
Abstract
Background:
Radiation therapy has been applied to prolong the duration of lymphedema. This study aimed to evaluate the effect of radiation on the development of lymphedema in a mouse hindlimb model.
Methods and Results:
A total of 24 Balb/c mice underwent the right popliteal lymph node excision and the afferent and efferent lymphatics blockage. The radiation group (n = 12) received a single 20 Gy radiation 1 day before surgery in the right hindlimb of each mouse, whereas the control group (n = 12) only received surgery without radiation. The right hindpaw thickness of each mouse was measured twice a week for 4 weeks. Fluorescence microscopy images using fluorescein isothiocyanate–dextran tracer were obtained once weekly. Immunohistochemical (IHC) staining images using anti-lymphatic vessel endothelial hyaluronan receptor-1 (anti-LYVE-1) were obtained at 4 weeks after surgery. The radiation group showed significant increase in the thickness of the right hind paws from 0.5 to 2 weeks compared with the control group. As for fluorescence lymphography, the radiation group showed a lower number of regenerated lymphatics and more congestion of tracers in the operated limb at the surgery sites at 1, 2, 3, and 4 weeks after surgery. For the IHC analysis, the radiation group showed a lower number of regenerated lymphatics per high-power field at the surgery site than the control group.
Conclusion:
Radiation therapy transiently aggravated the extent of lymphedema by inhibiting regenerated lymphatics in a mouse hindlimb model. However, it did not prolong the duration of lymphedema because the cutaneous interstitial flow contributes to the lymphatic fluid clearance.
Introduction
Lymphedema is a pathophysiologic process characterized by the accumulation of protein-rich fluid in the interstitial space, adipose deposition, and tissue fibrosis resulting from injury, infection, obstruction, or congenital defects in the lymphatic system. Globally, the most common cause of lymphedema is filariasis that occurs owing to infection by the nematode Wuchereria bancrofti. 1 In the developed world, majority of lymphedema cases are secondary and caused by malignancy or its treatment.2–6 Lymphedema is a chronic condition that can be managed; however, it is generally not cured. 7 As the treatment of chronic lymphedema remains challenging, the preclinical studies of the underlying pathophysiology and therapeutic interventions of lymphedema are urgently warranted. A reliable and reproducible lymphedema animal model is quite essential for such studies. The mouse tail model, by blocking lymphatic collateral vessels located at both sides of a rodent tail, was used to clarify the underlying mechanisms of lymphedema development in most recent studies.8–10 Tail model has the advantages of low cost, easy handling, and its effectiveness in interpreting the molecular mechanisms of lymphedema; however, as the pattern of lymphatic flow and regeneration in rodent tail is different from that of humans, there is a necessity of an animal model that mimics the secondary lymphedema of humans.
A number of hindlimb models in rodents,11–16 which are more complex to create but physiologically and anatomically more similar to human postsurgical lymphedema, have been reported with various techniques. Most of previous studies using a hindlimb model reported gain of secondary lymphedema in the affected limb within 1 week after model creation surgery. However, the improvement of lymphedema usually occurred within 2–3 weeks because of wound healing, accompanied by lymphatic channel regeneration. To prolong the duration of secondary lymphedema, radiation therapy was applied before or after surgery.13,14 Theoretically, radiation therapy is expected to damage the healing competence of tissue and thus augment the duration and degree of secondary lymphedema. However, no comparative study has been conducted to investigate whether radiation therapy truly affects the results of the experimental secondary hindlimb lymphedema.
In this study, we hypothesized that conducting a surgery to create lymphedema preceded by radiation therapy may augment secondary lymphedema by inhibiting lymphangiogenesis and hindering lymphatic channel regeneration compared with conducting a surgery without radiation therapy. Thus, the purpose of this study was to evaluate the effect of radiation therapy on the duration and degree of secondary lymphedema in an experimental hindlimb lymphedema model.
Materials and Methods
This study was approved by the committee for animal research at our institution and conformed to the U.S. National Institutes of Health Guidelines on the care and use of laboratory animals.
