
Abstract
Background:
Lymphedema of the breast/chest wall after breast cancer treatment is often associated with pain and reduced quality of life. We conducted a pilot study to evaluate whether the use of a compression vest reduced symptoms of breast/chest wall edema in breast cancer patients.
Methods and Results:
This single-center study included patients (n = 25) with symptomatic breast/chest wall edema with a pain score of ≥3 on the Numerical Rating Scales (range 1–10). The patients were instructed to wear a compression vest (Lymphatrex, Class II) for 6 months. Wilcoxon signed-rank tests were used to compare differences in patient-reported pain intensity/severity. Analyses included all patients with available data. In total, 17 (68%) continued to wear their vests for 6 months, whereas the other 8 withdrew prematurely. At baseline, median pain severity (4.9, interquartile range [IQR] 3.6–6.0) and pain interference (4.3, IQR 2.1–5.9) scores were significantly higher compared with pain scores after wearing the compression vest for 6 months (1.8 IQR 1.0–4.8 and 1.4 IQR 0.9–4.4, resp.). Patient-reported breast/chest wall swelling decreased from 92% (n = 22) at baseline to 71% (n = 12) at 6 months. The prevalence of moderate/severe patient-reported breast/chest wall pain declined from 63% (n = 15) at baseline to 18% (n = 3) at 6 months. Physical, emotional, and social functioning improved over time and was comparable to scores of the Dutch reference population.
Conclusion:
The results of this pilot study suggest that a compression vest could be an acceptable and effective treatment option for patients with painful breast/chest wall edema. In compliant patients, swelling and pain was significantly reduced.
Introduction
Over the past decades, breast cancer treatment has improved, leading to a growing number of breast cancer survivors.1–4 This growing population has resulted in an increased focus on survivorship and the management of acute and late toxicities after breast cancer treatment. Breast cancer-related lymphedema is still a major complication after treatment.5–7 Over the past years, lymphedema of the arm has been extensively described; whereas edema of the breast or thoracic wall has received less attention.8,9 Especially with the large proportion of patients opting for breast-conserving therapy nowadays, edema of the breast/chest wall is an increasingly common complication.9–13
Patients suffering from breast or thoracic wall edema often report chronic pain after breast cancer treatment, which could be caused by lymphedema or by other morbidity after breast cancer treatment. Lymphedema may also cause body image disturbance, social and physical morbidity, which could be important reasons for reduced health-related quality of life (HRQOL).14–17 Therefore, efforts to prevent and treat breast edema are important.18,19 Current standard therapy for breast/chest wall edema consists of manual lymphatic drainage and taping by a lymphedema therapist. 20 However, evidence of effectiveness is limited and standard therapy for breast/chest wall edema does not yet exist.21–25 A disadvantage of manual lymphatic drainage is that therapy is time consuming and has to be applied regularly by a lymphedema therapist. An attractive alternative or additional option could be compression treatment with elastic compression garments. Compression has been described as a key component in treatment of lymphedema, since elastic compression vests can exert continuous pressure on the edematous breast/chest wall.15,23,26 Apart from reducing symptoms, compression vests have the potential to improve self-efficacy and self-management in patients. 27 The aim of the present pilot study was to evaluate the effect of compression treatment in patients suffering from breast cancer-related breast/chest wall edema.
Methods
Participants
Between January 2016 and June 2017, patients with symptomatic lymphedema of the breast/chest wall after breast cancer treatment were recruited to wear a tailored compression vest (Thuasne®). The study was approved by the Medical Research Ethics Committee of the University Medical Center (UMC) Utrecht, The Netherlands, and registered on clinicaltrials.gov (NCT02070146).
