
Abstract
Background:
Patients treated for breast cancer with breast conserving surgery and radiotherapy (RT) often complain about swelling, heaviness, and pain in the treated breast. This pilot study was undertaken to examine if compression therapy was effective as an early treatment to reduce breast edema and symptoms assessed by Visual Analogue Scale (VAS).
Methods and Results:
Fifty-six breast cancer-treated women with breast edema, diagnosed by the measurement of tissue water content by tissue dielectric constant (TDC) technique 3 months post-RT, were randomized to either an intervention group, wearing a sports bra of compression type, or a control group, wearing a standard bra daily for 9 months when tissue water content in breast, upper arm, and lateral thorax of the operated side, and symptoms assessed by VAS were evaluated. No differences were found between the groups at start or end of study concerning tissue water content or VAS. However, within both groups, a significant reduction in tissue water content and experience of heaviness was found.
Conclusion:
Breast edema as well as experience of heaviness in the affected breast found at 3 months post-RT decreased after 9 months independent of whether a sports bra of compression type or a standard bra was used.
Introduction
Patients treated for breast cancer with partial mastectomy and radiotherapy (RT) to the breast complain about swelling, heaviness, redness, and pain in the treated breast.1,2 The incidence of swelling shows a great variation between 0% and 90%, probably because of a large variation of measurement methods as well as of time after RT. 2 Constantine et al. found that 17% of patients experienced breast edema within 90 days of RT, scored on a 10-point scale. 3 One year post-surgery and -RT to the breast, Rönkä et al. found subcutaneous edema of the breast, measured with ultrasound, in 70% of patients with axillary node dissection and in 28% with sentinel node biopsy. 4 After a median follow-up of 27 months, Goffman et al. found an incidence of breast edema only in about 10% of patients in a similar material, using clinical signs such as erythema and changes similar to peau d'orange of the breast as indicators of edema. 1
In a recent study, the incidence of breast edema was 63% at 3 months after breast conserving surgery and RT. 5 The measurements were performed with a tissue dielectric constant (TDC) technique based on high-frequency electromagnetic waves measuring tissue water content. The technique has been introduced showing potential to measure breast edema. 5 Since the technique enables the measurement of different quadrants of the breast, it may provide information that may lead to improvement in conservative treatment of breast edema.
Prior studies have suggested that breast cancer-related arm lymphedema can be diagnosed early with MoisterMeterD.6,7 The device, assessing the TDC, has also been compared with bioimpedance spectroscopy assessing extracellular fluid in this group of patients. Both methods can identify early lymphedema, but the TDC technique shows a higher sensitivity. 8
Treatment of arm lymphedema, following breast cancer treatment, by compression garment is well documented. 9 It is our clinical experience that breast edema commonly is treated with a compression bra, often a sports bra of compression type, which can be expected to have an effect on breast edema. For arm lymphedema it has also been shown that early treatment can keep the lymphedema volume at a very low level in 80% of patients during many years. 10 Therefore, we hypothesized that breast edema can be treated by compression at an early stage. We also wanted to investigate if an association between breast edema and edema in the upper arm or lateral thorax could be found.
Materials and Methods
Design
This was a randomized controlled pilot study evaluating the effect of 9-month intervention with compression treatment for breast edema following breast conserving surgery and RT to the breast.
Patients
Within a longitudinal study of breast edema, 118 patients treated for breast cancer with breast conserving surgery and sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND), and RT to the breast, at the Department of Oncology at Skåne University Hospital, Sweden, were examined for breast edema. 5 Patients with preoperative chemotherapy, recurrent cancer, or concurrent diseases that may interfere with measurement of edema and patients with difficulties in participating in the study, for example, dementia, were excluded.
Ninety-six patients were examined 3 months post-RT within the longitudinal study, and 70 patients diagnosed with breast edema (inter-breast TDC ratio ≥1.40) were included in the present intervention study. Twelve declined to take part mostly due to long travel distance. Fifty-eight patients were randomized to either control (CG) or intervention group (IG). Two patients dropped out without giving any reason, one in each group (Fig. 1). Finally, 56 patients, 28 in each group, completed the study. There were no statistically significant differences in patient characteristics between the groups (Table 1).

Flowchart of patients treated for breast cancer with breast conserving surgery and RT to the breast. RT, radiotherapy.
Characteristics of Breast Edema Patients (N = 56) Taking Part in the Intervention Study
With multifocal tumors in 15 patients, the size of each tumor was added up to a total sum.
Surgeries considered to be performed in 0 quadrant were performed at the border of the quadrants.
Bra size was reported by the patient.
