
Abstract
Background:
Acquired lymphedema is a common consequence of cancer surgery. Fibrosis is one of the main causes of chronic lymphedema since it hinders lymphatic regeneration and this causes a significant decrease in lymphatic flow and accumulation of excessive protein-rich fluid. The transforming growth factor-β1 (TGF-β1) signaling pathway is known in a process of wound repair and fibrosis. In our study, the purpose was to evaluate the efficacy of EW-7197, a peroral TGF-β type I receptor kinase inhibitor, in treating acquired lymphedema.
Methods and Results:
For lymphedema mouse tail model, we used 10- to 12-week-old female C57BL/6 mice. The skin was circumferentially excised, making a circular band followed by cauterization of lymphatic collecting vessels. Two groups were made in this study: control and treatment. The treatment group (n = 12) received a solution consisting of 0.1 mL of artificial gastric juice and 20 mg/kg EW-7197 by gavage once daily. For evaluation, tail diameter measurement, fluorescence lymphography, and immunofluorescence images were used. EW-7197 treatment ameliorates acquired lymphedema in a mouse tail model by increasing lymphangiogenesis and interstitial flow of the lymphatics by inhibition of the fibrosis. The differences in maximal tail thicknesses between the control and treatment groups were statistically significant from 2 to 4 weeks after surgery. The treatment group showed a greater number of lymphatic vessels at the surgery site than the control group. The treatment group also showed more FITC coverage area at the surgery site.
Conclusion:
EW-7197 treatment ameliorates acquired lymphedema in a mouse tail model by increasing lymphangiogenesis and interstitial flow.
Introduction
Acquired lymphedema is a relatively common consequence of cancer surgery. 1 The major lymphatic system is damaged following cancer surgery with or without radiotherapy, causing a significant decrease in lymphatic flow and accumulation of excessive protein-rich fluid. If lymphatic flow is restored by reconnecting disoriented lymphatic vessels, the lymphedema could be successfully recovered, but if not, chronic lymphedema occurs. 2
Fibrosis is one of the main causes of chronic lymphedema, as it hinders lymphatic regeneration.3,4 Pathological studies of fibrosis in relation to lymphatic regeneration have been the focus of intense investigation and new treatment strategy for chronic lymphedema. Some of these studies have shown that transforming growth factor-β1 (TGF-β1), one of the important regulators of fibrosis, plays a key role in lymphatic regeneration during wound repair.3–6 TGF-β1 is a member of the TGF-β superfamily that takes an important role in homeostasis of epithelial, endothelial, and hematopoietic cells. It promotes mesothelial-to-mesenchymal transition and results in inducing tissue fibrosis during wound repair process. 7 Avraham et al. 3 reported that either systemic or local TGF-β1 blockade using monoclonal antibody treatment significantly improves lymphatic function by promoting lymphatic regeneration and by decreasing fibrosis. 3 However, to date, there have been no lymphedema studies to assess the therapeutic effects of systemic TGF-β1 receptor inhibitor.
EW-7197, N-[[4-([1,2,4]Triazolo[1,5-a]pyridin-6-yl)-5-(6-methylpyridin-2-yl)-1H-imidazol-2-yl]methyl]-2-fluoroaniline, is a highly selective peroral TGF-β type I receptor kinase inhibitor. ALK5, one of the TGF-β1 receptors, phosphorylates SMAD2/3 and triggers several cellular cascades involved in wound repair and fibrosis. Son et al. 8 reported that EW-7197 acts as an ATP-competitive inhibitor of ALK5 by binding to the ATP-binding site. This results in inhibition of the TGF-β1/Smad signaling pathway.
We hypothesized that the administration of a TGF-β type I receptor kinase inhibitor just before or after surgery could prevent the fibrosis process following surgery and thereby ameliorate the resulting acquired lymphedema. Thus, the purpose of this study was to evaluate the efficacy of EW-7197in treating acquired lymphedema in a surgical model of mouse tail. Since a considerable amount of lymphatic fluid is transmitted by interstitial flow through the dermal matrix, 9 both the degree of lymphatic regeneration and interstitial flow were taken into account to evaluate the efficacy of EW-7197.