A lymphedema mouse hindlimb model
Hindlimb lymphedema was created in 10-week-old female Balb/c mice (Orient Bio, Seong-nam, Korea) as described previously, 14 but with a modification. We did not inject an indicative blue dye to avoid its toxic effect. In brief, the mice were anesthetized with intramuscular injection of 50 mg/kg zolazepam and tiletamine (Zoletil 50; Virbac, Carros, France) and 10 mg/kg xylazine (Rompun; Bayer HealthCare, Leverkusen, Germany). The right-side inguinal skin was circumferentially incised, followed by location of the popliteal lymph node (Fig. 1a) and complete resection with the surrounding adipose tissue. A hole at the facial layer was noted after the lymph node resection (Fig. 1b). We cauterized the inner wall of the hole using a Bovie cautery to block both afferent and efferent lymphatics. Finally, both the ends of the skin wound were directly sutured with 5-0 nylon sutures. This surgical procedure took ∼30 minutes by a single operator.

Mouse limb irradiation
The irradiation was performed a day before surgery for the radiation group. The mice (n = 12) were anesthetized with zolazepam–tiletamine, and then the right inguinal areas were exposed and irradiated with 20 Gy in a single dose. The ionizing radiation was emitted from the X-RAD 320 machine (Precision X-Rad, North Branford, CT) at a dose rate of 4.12 Gy/min (150 kVp, 20 mA). The rest of the mouse body was shielded from radiation by using lead blocks. The control group (n = 12) mice received anesthetic and were placed in the irradiator, but they received no radiation. All mice were maintained in a temperature-controlled room (22 ± 2°C) and supplied with food and water ad libitum. After the respective observation periods, the mice were killed by carbon dioxide asphyxiation.
Hindpaw thickness measurements
Digital images of mouse hind paws were collected twice a week. Canon D550 camera was mounted on a tripod for imaging mouse paws. Hindpaw thickness was measured in standardized locations (2 mm proximal to the tarsal joint) 17 from these digital images using ImageJ imaging software (U.S. National Institutes of Health, Bethesda, MD).
Fluorescence lymphography
Fluorescence lymphography, which was performed once weekly after surgery for 4 weeks, was used to evaluate the distribution of regenerated lymphatic vasculature and lymphatic flow in the surrounding tissue. Lysine-fixable fluorescein isothiocyanate–dextran of 2000 kDa (Molecular Probes) was used as a tracer. Tracer (5 μL) was injected intradermally into the right hind palms for in vivo lymphatic imaging, with a gentle massage of the footpad for better distribution. Digital images were taken immediately with a microscope-based multispectral imaging system for examination of the uptake of fluorescence and lymphatic pattern. In brief, a Nuance™ spectral imaging system (PerkinElmer, Inc., Hopkinton, MA) was mounted onto a conventional fluorescence microscope equipped with a filter cube comprising a standard excitation filter and dichroic mirror and a long-pass emission filter.
Immunohistochemical staining
After 4 weeks of surgery, all mice were killed using carbon dioxide asphyxiation, and then the right hindlimb of each mouse was cut off from the body. We collected the sample including the surgical area for immunohistochemical (IHC) staining. The surgical area and the range of sample collection are given in Figure 4a. The tissue was immersed in paraformaldehyde perfusion fixative (Electron Microscopy Sciences, Hatfield, PA) overnight at 4°C. After decalcification, the samples were embedded in paraffin and sectioned into 5 μm slices. After deparaffinization, rehydration, and blocking, the anti-lymphatic vessel endothelial hyaluronan receptor-1 (anti-LYVE-1) polyclonal antibody (Abcam, Cambridge, United Kingdom) was used for IHC staining of lymphatic vessels at a dilution of 1:100.
The IHC images taken from the tissue of 5 mm distal to the surgery site were analyzed by two experienced observers, independently. Five random areas were selected with the same scale per high-power field (HPF) at 200 × magnification. The number of lymphatic vessels stained by anti-LYVE-1 in each area was counted, and the mean value of the number of lymphatic vessels from the five areas was calculated.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (SPSS, Inc., Chicago, IL). The comparison of hindpaw thickness between the two groups was performed using the Student's t-test. The mean number of vessels per HPF was compared using the Student's t-test. All p-values were two-sided with statistical significance evaluated at the 0.05 alpha level, and 95% confidence intervals were constructed to assess the precision of the obtained estimates.
Results
Hindpaw thickness measurements
During the observation period, all mice developed an acute lymphedema immediately after surgery. In the radiation group, only one mouse developed hindlimb necrosis. The data of this mouse were excluded from this study.