BMI, body mass index; CG, control group; IG, intervention group.
All subjects provided written documentation of informed consent before participation in the study. The study was approved by the Research Ethics Committee, Lund University, Sweden, Dnr 2011/7, and performed in accordance with the Declaration of Helsinki.
Procedure
After evaluation at 3 months within the longitudinal study by one of the two physiotherapists (V.F. or L.J.) and inclusion in the present study, patients were randomized by K.J., in random blocks of four, to either IG or CG. Duration of the longitudinal study was 1 year after completion of RT, consisting of a randomization at 3 months post-RT and intervention time of 9 months. Thus, patients included at 3 months post-RT took part in the present study for 9 months.
The intervention group
Patients were provided with sports bras of compression type with firm pressure flattening the breasts. The bras were of different designs, fitted for each woman, making sure they were comfortable. The bras were worn during daytime, but not during nights, based on the common regime applied for arm lymphedema where a compression garment most usually is worn during daytime.
The control group
Patients used ordinary bras during daytime, but were allowed to use loose-fitted sports bras.
Patients in both groups were told to continue with daily activities such as work, household activities, and sports during the study as they had done before.
By end of intervention, pressure of the bra was measured by K.J., who was not blinded to group status. Evaluation started with measuring weight and length to calculate body mass index (BMI), followed by assessment of experiences of tightness, heaviness, and pain in the breast, and at last TDC measurements of breast, arm, and lateral thorax. Assessments were performed by V.F. and C.J., who were blinded to group status. Each physiotherapist performed both pre- and postintervention measurements for the same patients.
Measurements
Primary outcomes of interest of this study were TDC values, as indices of local tissue water of the breast, and patients' experiences of tightness, heaviness, and pain in the irradiated breast. Secondary end points were tissue water content in upper arm and lateral thorax of the affected side. Assessments were made before and immediately after intervention.
Local tissue water was measured by the TDC technique (MoistureMeterD; Delfin Technologies Ltd., Finland). The device transmits a very high-frequency electromagnetic (EM) wave of 300 MHz into an open-ended coaxial probe in contact with the skin. A part of the EM energy is absorbed by tissue water, while the rest is reflected back to the coaxial line, and an electrical parameter, TDC, directly proportional to tissue water content in skin and upper subcutis is calculated. 11 With the TDC technique, local tissue water in both breasts was measured to an effective depth of 2.5 mm. The effective depth illustrates the depth where the EM field in water-equivalent material has attenuated to 37% of the value at the skin surface. The TDC scale ranges from 1.0 to 78.5 based on the percentage of fluid at the measurement site, where a value of 1 indicates that the object has no water, and 78.5 indicates that the object has 100% of water. The measurement has been validated against circumference measurements of the forearm by hemodialysis treatment and showed a high correlation (r = −0.97, p < 0.05) in edema reduction and fluid removal during hemodialysis treatment (r = −0.99, p < 0.01).
Breast
Affected and contralateral breast TDC values were measured with the patient in supine position. The four quadrants of the breast were marked, and the numbering of the quadrants was based on the order used in the surgical procedure. Measurements were performed in the following order, starting with the operated breast; upper medial; lower medial; lower lateral; and upper lateral quadrant. Measurements were made along a line that bisected each quadrant with the edge of the probe 10 mm from the edge of the areola (Fig. 2), and measurement results were registered for both breasts. The mean TDC value of the total breast (four quadrants) was then calculated; however, quadrant(s) with scar tissue were excluded, and for the corresponding quadrant(s) in the healthy breast, a TDC ratio was determined using mean values from both breasts.

Each quadrant of the breast was measured with the probe placed along a line that bisected each quadrant with the edge of the probe 10 mm from the edge of the areola.
Arm
With the patient in supine position and with the arms in outward rotation, the tissue water content in medial upper arms of both upper limbs, 5 cm proximal to the anticubital fossa, was measured by TDC technique.
Lateral thorax
With the patient in prone position with arms along the side and the head resting in a neutral position with face down, the thoracic measurement site was defined at a spot 5 cm caudally from a line drawn between the highest point of the fold between arm and body and the lateral scapula edge (Fig. 3).