Materials and Methods
This study was approved by the committee for animal research of our institution and conformed to the U.S. National Institutes of Health guidelines on the care and use of laboratory animals.
Mouse tail model of lymphedema
Tail lymphedema was created in 10- to 12-week-old female C57BL/6 mice (Orient Bio, Seongnam, Korea) as described previously, 10 but with minor modifications. In brief, the mice were anesthetized with an intramuscular injection of 50 mg/kg zolazepam and tiletamine (Zoletil 50; Virbac, Carros, France) and 10 mg/kg xylazine (Rompun; Bayer HealthCare, Leverkusen, Germany), and the skin was circumferentially excised 18-mm distal to the base of the tail, making a 2-mm circular band. The lymphatic collecting vessels were cauterized using Bovie cautery.
EW-7197 treatment
A total of 24 mice were divided into two groups. The control group (n = 12) received 0.1 mL of artificial gastric juice by gavage once daily for 4 weeks. The treatment group (n = 12) received a solution consisting of 0.1 mL of artificial gastric juice and 20 mg/kg EW-7197 phosphate by gavage once daily for 4 weeks. EW-7197 phosphate was provided by the Laboratory of Medicinal Chemistry, College of Pharmacy, Ewha Woman's University (Seoul, Korea). The dosage of EW-7197 phosphate was determined based on prior studies.8,11 All mice were maintained in a temperature-controlled room (22°C ± 2°C) and supplied with food and water ad libitum. For histologic evaluation, mice were sacrificed by carbon dioxide asphyxiation 4 weeks after surgery.
Tail diameter measurements
Digital images were obtained from the mouse tails after surgery twice a week with use of a Canon D550 camera mounted to its tripod. Tail diameter measurements were made from these digital images using ImageJ imaging software (U.S. National Institutes of Health, Bethesda). Maximum tail diameter was measured at the point of greatest diameter distal to the surgery site as described previously. 12
Fluorescence lymphography
We used lysine-fixable FITC-dextran (molecular weight, 2000 kDa; Molecular Probes) fluorescence lymphography tracer to identify lymphatic flow. Five microliters of FITC-dextran tracer was injected intradermally into the distal tail 30-mm distal to the site of the surgery once a week. Digital images were obtained with a microscope-based multispectral imaging system, Nuance™ (PerkinElmer, Inc., Hopkinton, MA) 30 minutes after the injection. The system was mounted onto a conventional fluorescence microscope equipped with a filter cube that comprised a standard excitation filter, dichroic mirror, and a long-pass emission filter.
Immunofluorescence stain was used to detect lymphatic regeneration and interstitial flow on longitudinal cross sections of mouse tail. Six mice in each group were assigned to detect lymphatic vessel regeneration. Immunostaining was performed using antilymphatic vessel endothelial receptor-1 (LYVE-1) to observe physical structures of lymphatic vessels and anti-α-smooth muscle actin (α-SMA) antibodies to observe smooth muscle cells. In brief, mouse tails were harvested 4 weeks after surgery and fixed with 4% paraformaldehyde perfusion fixative (Electron Microscopy Sciences, Hatfield, PA) overnight at 4°C, followed by sequential incubation in 15% and 30% sucrose solution. Fixed samples were embedded in optimal cutting temperature compound, and 5-μm cryostat sections were prepared and collected on slides for double immunofluorescence staining. Before staining, slides were air-dried, then fixed and permeabilized in ice-cold acetone for 10 minutes at −20°C. After fixation and permeabilization, slides were blocked with 10% fetal bovine serum in 1 × phosphate-buffered saline (PBS) with 0.1% Tween 20. Tissue sections were stained with primary antibodies, including rabbit anti-LYVE-1 antibody (1:100, ab14917; Abcam, Cambridge, Cambridgeshire, United Kingdom) and mouse-anti-α-SMA antibody (1:300, ab7817; Abcam) overnight at 4°C followed by washing with PBS with 0.1% Tween 20. After washing, secondary antibody staining was performed using Alexa Fluor 488, Alexa Fluor 594, and 4′-6-diamidino-2-phenylindole (DAPI) (Invitrogen, Burlington, Canada). Slides were then incubated for 1 hour at room temperature.