The study included women with pain of the breast/chest wall on a 10-point Numerical Rating Scale of three or higher and the presence of breast/chest wall edema at inclusion. Patients were deemed ineligible if they were younger than the age of 18, pregnant, unable to understand the Dutch language, indicated to undergo radiation treatment of the breast/chest wall within the next 6 months, suffering from cardiac or pulmonary complaints, and had nonbreast cancer-related lymphedema or clinical depression or anxiety disorder. After informed consent, patients received a Class II Lymphatrex compression vest (Thuasne), which they were recommended to wear at least 4 days a week, 6 hours a day (Fig. 1). It was explained to patients that wearing the vest beyond the recommended period might maximize the effect of the compression vest. All vests were custom-made (measures were taken by a skilled nurse), taking into account the circumference under the breast and right cup size. In case of mastectomy, seamless, (bilateral) pockets for the breast prosthesis were made.
Custom-made thuasne lymphatrex, Class II compression vest.
Breast/chest wall edema was diagnosed by a surgeon, radiation oncologist, physician assistant, or nurse practitioner according to the Common Terminology Criteria of Adverse Events (CTCAE) v4.03 (Supplementary Table S1). The CTCAE criteria for scoring edema of the breast/chest wall have been in use at the Department of Radiation Oncology for many years and were measured on a scale from 0 (no edema) to 3 (severe symptoms of edema, limiting self-care). However, at the Surgery Department, scoring edema according to CTCAE criteria was uncommon. Therefore, to evaluate agreement in CTCAE scoring of breast/chest wall edema, an interobserver study and training was performed before the start of the study. Breast cancer patients (n = 47) visiting the Surgery Department or the Department of Radiation Oncology during or after breast cancer treatment were invited randomly to participate in the sub-study, irrespective of the presence of lymphedema. The breast/chest wall of each participant was independently scored by a caregiver from the Radiation Oncology Department and by a caregiver from the Surgery Department according to the CTCAE criteria. All observers (i.e., surgeons, radiation oncologists, nurse practitioners, and physician assistants) were specialized in treating breast cancer patients. Interobserver agreement between surgical and radiation oncology caregivers was assessed before a CTCAE scoring training session and afterward.
Data collection
Patient-, disease-, and treatment characteristics of this study were collected on inclusion and at regular follow-up consultations at the UMC Utrecht. Visits were scheduled before the start of compression treatment (i.e., baseline) and at 1, 3, and 6 months thereafter. During these visits, breast examination was performed by the radiation oncologist, physician assistant, nurse practitioner, or surgeon, including assessment of the degree of breast/chest wall edema according to the CTCAE v4 criteria. Additional photos of the breast/chest wall were taken by a medical photographer.
For the interobserver sub-study, the CTCAE score for each patient was independently obtained by two different observers from different specialties, that is, surgery (surgeons or nurse practitioners) or radiation oncology (radiation oncologists or nurse practitioners). Observers received basic patient information, including age, date of surgery, tumor type, (neo)adjuvant treatment, hormonal treatment, lymph node dissection, axillary staging of breast cancer, radiation therapy, and chest/breast wall pain.
Patient-reported outcomes on HRQOL and pain were assessed at baseline, at 2 weeks, and 1, 3, and 6 months afterward with standardized questionnaires of the European Organization for Research and Treatment of Cancer (EORTC QLQ-C30/BR23). 28 To identify patient-reported breast/chest wall swelling and pain, two specific questions were analyzed (i.e., EORTC QLQ-BR23 question 50: “During the past week: Have you had any pain in the area of your affected breast?” and EORTC QLQ-BR23 question 51: “During the past week: Was the area of your affected breast swollen?”). The Brief Pain Inventory (BPI) was used to measure pain severity and pain interference with daily function. The BPI uses 0 (“no pain”) to 10 (“pain as bad as I can imagine”) numeric rating scales. 29 Assessments included current pain, pain at its worst, least, and average in the past 3 days that results in a pain severity score. Moreover, pain interference was measured by seven single questions (effects on general activity, mood, walking ability, normal work, relations with other people, sleep, and enjoyment of life). 29 HRQOL outcomes of women participating in this study were compared with those of a cohort of women from the Dutch general population (n = 832, median age 55 years) without a history of breast cancer. 30
Statistical analysis
Patient-, tumor-, and treatment characteristics were described by using frequencies and percentages. Continuous data were summarized by using medians and interquartile ranges (IQR). Differences between patients who completed the 6-month study period (i.e., compliant) were compared between patients who were unable to fulfill the study period (i.e., noncompliant). Differences between these patients were not tested due to small sample sizes. Patient-reported pain severity and intensity were compared between baseline (i.e., before start of the compression vest) and follow-up moments. The null hypothesis consisted of no changes in patient-reported pain from baseline. The Wilcoxon signed-rank tests for non-normally distributed data was used. The level of significance was set at p < 0.05. Analyses were done in both the complete cases, which excluded patients who did not complete the 6-month study period, and the available cases, which included all patients who received a tailored compression vest at baseline and the available data at each time-point. All described analyses are in patients with available data at each time-point.