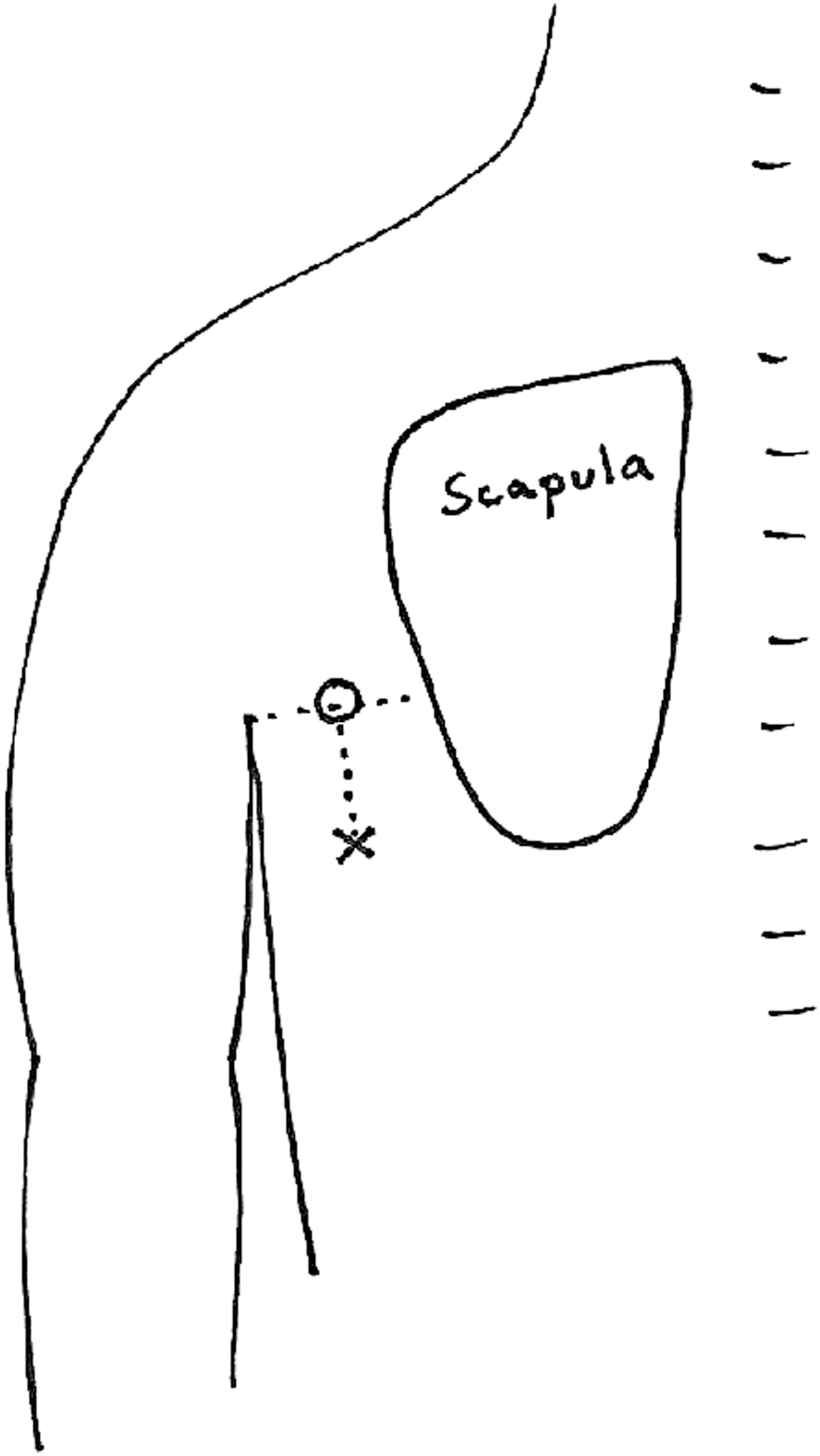
Measurement site at lateral thorax was defined at a spot 5 cm below (caudal) the line drawn between the highest point of the fold between arm and body, and the lateral scapula edge.
To eliminate individual differences in tissue water content, the TDC ratio between the affected and healthy breasts was calculated for each measurement site. The TDC threshold ratio for breast edema was defined as a TDC ratio ≥1.40, 10 ≥1.45 for the upper arm, 12 and ≥1.35 for the lateral thorax. 7
Experiences of tightness, heaviness, and pain in the affected breast were each self-scored by patients on a 100-mm horizontal Visual Analogue Scale (VAS). The end points were “no discomfort” (0 mm) and “worst imaginable” (100 mm).
BMI was calculated at start of study based on measured body weight and length.
At start of study, pressure of the bra was measured by the primary investigator (K.J.) using a device (Kikuhime; TT Meditrade, Denmark) and a sensor that was placed in the position of the third quadrant (lower lateral) of the breast.
Data concerning previous cancer treatment were collected from patients' medical records.
