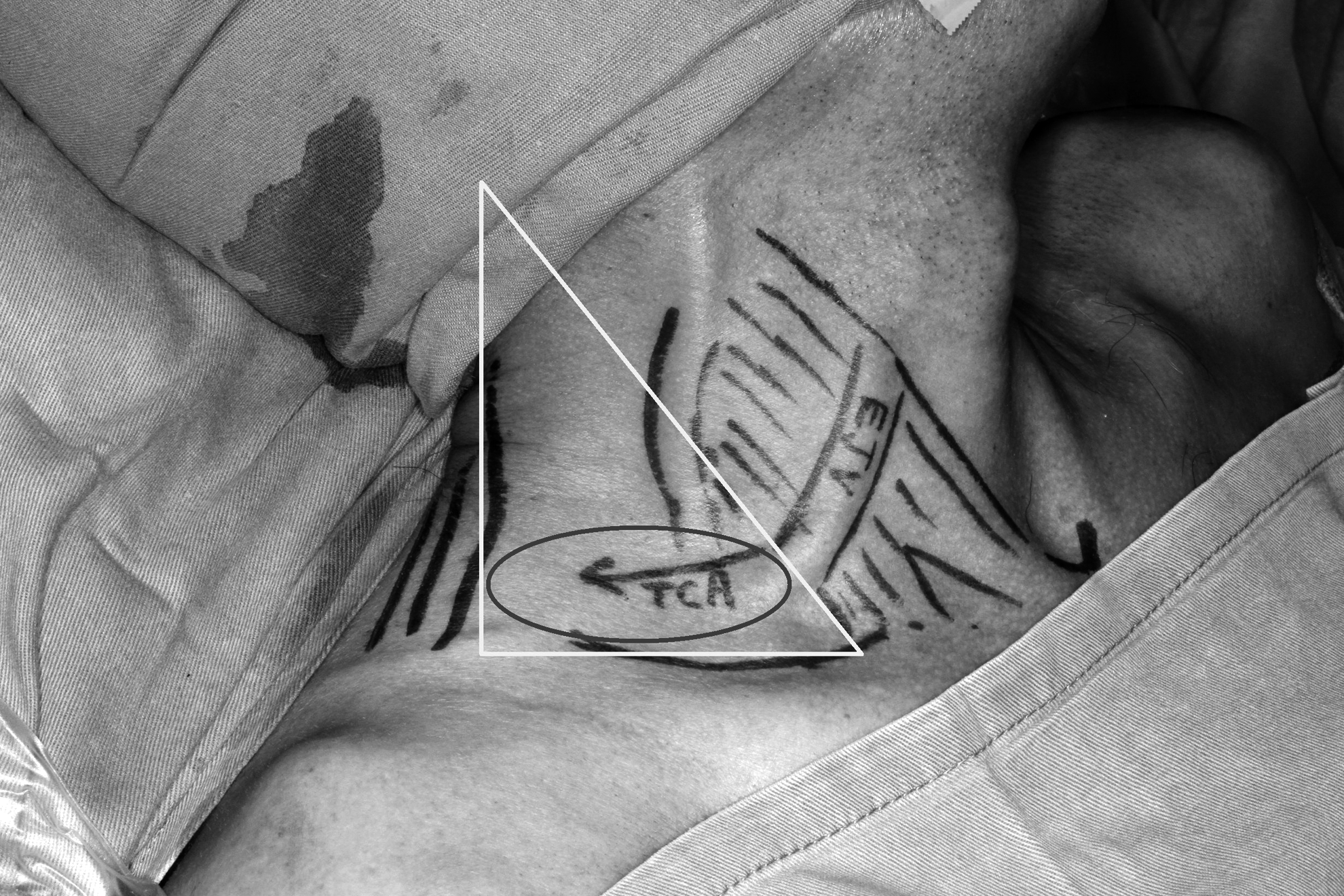
The posterior triangle of neck was outlined (triangle), which was bounded by SCM, trapezius, and clavicle. The EJV was outlined and harvested as the pedicle vein. The targeted tissue was at the base of the posterior triangle (ellipse). EJV, external jugular vein; SCM, sternocleidomastoid muscle.
Skin crease incision was made 1 cm above the clavicle to avoid conspicuous scar. The skin flap was raised at the subplatysmal plane. Clavicle, SCM, and external jugular vein (EJV) were exposed immediately after raising the skin flap cranially (Fig. 2). The branches of supraclavicular nerve overlying the clavicle were severed.