HRQOL data were handled according to the EORTC QLQ-C30 manual. 28 Scores were linearly transformed into scores ranging from 0 to 100 and used as continuous outcomes. Higher scores indicate better functioning.
In the interobserver sub-study, the interobserver agreement for scoring breast/chest wall edema according to CTCAE v4.03 was measured by calculating kappa (κ) scores between two different observers (i.e., one observer from the Surgery Department and one from the Department of Radiation Oncology). Kappa score is a measure of the level of agreement beyond chance alone. Kappa values were interpreted as suggested by Landis and Koch:, that is, 0.20 or less indicated poor reliability; 0.21–0.40, fair reliability; 0.41–0.60, moderate reliability; 0.61–0.80, substantial reliability; and 0.81–1.00, excellent reliability. 31
Statistical analyses were performed with the Statistical Package for Social Sciences (SPSS) for Windows, version 23 (IBM Corp, Armonk, NY).
Results
Breast edema study
A total of 24 breast cancer patients were enrolled between January 2016 and May 2017 and started wearing the compression vest (Thuasne). One woman withdrew before the start of compression treatment, and seven patients (29%) did not complete the full 6-month study period (i.e., noncompliance). Different reasons for not wearing the vest were reported (see Table 1 for details). In total 17 patients (71%) who started compression treatment (vest) wore the vest during the complete study period (i.e., 6 months).
Patients’ Quotations Regarding Noncompliance of the Vest and the Reason for Dropping Out of the Study (n = 8)
The median age of all included patients (n = 24) was 60 years (IQR 50–64 years). All patients underwent breast cancer surgery and postoperative radiotherapy between June 1994 and January 2017, of whom 14 (58%) were treated with breast-conserving surgery and 42% with mastectomy (Table 2). Axillary lymph node dissection was performed in 42% of the patients (n = 10), and the majority of women were treated with adjuvant hormonal therapy (n = 15, 63%). Differences in patient-, disease-, and treatment characteristics were observed between noncompliant and compliant women. Noncompliant patients differed from compliant patients with respect to neo-adjuvant chemotherapy (43% vs. 12%), adjuvant hormonal treatment (86% vs. 53%), mastectomy (71% vs. 29%), axillary lymph node dissection (71% vs. 29%), and axillary radiotherapy (Supplementary Table S2).
Baseline and Treatment Characteristics of Included Patients
Data are median (IQR) or n (%). Some percentages do not total 100 because of rounding.
Axillary lymph node dissection with or without preceding sentinel node biopsy.
BMI, body mass index; IQR, interquartile range.
Physician-reported edema according to Common Terminology Criteria of Adverse Events
At baseline (before start of the compression vest) and at 1 month after start, 96% (n = 23) of the women presented with slight-to-moderate physician-reported breast/chest wall edema (CTCAE grade 1 and 2). At baseline, one patient had severe edema (CTCAE grade 3). Three and 6 months after the start of compression therapy, a decrease in slight/moderate edema (CTCAE grade 1/2) was observed, 89% (n = 16) and 87% (n = 13), respectively. At 6 months, two patients had no physician-reported lymphedema anymore (CTCAE grade 0).