Six additional mice were assigned to each group to detect interstitial flow. FITC-dextran tracer was injected intradermally into the tip of the tail before sacrifice. Single immunofluorescence staining was performed using anti-α-SMA antibody and Alexa Fluor 594 as described previously. Nuclei were visualized with DAPI.
Digital images were collected using a Panoramic Super-Resolution Confocal microscopy system (3D HISTECH, Budapest, Hungary).
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (SPSS, Inc., Chicago, IL). The maximum diameter of the tail was compared using the paired t-test. Mean FITC coverage area and mean number of vessels per high-power field were compared using the Student's t-test. All p-values were two sided with statistical significance evaluated at the 0.05 alpha level, and 95% confidence intervals were constructed to assess the precision of the obtained estimates.
Results
Tail diameter measurements
The maximum tail diameter was rapidly increased after surgery in both groups, which lasted up to 2 weeks in the control group and 1.5 weeks in the treatment group, respectively (Fig. 1). The differences in maximal tail diameter between the control and treatment groups were statistically significant from 2 to 4 weeks after surgery (6.1 ± 0.5 mm vs. 5.8 ± 0.3 mm, p = 0.046 at 2 weeks; 5.8 ± 0.5 mm vs. 5.4 ± 0.2 mm, p = 0.035 at 3 weeks; 5.5 ± 0.4 mm vs. 5.0 ± 0.3 mm, p = 0.030 at 4 weeks).