Level Vb region of the right side of neck. After making the supraclavicular skin crease incision, the skin flap was raised at the subplatysmal plane. EJV and SCM (asterisk) were exposed immediately beneath the skin flap. The anterior border of the trapezius muscle was covered with fibrofatty tissue.
It was our practice to first incise at the posterior border of the SCM to expose the proximal part of TCA, so that the surgeon could have the idea of where to place the central axis of the flap.
After that, the flap dissection was begun at the inferior border and subsequently the lateral border. During the dissection of inferior border of the flap, that is, clavicular region, the posterior belly of omohyoid muscle and some branches of EJV were exposed (Fig. 3). The posterior belly of omohyoid muscle was transected to facilitate further dissection. The EJV branches were clipped and preserved as the pedicle vein. At the lateral border dissection, the anterior border of trapezius muscle was first exposed by incising the fibrofatty tissue laterally. The distal runoff of TCA was then exposed and ligated.

The anterior border of trapezius muscle (asterisk) was exposed after incising the fibrofatty tissue laterally. The posterior belly of omohyoid muscle was isolated and subsequently transected during dissection of the inferior border of the flap (i.e., clavicle).
The SCLNF was then elevated from inferior to superior (clavicle to head end) and lateral to medial (trapezius to SCM). The deep plane of SCLNF elevation was along the undersurface of TCA. The identification of this plane was facilitated by tracing the ligated distal runoff of TCA (Fig. 4). When the flap was elevated from this plane, brachial plexus, and phrenic nerve were exposed and preserved at the lateral and medial part of the surgical field, respectively. The superior extent of the flap was a bit arbitrary, which was taken around 2 cm superior to the horizontal course of TCA. The harvesting procedure was completed after isolating the TCA. To obtain a longer pedicle length, SCM could be retracted to expose the TCA origin at the thyrocervical trunk (Fig. 5). Besides the flap's lymph node content, the size and length of TCA were also studied. The diameter of TCA was measured at the point where it was considered suitable for microvascular anastomosis.

The right side of neck. The picture was taken from the head end. The distal runoff of TCA was ligated. The identification of the deep plane of flap dissection could be facilitated by following the undersurface of the TCA (arrows). TCA, transverse cervical artery.

The SCLNF was about to be detached. If a longer pedicle length (two arrows) was desired, the thyrocervical trunk could be exposed by retracting SCM medially. The phrenic nerve (single arrow) was lying on the anterior scalene muscle. The brachial plexus (asterisk) was emerging at the lateral border of the anterior scalene muscle. Both phrenic nerve and branchial plexus lied beneath the plane of TCA. SCLNF, supraclavicular lymph node flap.
After the flap was delivered, Valsalva maneuver was performed to rule out lymph leak. The leaking lymphatic channels were plicated with silk sutures.
Processing and examination of SCLNF specimens
The SCLNF specimens were fixed in 10% formaldehyde immediately after harvesting. After fixation, the specimens were embedded in paraffin and sectioned at 2 mm interval. The sections were subsequently stained with hematoxylin and eosin (H&E).
The histological studies were performed by board-certified pathologists. To be qualified as a lymph node, the structure needs to have (1) a capsule, (2) subcapsular sinus, and (3) lymphoid follicles (Fig. 6). The presence of head and neck cancer metastasis was identified by H&E staining.