Patient-reported edema
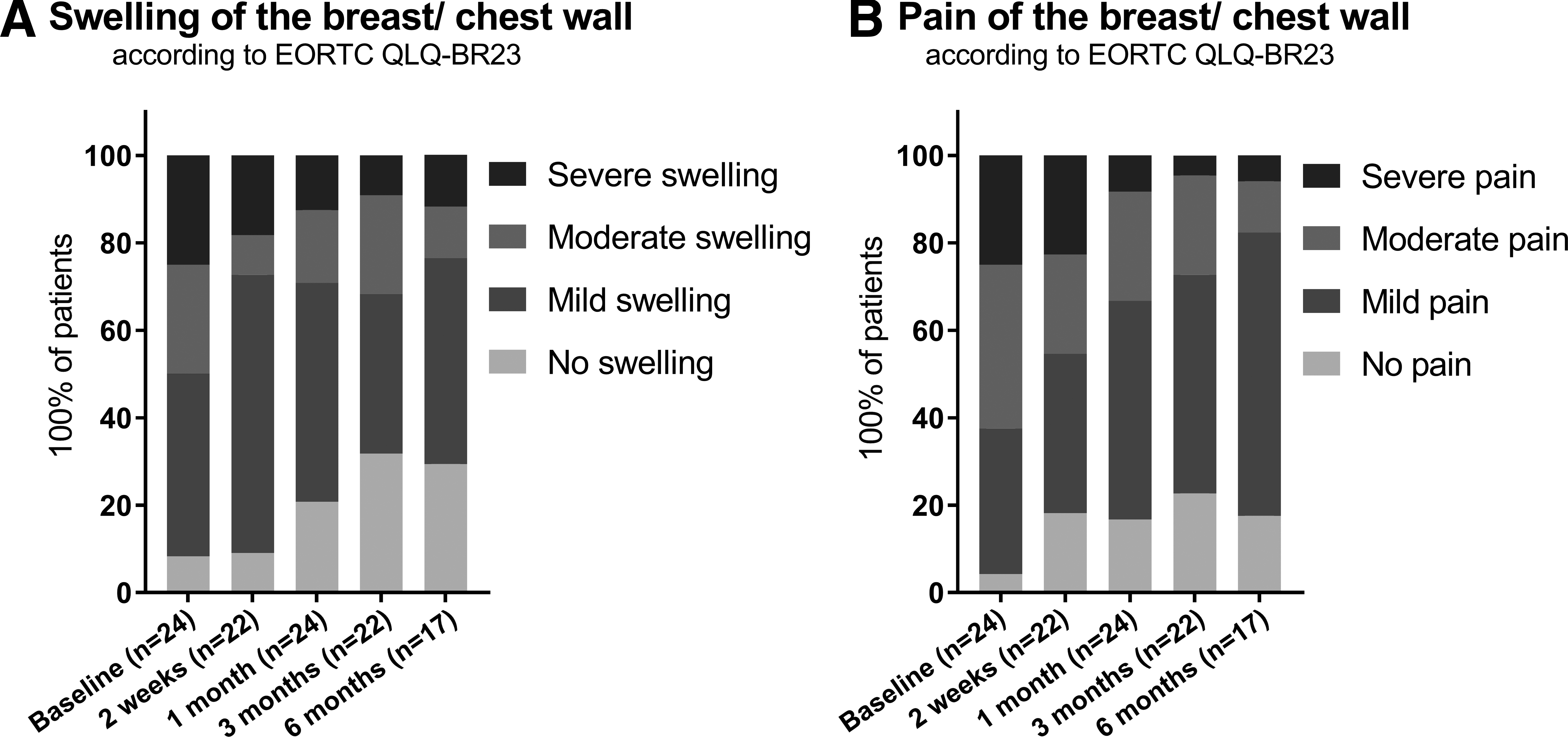
In total, 22 (92%) patients reported breast/chest wall swelling at baseline, of whom 6 reported severe swelling of the breast/chest wall. After 6 months, only two patients still reported severe swelling of the breast/chest wall (Fig. 2A).