Fluorescence lymphography and immunofluorescence
Fluorescence lymphography showed accumulation of the FITC-dextran tracer distal to the surgery site in both groups. The treatment group showed fluid channels at the surgery site 4 weeks after surgery, which were not observed in any of the mice of the control group (Fig. 2).
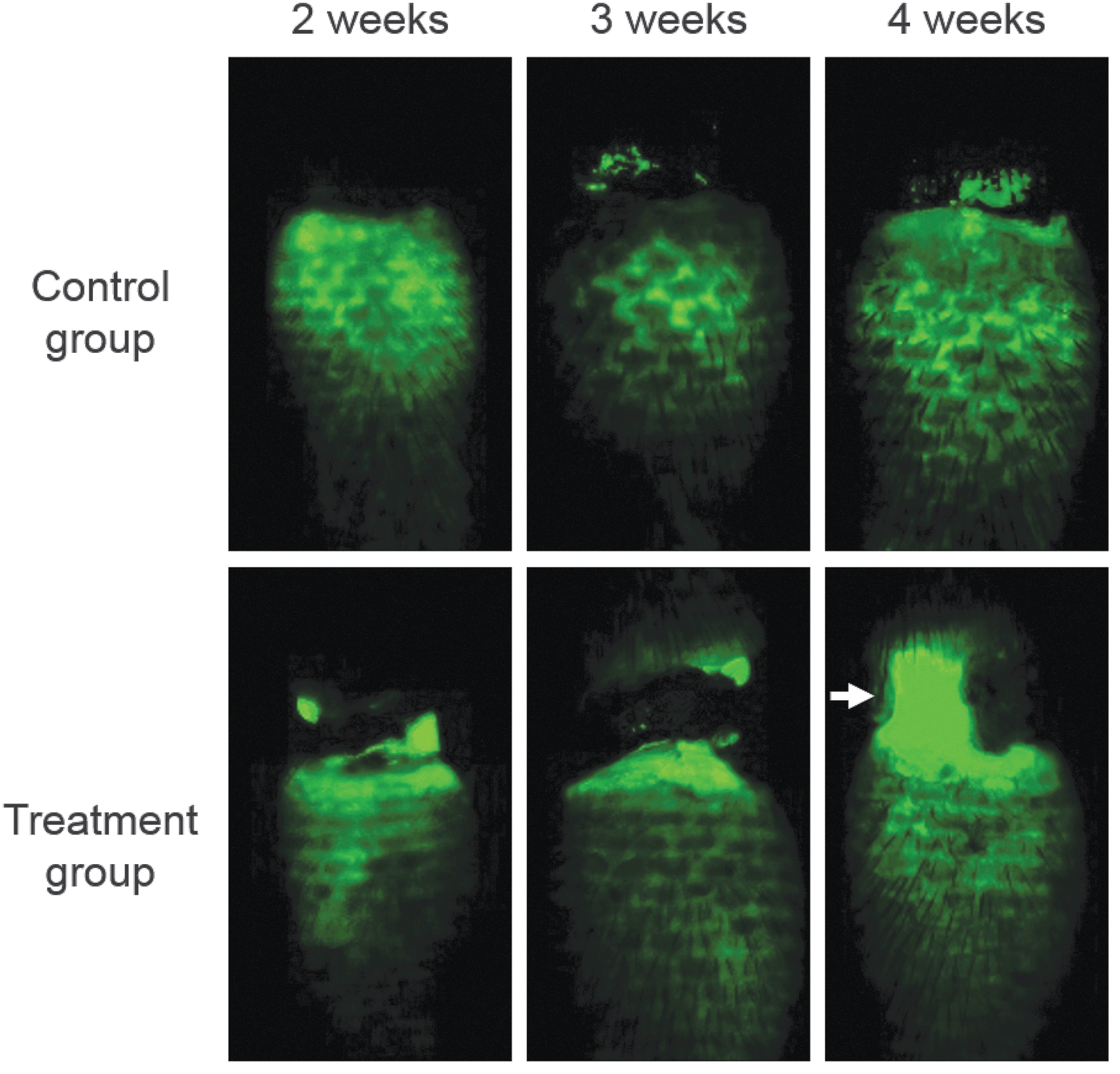
Fluorescence lymphography was used to identify postsurgery lymphatic flow in mouse tails. The treatment group shows a fluid channel (arrow) in the surgery site 4 weeks after surgery, while the control group shows accumulation of the FITC-dextran tracer (2000 kDa) distal to the surgery site with no formation of a fluid channel. Color images are available online.
Regarding α-SMA expression at the surgical site, the treatment group had lower expression than the control group (17.1% vs. 38.5%, p < 0.001). As for lymphatic regeneration, the treatment group showed a larger number of LYVE-1-stained vessels at the surgery site per high-power field (9.9 ± 3.8 vs.1.6 ± 1.3, p < 0.001) (Fig. 3). In terms of interstitial lymphatic flow, the treatment group had greater FITC coverage area at the surgical site than the control group (3.8% ± 1.1 vs. 0.6% ± 0.5, p < 0.001) (Fig. 4).