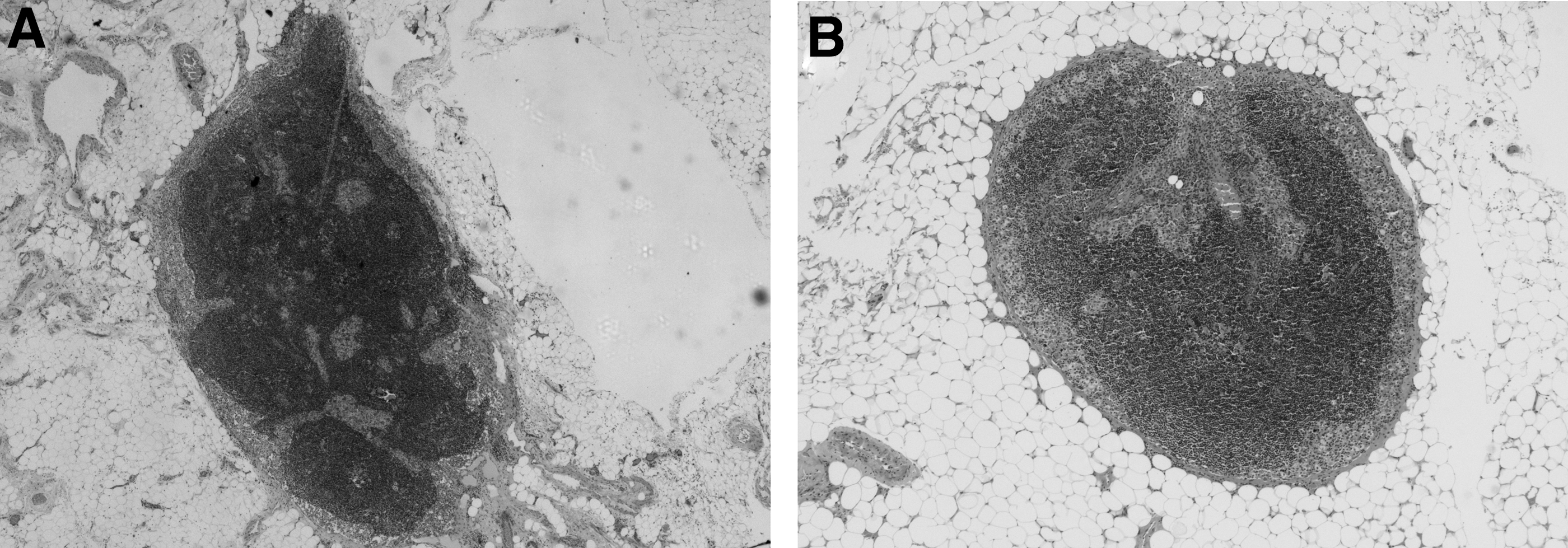
The histological section [hematoxylin and eosin stain,
Statistical analysis
All values are reported as mean ± standard deviation. Independent sample t-test was used to compare the difference in lymph node content between the left and the right sides of neck. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed with IBM SPSS Version 22.0 (IBM Corp., Armonk, NY).
Results
A total of 12 SCLNFs were studied. Seven flaps were harvested from the left side of neck, while five flaps were harvested from the right side. For the dimensions of flap, the mean transverse dimension/width (length from the trapezius end and the SCM end) was 5.9 ± 0.6 cm (range, 5–7 cm), the mean craniocaudal dimension/height was 4.0 ± 0.5 cm (range, 3–5 cm), and the mean thickness of flap was 1.8 ± 0.2 cm (range, 1.5–2 cm). The dimension measurement was made in the operation theater immediately after the SCLNF was delivered (Fig. 7). The mean diameter of TCA was 1.8 ± 0.5 mm (range, 1–2.5 mm) and the mean length of TCA was 2.1 ± 0.3 cm (range, 1.8–2.7 cm).

This was the harvested SCLNF. The transverse dimension (width) of the flap was relatively standard as it was the distance between the posterior border of SCM and the anterior border of trapezius muscle, which was round 5.5–7 cm.
For the histological study, there was no tumor metastasis in all 12 SCLNF specimens. The mean number of lymph nodes per flap was 8 ± 4.7 (range, 3–15). For the seven flaps harvested from the left side of neck, the mean number of lymph nodes per flap was 8.4 ± 5.7 (range, 3–15). For the five flaps harvested from the right side, the mean number of lymph nodes per flap was 7.4 ± 3.4 (range, 5–13). The difference in the flap lymph node content between the left and the right sides of neck was not significant (p = 0.72). The patient demographics and flap characteristics are listed in Table 1.
Patient Demographics and Supraclavicular Lymph Node Flap Characteristics
Discussion
The proposed mechanisms of VLNT include lymphangiogenesis and absorptive function of the transplanted lymphatic tissue. In theory, the lymph node content of lymph node flap is crucial to the success of treatment.11–17
According to the neck lymph node classification system published by the American Academy of Otolaryngology–Head and Neck Surgery in 2008, neck lymph nodes are divided into seven levels. The level V region also refers to the posterior triangle of the neck, which is bounded by the posterior border of SCM, the anterior border of trapezius muscle, and the clavicle. Level V is further subdivided by the horizontal plane of the inferior border of cricoid cartilage. Level Va nodes refer to the nodes superior to this plane, while, level Vb nodes are also known as transverse cervical nodes, which are located inferior to this plane. 18
The targeted nodes of SCLNF harvesting are located in level Vb. However, they not equivalent to level Vb nodes as the SCLNF dissection is dependent on the course of TCA rather than a level Vb anatomical dissection.
Different donor sites have been described for vascularized lymph node flap, which include neck, groin, axilla, and mesentery.1–7 For the treatment of secondary lymphedema of lower limb, the sensible options remaining are neck, axilla, and intraabdominal donor sites.