Patient-reported swelling
Patient-reported pain
Breast/chest wall pain was present in 23 patients (96%) at baseline, of whom 25% (n = 6) suffered from severe breast pain (Fig. 2B). At 3 months, after the start of compression vest therapy, the highest proportion of patients (32%, n = 7) reported complete breast/chest pain relief. The proportion of patients suffering from moderate or severe breast/chest wall pain was lowest (n = 3, 18%) at 6 months.
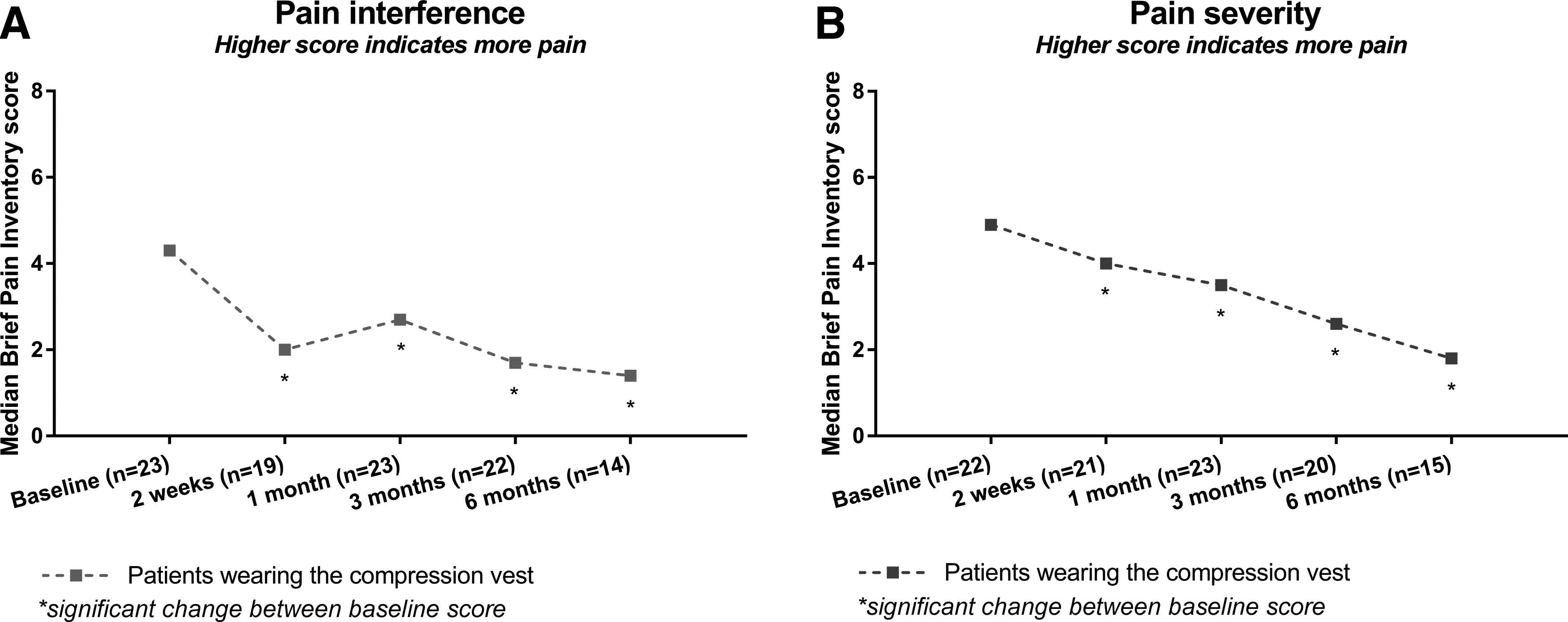
Pain interference assessed with the BPI decreased over time (Fig. 3A). Wilcoxon signed-rank test showed that wearing the compression vest resulted in a statistically significant decrease in pain interference at 6 months (median = 1.4 IQR 0.9–4.4), compared with baseline (median = 4.3 IQR 1.9–5.1), in women with symptomatic breast/chest wall edema (Z = −2.6, p = 0.009, Fig. 2). In comparison with pain severity at baseline (median = 4.9 IQR 3.6–6.0), there was a decrease over time. Similar to pain interference, severity scores were lowest at 6 months (median = 1.8 IQR 1.0–4.8) compared with baseline (Z = −3.3, p = 0.001, Fig. 3B).