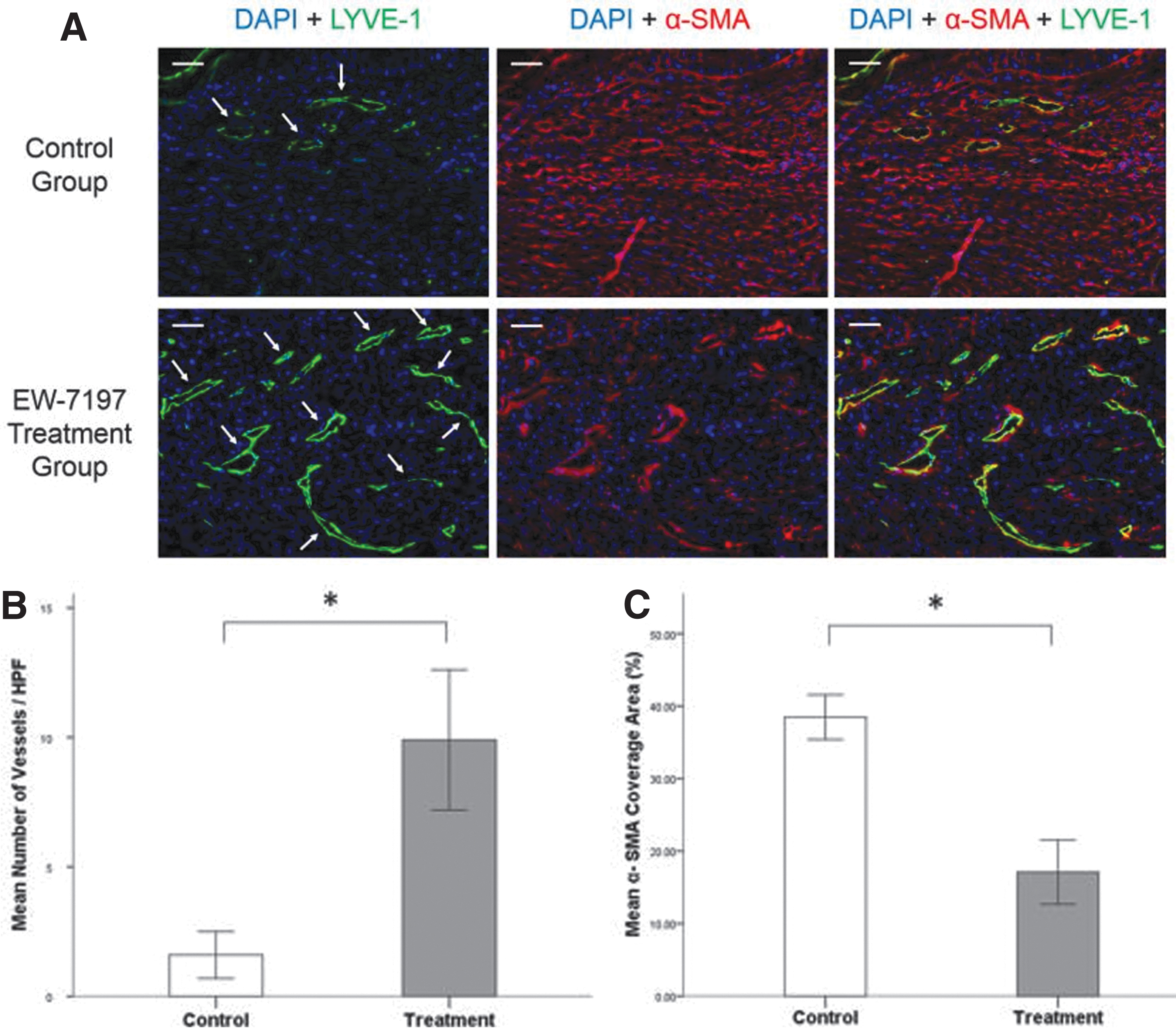
Comparison of postsurgical lymphangiogenesis between the treatment and control groups.