The thickness of the hind paws in the control and radiation groups rapidly increased and reached the peak value at 0.5 weeks after surgery. The values in both groups gradually reduced from 0.5 weeks after the surgery. The differences of the hindpaw thickness between the radiation and control groups were statistically significant from 0.5 to 2 weeks (5.0 ± 0.2 mm vs. 4.7 ± 0.1 mm, p = 0.026 at 0.5 weeks; 4.8 ± 0.2 mm vs. 4.4 ± 0.1 mm, p = 0.012 at 1 week; 4.6 ± 0.2 mm vs. 4.2 ± 0.1 mm, p = 0.032 at 1.5 weeks; 4.4 ± 0.2 mm vs. 4.1 ± 0.1 mm, p = 0.046 at 2 weeks) (Fig. 2).
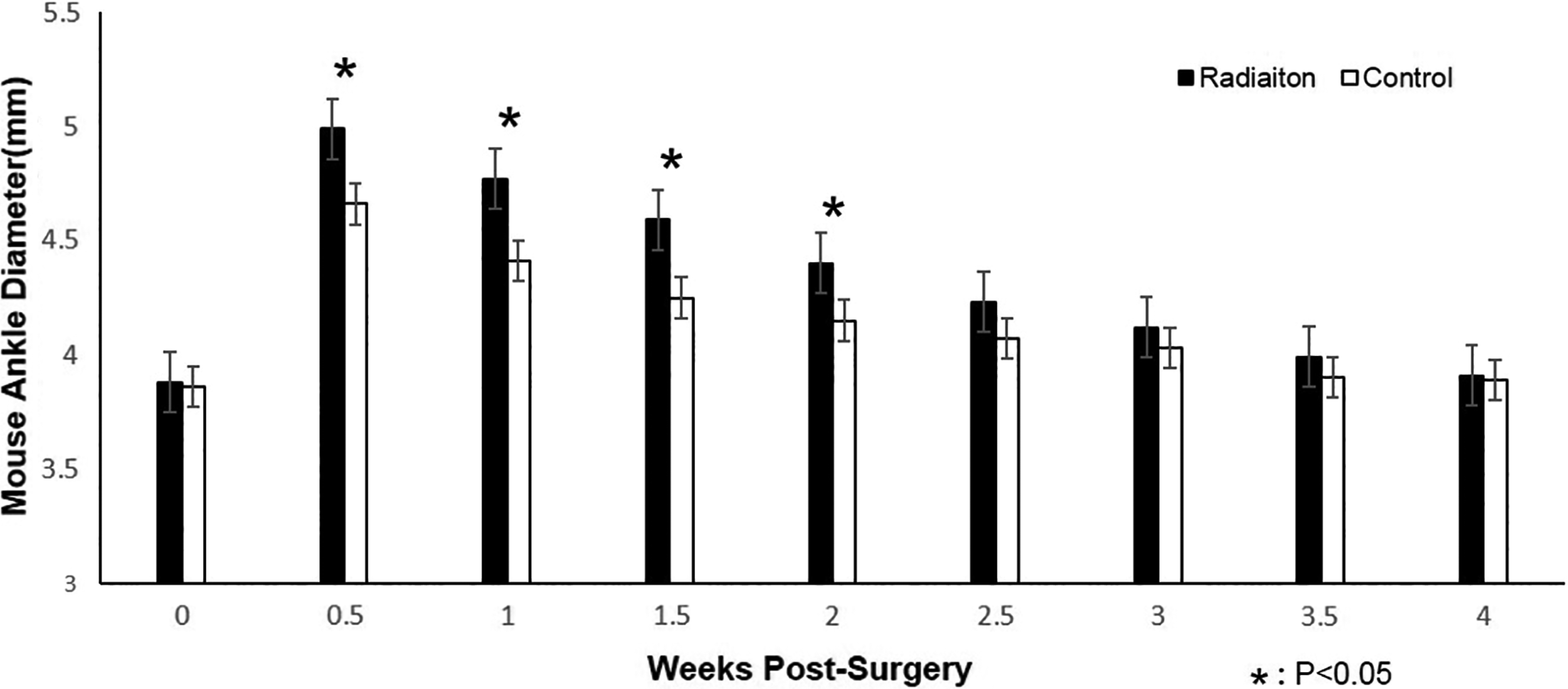
Changes in the mice hindpaw thickness after surgery. The radiation group showed a significant augment compared with the control group during 2 weeks after surgery.
Fluorescence lymphography
The radiation group showed a lower number of regenerated lymphatics in the operated limb and more congestion of tracers distal to the surgery site at 1, 2, 3, and 4 weeks after surgery. The image in the radiation group obtained at 3 weeks showed that inguinal lymph node occurred because of the lack of regenerated lymphatics (Fig. 3).