Median patient-reported pain interference
Quality of life
Over time, an improvement in quality of life, as well as in physical-, role-, and social functioning improved to similar levels of the age-matched reference population during and at 6 months after the start of compression treatment (Supplementary Fig. S1).
Interobserver agreement CTCAE
Reproducibility of CTCAE criteria for breast/chest edema was measured in a sub-study in 47 breast cancer patients with a total of 94 CTCAE scores. In the first 23 patients, overall interobserver agreement of CTCAE score for breast/chest wall edema between raters was poor (κ = 0.066, 95% confidence interval [CI] −0.098 to 0.230) in CTCAE scores. After establishment of a consensus meeting and training with all observers, the CTCAE criteria for breast edema were extensively discussed and adapted (Supplementary Table S1). The interobserver agreement scored in the next 24 patients increased slightly from poor to fair (κ = 0.248, 95% CI 0.068–0.428) and the overall agreement was 58% (Table 3).
Interobserver Agreement on Breast/Chest Wall Edema Before the Consensus Meeting and After the Consensus Meeting Regarding the Common Terminology Criteria of Adverse Events v4 Criteria
No. of patients.
Discussion
This study showed that a compression vest may be an acceptable treatment option in reducing breast pain and swelling in patients suffering from breast cancer treatment-related breast/chest wall edema. When compliant for 6 months, the use of a compression vest may improve patient-reported pain and swelling of the breast/chest wall. Within a study period of 6 months, the largest decrease in swelling and pain was reported within the first 3 months after the start of using the compression vest. For one-third of the patients, the vest was not a well-acceptable treatment option, especially for patients experiencing (pre-existent) hot flushes.
Breast/chest wall edema is a well-known and often persistent complication that can cause pain and compromise HRQOL. To date, there is no consensus on the definition of breast/chest wall edema.32,33 The lack of definition leaves this type of edema underdiagnosed and, therefore, often untreated in clinical practice. Before this study, we performed an interobserver agreement study of CTCAE scoring of breast/chest wall edema by caregivers. The results showed low overall agreement on the CTCAE v4.03 criteria for scoring and diagnosing edema between professionals. Consequently, clinical assessment as an objective diagnosis of breast/chest wall edema is insufficient. Patient-reported breast/chest wall edema may be more valuable in identifying edema, as the patients’ perceptions are the most important outcomes for individuals and are correlated strongly with signs of breast edema. 11 In 2015, patient-reported CTCAE (PRO-CTCAE) scores were developed to integrate the patients’ perspective into adverse event reporting. 34 However, data on breast edema as assessed with this instrument are not yet available. Future studies could compare breast edema outcomes assessed by PRO-CTCAE with PROs from the EORTC QLQ-BR23 questionnaires, to determine which patient-reported outcome instrument is the most sensitive in diagnosing breast/chest wall edema.