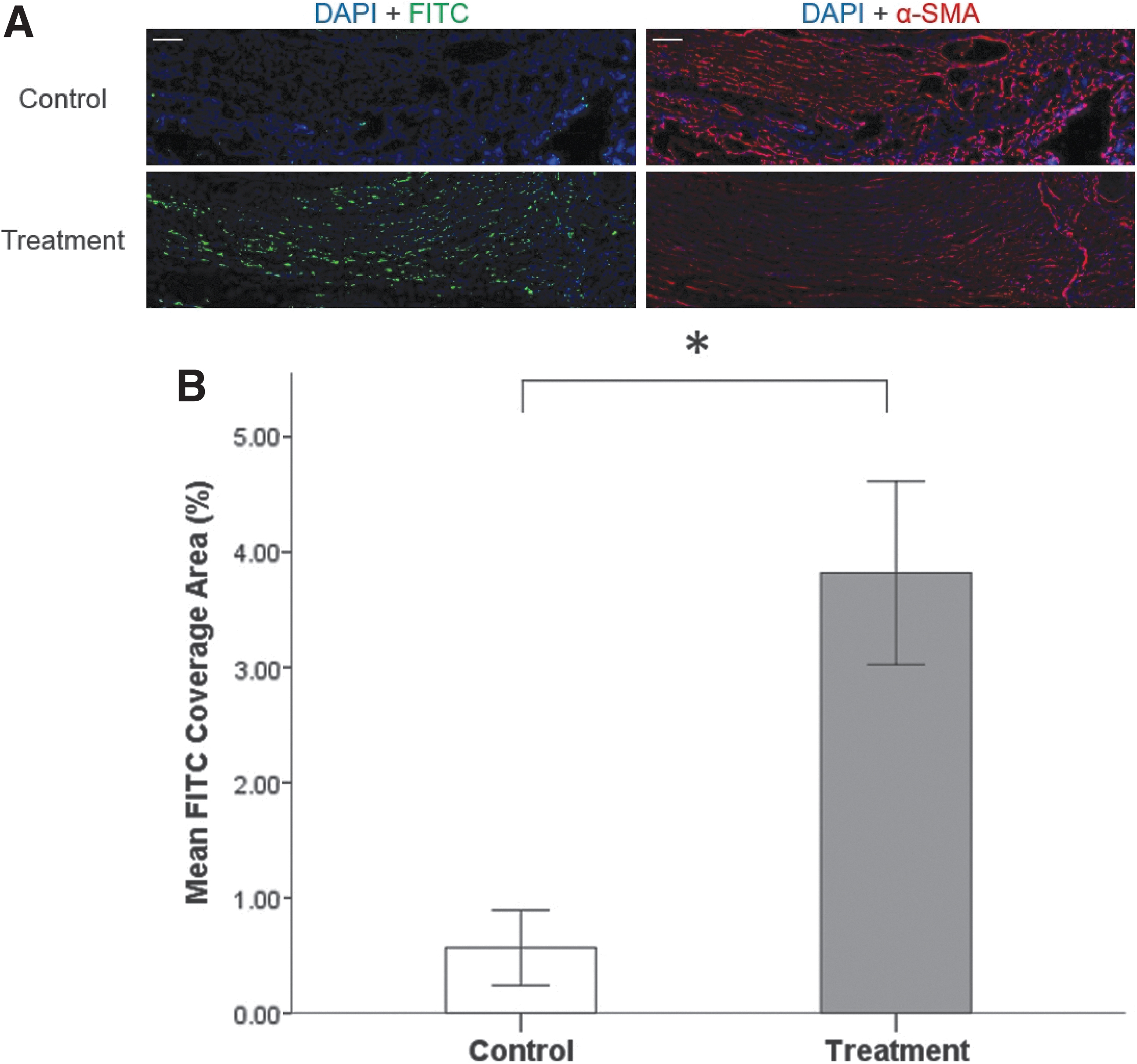
Comparison of postsurgical interstitial flow between the treatment and control groups.
In this study, systemic TGF-β1 receptor inhibitor administration significantly decreased the degree of acquired lymphedema in a mouse tail model. The TGF-β/SMAD pathway is a central mediator of both wound healing and fibrosis processes, and there are two possible explanations for why this has been proposed as being highly correlated with lymphedema. 3 First, stimulation of lymphangiogenesis was observed at the surgery site in the treatment group. As seen in Figure 3, a higher number of lymphatic vessels were observed in the treatment group. Upregulation of LYVE-1 was specifically observed where there was lower α-SMA expression, whereas there was a large area of α-SMA expression in the control group but no LYVE-1 expression. This indicates that lymphangiogenesis is achieved by suppression of α-SMA, which inhibits the formation of lymphatic vessels. Second, increased interstitial flow was observed at the surgery site in the treatment group. As seen in Figure 4, the lymphatic interstitial flow was significantly higher in the treatment group according to the amount of FITC-dextran tracer. This result may be due to the decreased fibrosis that was represented by the lower amount of α-SMA expression, which hinders lymphatic flow. In addition, Figure 2 shows that lymphatic channels were re-established at the surgery site, which helped to increase interstitial flow.