Statistics
Descriptive statistics of baseline variables include rates for binary variables and median and interquartile ranges for continuous variables. Nonparametric tests for continuous variables were used because the groups were small, and values did not exhibit Gaussian distribution. Data were compared between the IG and CG using Mann–Whitney U test, and within groups using Wilcoxon sign rank test. Chi-square exact method was used to compare binary outcomes. A two-sided significance level of 0.05 was applied.
Results
There were no serious adverse events related to the intervention. Slight adverse effects were reported by some patients who considered compression from the bra to have caused discomfort. Baseline data for the TDC values, TDC ratios, and patients' scoring of tightness, heaviness, and pain in the breast were not statistically different between the groups (Tables 2 and 3).
Median (q1–q3) and Mean ± Standard Deviation for Tissue Dielectric Constant Values and Tissue Dielectric Constant Ratio, Pre- and Postintervention with Compression Treatment (I, n = 28) or No Treatment (C, n = 28) for Breast Edema
Within groups, Wilcoxon sign rank test.
RT, radiotherapy; TDC, tissue dielectric constant.
Median (q1–q3) Scores of Tightness, Heaviness, and Pain in the Breast on a Visual Analogue Scale, by Intervention (n = 28) with Compression Treatment or Controls (n = 28) with No Treatment for Breast Edema
No. of patients with symptoms.
Within groups, Wilcoxon sign rank test.
VAS, Visual Analogue Scale.
Local tissue water
TDC values
After intervention, no differences were found between the groups concerning TDC values. In the two groups, a significant reduction in TDC values was found in breast and lateral thorax in the RT side (Table 2). In the non-RT side, a slight reduction was found for breast TDC values in the CG and for lateral thorax TDC values in the IG.
TDC ratio
The mean TDC ratio for all patients was 1.73 ± 0.2, 1.04 ± 0.16, and 1.04 ± 0.08 at start of study, and 1.49 ± 0.28, 1.03 ± 0.12, and 1.04 ± 0.07 at end of study, in the breast, upper arm, and lateral thorax, respectively.
At start 10.7% and at end 7.1% of patients had a TDC ratio >2.0, illustrating 100% edema compared with the anatomically equivalent contralateral side.
After intervention, no differences were found between the groups at different sites concerning the TDC ratio. In both groups, a significant reduction was found for TDC ratio related to breast (Table 2). At end of study, the TDC ratio was <1.40 in 16 patients (55%) in each group.
One patient had lymphedema in the upper arm at the beginning of study (TDC ratio 1.48) and a borderline value at end of study (TDC ratio 1.40). No lymphedema was found at the lateral thorax. Hence no analysis of association between breast edema and edema in arm or lateral thorax was performed.
Experiences of tightness, heaviness, and pain
Tightness, heaviness, and pain were experienced in 48.2%, 41.1%, and 53.6% of all patients at start of study, and in 25.0%, 23.2%, and 33.9%, respectively, at end of study.
At start, tightness, heaviness, and pain were scored >50 on the VAS in 5.4%, 1.8%, and 7.1% and at end in 0%, 3.5%, and 7.1% of patients.
After intervention, no differences were found between the groups concerning VAS scoring of tightness, heaviness, and pain. Scores for feeling of heaviness decreased significantly (>0.05) within both groups. No change within group was found for feeling of tightness or pain, but pain increased in the IG, but not significant (Table 3).
Pressure of the bra was 9–11 mmHg in the sports bra and 2–3 mmHg in the ordinary bra.
Discussion
Breast compression treatment evaluated in this study showed no effect. When comparing outcomes at start and end of study, we found no differences between the IG and CG in tissue water content in the skin or the patient's experience of tightness, heaviness, and pain in the breast. However, both groups showed significant reduction of feeling of heaviness in the breast at end of study.
Edema origin
The present study was based on the hypothesis that breast edema had a similar origin as breast cancer-related arm lymphedema, which can be successfully treated with compression garments. 9 Thus, a larger reduction of edema could be expected in the IG. However, similar results with decreasing edema in both groups rise the question if breast edema consists of edema of different origins. Edema created by lymph node dissection with damage to lymphatic vessels may be impossible to distinguish from RT-induced edema (also called delayed acute reaction in radiation oncology) typically 3 months post-RT. This theory is supported by the fact that the TDC ratio was high both in 77% of SLNB patients (mean TDC ratio 1.73) and in 23% of ALND patients (mean TDC ratio 1.74), implying that axillary nodes dissected did not increase the risk of edema in the breast, as could be expected based on the results of risk evaluation for arm lymphedema. 13
Though the TDC ratio significantly reduced from mean 1.73–1.49 in the whole group, still more than half of the patients, equally divided between both groups, had a TDC ratio >1.4 (set as threshold to determine breast edema) at end of study. The reason for this kind of long-lasting edema is unknown at present. In contrast, at the same time, only about 25% of patients experienced tightness or heaviness in the breast, and none scored >50 on the VAS for tightness, and only 3.5% for heaviness, implying that the experienced symptoms at 3 months post-RT were very much fading away. Also, the significant reduction of heaviness in both groups supports these findings.