Moreover, the CTCAE score for breast/chest wall showed very little changes over time, whereas patient-reported swelling of the breast/chest wall decreased in the first months after compression treatment. Alongside swelling of the breast/chest wall, pain (i.e., pain severity, pain interference, and breast/chest wall pain) also decreased, which might be clinically most important from the patients’ perspective. Especially, patient-reported breast/chest wall pain is relevant for patients, as pain severity/intensity may also be caused by other factors (e.g., pain from arm lymphedema or joint pain from endocrine treatment).
Previous studies have reported encouraging effects of compression therapy on breast cancer-related lymphedema of the arm.21,32,35,36 Compression of the limb (i.e., compression sleeve) is a well-established treatment option in improving the lymph outflow and decreasing arm edema.19,37 As pressure applied on the swollen tissue improves the lymphatic and venous circulation, compression therapy in women with breast/chest wall edema theoretically seems useful. However, the role of compression in the breast and chest area, which is the primary area where surgery and radiotherapy is performed, is less clear and studies on effective treatment for breast edema are limited. Hansdorfer-Korzon et al. examined the efficacy of a compression corset for the treatment of chest lymphedema in 29 breast cancer patients with edema of the breast/chest wall. 38 All patients were treated with surgery (i.e., mastectomy or breast-conserving). They found that wearing a compression corset (not custom made) for the course of 6 months reduced the thickness, measured by ultrasound, of the subcutaneous breast tissue. At 6 months, patients were asked to rate the comfortability of the compression garment. All patients rated the compression corset comfortable and the breathability of the corset sufficiently. 38
The small number of patients participating in this pilot study limited further analysis on patient and treatment factors associated with good response to compression treatment. Our results suggest that wearing a compression garment for the course of 6 months is not acceptable for all patients. Systemic therapy (e.g., hormonal and/or chemotherapy) might negatively impact the compliance to compression treatment (i.e., vest), most probably because of hot flushes. Also, compression treatment might be less effective in patients with more advanced tumor stages for whom extensive breast cancer treatment is required (i.e., axillary lymph node dissection and/or systemic treatment and/or locoregional radiotherapy), since noncompliance was highest in these patients. The highest dropout of the study was seen at 3 months. It might be that at this time-point, the effect of the vest is achieved, and the burden of the vest no longer outweighs the effect of compression therapy. No recommendation exists on treatment duration but based on these results, we would suggest wearing the vest 3 months and extending the use in case of no, satisfying, clinical response. Also, compression vests from a more breathable material might lead to a more comfortable vest and improve compliance. Besides, the high level of pressure might result in noncompliance, and there is no consensus yet on the required level of pressure to effectively treat chest/wall edema; although results of this study show that a Class II compression vest is effective, it could be that less pressure is more comfortable for patients.
In this study, we have chosen to allow patients to continue other edema reducing treatments while wearing the edema vest, to evaluate the role of the vest in an uncontrolled, routine care setting. Based on the rather promising results of this pilot study, randomized controlled trials are necessary to objectify and confirm the effects of compression corsets in patients with breast/chest wall edema in comparison to other edema treatment options and/or no treatment. In these trials, in addition to patient-reported outcomes, objective edema measurements using ultrasound could be considered. The efficacy of treatment should be evaluated by using patient-reported outcome measures, since the interobserver agreement on edema scoring was low.
The compression vest was not well tolerated by 32% of patients with breast/chest wall edema. Still, results of this study underline that treatment with a compression vest could be discussed with patients during shared decision making, especially when patients do not benefit from standard treatment for lymphedema such as manual lymphatic drainage and taping by a lymphedema therapist.
In conclusion, results of this study suggest that a compression vest could be an acceptable and effective treatment option for patients with symptomatic breast/chest wall edema. In patients wearing the vest for the course of 6 months, breast/chest wall swelling and pain declined and HRQOL improved to comparable levels of age-matched women without a history of breast cancer.
Compliance with Ethical Standards
Funding: This study was partly funded by Thuasne (we received 20.000 euro).
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: Informed consent was obtained from all individual participants included in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.