Stimulation of lymphangiogenesis can be achieved by two major ways. First, reducing the direct inhibitory effect of TGF-β1 on lymphatic epithelial cell proliferation can help regeneration of lymphatic vessels. 5 Avraham et al. reported that blockage of TGF-β1 using the TGF-β monoclonal antibody accelerated lymphangiogenesis. 3 They also suggested that inhibition of the function of TGF-β decreases the expression of Th2 cytokines (IL-4 and IL-13), which are necessary for soft tissue fibrosis. Second, downregulation of the TGF-β1 canonical pathway of fibrosis may achieve stimulation of lymphangiogenesis. Fibrosis induced by TGF-β1 causes the formation of thicker bundles of collagen matrix that have a negative effect in lymphangiogenesis. 13 Lynch et al. reported that this collagen matrix composition change at the surgery site hindered lymphatic regeneration. 12
Apart from lymphangiogenesis, interstitial lymphatic flow is another important transport mechanism of lymphatic fluid clearance. We found that a substantial amount of FITC-dextran tracer traveled through the interstitial space at the surgery site in the treatment group. However, interstitial flow was barely observed in the control group. These results suggest that fibrosis not only inhibited lymphatic vessel regeneration but also reduced the upstream interstitial flow by narrowing the interstitial space. In addition, the direction of interstitial flow is a crucial factor of lymphangiogenesis. It helps to guide the growth and organization of a developing lymphatic capillary network by enhancing lymphatic endothelial cell migration and proliferation.9,14 Thus, lack of sufficient interstitial flow level in fibrotic scar tissue reduces lymphangiogenesis and limits clearance of lymphatic flow.
Our data imply that fibrosis may mediate its proedema effects by two mechanisms: decreased lymphangiogenesis and reduced interstitial flow. However, in most previous studies, only the degree of lymphangiogenesis has been used as an assessment tool for therapeutic effect. Uzarski et al. 9 reported that lymphedema resolution could occur solely by interstitial flow regardless of VEGFR-3 signaling and lymphangiogenesis. They suggested that resolution might be more dependent upon interstitial fluid dynamics than functional lymphatic regeneration. Collectively, these findings emphasize the current limitation of data interpretation in studies using a mouse tail lymphedema model. For example, the proportion of lymphatic fluid transportation by each mechanism according to the tail model would be different from that in human lymphedema. We believe that both functional lymphatic vessel flow and interstitial flow should be taken into consideration in assessing the therapeutic effect. Our data revealed that EW-7197 treatment increased lymphatic vessel generation and interstitial flow simultaneously, and decreased fibroblast proliferation. Thus, this evidence provides support for further development of TGF-β1 inhibitor as a therapeutic agent to treat human lymphedema.
One problem with systemic TGF-β1 inhibition is that it could delay the wound healing process. 15 We observed leakage of the FITC-dextran tracer that lasted for 2 to 3 weeks after surgery in the treatment group, but not in the control group (data not shown). Considering that lymphedema usually occurs after surgery, systemic TGF-β1 inhibition could induce complications due to delayed wound healing. Further studies may be warranted to investigate a suitable application strategy, including optimal timing of delivery, safe dosage, and systemic toxicity. In addition, to avoid systemic adverse effects, local application of TGF-β1 inhibitor using drug-releasing material could be recommended for further study.
The present study showed that EW-7197 ameliorates acquired lymphedema in a mouse tail model. In immunofluorescence assessment, we found that EW-7197 induced both lymphangiogenesis and interstitial flow of the lymphatics by inhibition of the fibrosis at the surgery site. Considering its therapeutic effect, EW-7197 may have potential in treating lymphedema.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant (2017-478) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2019R1A2C1009055).