For patients still experiencing problematic heaviness, a more extensive examination could be performed, such as evaluating, for example, fibrotic tissue followed by specialist treatment.
It should also be noted that high scoring of pain (>50 on VAS) did not change during the study, indicating that pain may have a completely different origin than tightness and heaviness, such as, for example, nerve injury due to surgery. In the IG, even an increase of pain was found, but not significant, suggesting that a high pressure from the bras may impair the feeling of pain.
Breast edema treatment
At the end of 1 year post-RT, the mean TDC ratio was still high (1.49), indicating that edema was still superficially present in the breast. If the compression pressure applied had been even higher than was achieved by a sports bra of compression type, there may have been a possibility to reduce breast edema in the IG compared to the CG. In contrast, to fully compress the breast is very hard to manage and requires firm garments or bandaging, and in some cases, where the breast is large, it may even be impossible. A higher compression with firm material would most likely lead to discomfort and may even increase pain. One should then also take into account that the rather low rates of tightness and heaviness in the breast at 1 year post-RT, in both groups, imply that edema for most patients was not a big problem. Thus, the assumed reduction of edema from a higher compression would probably not have been in proportion to the negative impact on comfort.
Beside breasts and arms, also a lateral thoracic measurement was made based on the clinical experience that the area posterior to the axilla often has increased thickness in the skin and subcutaneous tissue, compared to the contralateral side, implying that an edema may be present. This has recently been shown by Mayrovitz et al. 7 by TDC measurements. Though there was no lymphedema at the lateral thorax (i.e., TDC ratio <1.35), a significant reduction in TDC values was found in both groups at end of study, implying a similar decrease in tissue water as was detected in the breast. The cause of a significant reduction is most likely the pressure from any bra, not in particular a sports bra, on the skin. Further, the firmness of ribs just beneath the tissue in this area may support the effectiveness of compression. The firmness of ribs is just the same beneath the breast, but the breast is much softer and instable, compared to the skin. This may explain why compression may not work, as discussed above due to the difficulties in achieving effective compression.
No serious adverse effects were reported; however, slight adverse effects were reported by some patients due to excessive compression from the bras causing discomfort, even if the bras were fitted for each woman. Based on clinical experience, some women with breast edema find sports bras comfortable to wear, in particular during a period when the heaviness of the breast is large.
Experienced problems
The literature has called attention to problems experienced by patients such as tightness, heaviness, and pain1,2 in the breast following breast cancer treatment with surgery and RT. Though all patients in the present study had breast edema, diagnosed by a high TDC ratio, only about half of the patients experienced symptoms at start of intervention 3 months after completion of RT, where few scored >50. This may imply that large problems concerning edema are only experienced by a few patients.
A variety of treatments for breast edema have been recommended to patients. However, the success of these treatments is most likely a result of the normal course of breast edema development with a natural and progressive decrease in associated inflammation. Though some patients may have large problems during the first months after RT, these problems, in most patients, will substantially reduce or disappear during the following months. Therefore, patients should be informed that the experienced symptoms most likely will diminish within months. When the symptoms are significant, a firm bra may diminish the feeling of, in particular, heaviness. However, this should not be mixed up with the feeling that the edema is “treated.”
Strengths and limitations
A limitation of the study may be that no prior data were available for power calculations; hence no such calculation could be performed. Therefore, this study was considered a pilot study with a limited number of included patients. However, a strength is that the study design was an RCT. Data from this study can serve as a source for future power calculations in repeated studies. Moreover, results from both groups are very similar, and it is not likely that a larger number of patients would be able to show any significant difference between the groups.
Conclusion
No effect of 9-month compression treatment with sports bras compared to ordinary bras for breast edema at 3 months post-RT could be found, assessed by tissue water content and experienced symptoms. Most likely, breast edema was resolving similarly in both groups. Thus, patients should be informed of the normal course of breast edema development, particularly that symptomatic problems soon after the completion of RT will substantially reduce within a year.
Footnotes
Acknowledgment
This study was supported by research grants from the Swedish Cancer Foundation and the Swedish Breast Cancer Association, and it was made possible by the women who generously gave up their time to participate. Thanks to physiotherapist Viveka Fredlund for assisting with measurements.
Author Disclosure Statement
No competing financial interests exist.