Neck donor sites include the submental and supraclavicular regions. The harvesting of submental lymph node flap results in visible scar and depression at the upper neck. Meticulous dissection under loupe or even microscopic magnification is usually required for the preservation of the marginal branch of facial nerve.
Mesenteric or gastroepiploic lymph node flap requires the opening of abdominal compartment. For plastic surgeons who are not familiar with abdominal procedure, the flap harvesting may have to be performed by general surgeons.
In our institute, SCLNF is the preferred flap for the treatment of secondary lower limb lymphedema. The advantages of a supraclavicular region donor site include inconspicuous scar (Fig. 8), acceptable donor site morbidity, and negligible chance of iatrogenic lymphedema.

This patient had undergone vascularized SCLNF transfer for the treatment of secondary lower limb lymphedema. The SCLNF was harvested from her right side of neck. The depression at the donor site was minimal and the scar was inconspicuous.
The flap harvesting involves the sacrifice of the branches of supraclavicular nerve, omohyoid muscle, and EJV. From our experiences, numbness over the lower neck and supraclavicular region due to the loss of the branches of supraclavicular nerve is well tolerated by most patients. Also, the sensation usually returns partially around a year after operation. The loss of omohyoid muscle does not usually lead to any functional loss.
From earlier study, the head and neck region has a rich collateral lymphatic network. Therefore, we believe that the chance of iatrogenic lymphedema of the head region after SCLNF harvesting is low. 19
There was one cadaveric study conducted by Gerety et al. describing the lymph node content of SCLNF. A total number of 10 SCLNFs were studied. The flap size was expressed in terms of weight. The mean weight of SCLNF was 12.9 g. Also, the mean number of lymph nodes per flap was 2.5 ± 1.7. 20
There are fundamental differences in the study design between Gerety's study and our study. First of all, this is the only study in the literature describing the histological findings of fresh SCLNF specimens. We believe that a more accurate histological examination can be carried out with fresh samples as opposed to cadaveric samples.
Second, the flap described in Gerety's study was a, SCLNF with a skin island, while the flap described in our study was a skinless flap. Third, the flap size in our study was expressed in terms of width, height, and thickness, while it was expressed in terms of weight in Gerety's study. Obviously, the weight of a cadaveric specimen is not equivalent to the same weight of a freshly harvested specimen from a living human. Also, we believe that most surgeons will agree that width, height, and thickness are more easily comprehensible than the weight of a flap.
Regarding the findings, the lymph node content of SCLNF in our study was higher than that from Gerety's study (8 ± 4.7 vs. 2.5 ± 1.7). One possible explanation was that in Gerety's study, the mean weight of flap with a skin paddle was 12.9 g. Although the net weight of the fibrolymphatic component was not described by Gerety et al., we believe that the average flap size in our study is bigger compared with the fibrolymphatic component of flap in Gerety's study.
Steinbacher et al. studied the lymph node content of SCLNF with ultrasonography. 21 A total of 18 supraclavicular fossae were scanned. The mean numbers of lymph nodes per flap were 1.5 on the right side and 3 on the left side. We believe that the lymph node counting with histological study is more sensitive and accurate than using ultrasonography.
The lymph node contents of other lymph node flaps were described by various researchers. Cheng et al. and Dayan et al. described the lymph node content of groin lymph node flap.22,23 The mean numbers of lymph nodes per flap were reported to be 6.2 by Cheng et al. and 8.2 by Dayan et al. Cheng et al. also described the content of submental flap; the mean number of lymph node per flap was 2.3. 2 Barreiro et al. studied the content of lateral thoracic flap; the number of lymph node per flap ranged from 3 to 7. 24
When the SCLNF is harvested according to our described technique, its lymph node content is comparable to that of groin lymph node flap and even superior to that of submental flap. In theory, the clinical responses after VLNT should correlate with the number of lymph nodes transplanted to the edematous limb. However, there is no evidence to support this hypothesis. Kenworthy et al. reported transferring two omentum flaps to a single edematous limb. However, the focus of this study was on the lymphoscintigraphy and indocyanine green lymphangiography findings. Clinical result was not presented. 25
Conclusion
SCLNF is a sensible flap option for the treatment of secondary lower limb lymphedema. Its advantages include relatively straightforward flap raising procedure and acceptable donor site morbidity.
The study confirms its lymph node content, which is comparable to other lymph node flaps.
Footnotes
Author Disclosure Statement
No competing financial interests exist.