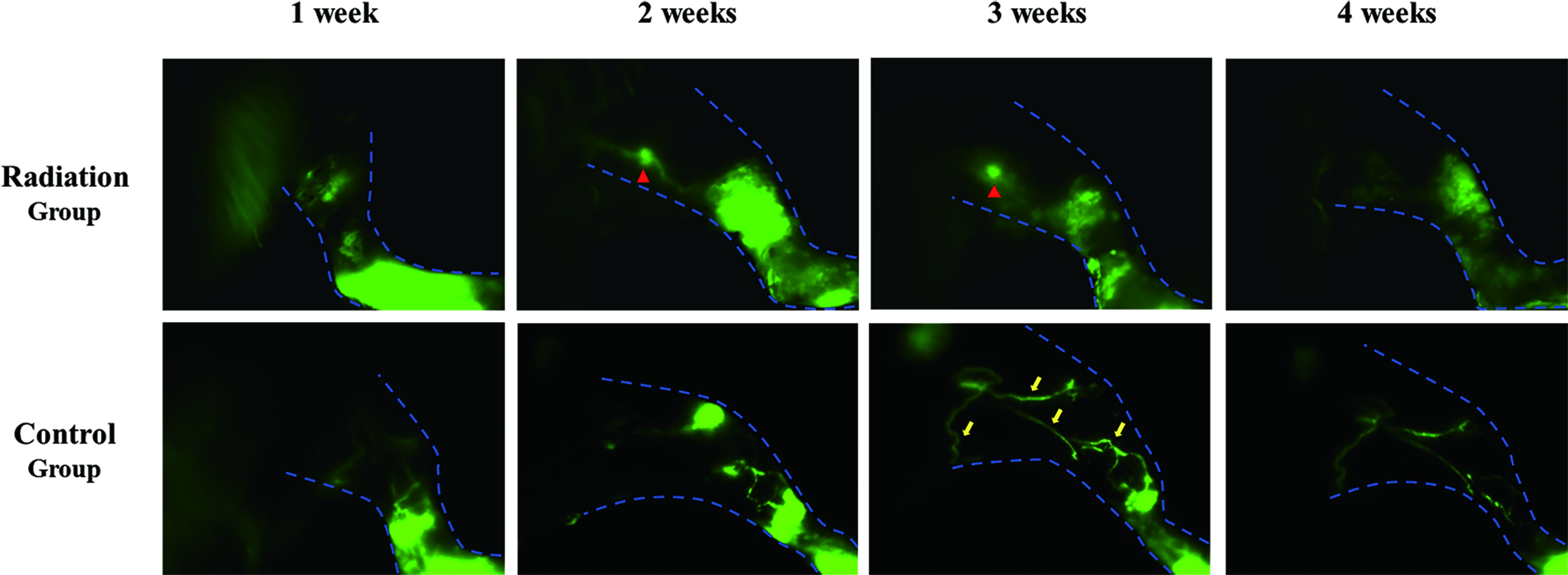
The fluorescence lymphography shows less regenerated lymphatics and more congestion of tracers in the radiation group at 1, 2, 3, and 4 weeks after surgery. Arrow heads indicate inguinal lymph node; arrows indicate the regenerated lymphatic vessels. Color images are available online.
IHC staining
The radiation group showed a lower number of regenerated lymphatics per HPF at the surgery site than the control group (3.6 ± 2.4 vs. 6.1 ± 2.4; p < 0.01) (Fig. 4).

IHC analysis of dermal lymphatics in the radiation and control groups.
Discussion
In this study, we showed that secondary lymphedema was augmented in the radiation group. We found that the number of regenerated lymphatic channels were lower in the radiation group. This finding is supported by histological analysis that demonstrated a lower number of LYVE-1-stained lymphatic vessels in the radiation group. In our study, an improved method was used to create a lymphedema hindlimb model. We blocked the lymphatic components without injecting blue dues. For the previous hindlimb models,11,14,15 researchers used various blue dye to identify the lymph nodes and lymphatics. The toxicity of blue dyes caused an inflammatory response, which led to tissue edema. It was not possible to distinguish the tissue edema results from the lymph node excision or toxicity of blue dyes in their studies.
Previous studies have demonstrated the incapability of surgery to create a sustained lymphedema model because the lymphatic endothelial cells' (LECs) proliferation and organization result in spontaneous lymphatic reconnection. Roh et al. 11 devised a mouse hindlimb lymphedema model by excising a popliteal lymph, a subiliac lymph node, a sciatic lymph node, and cauterization of the femoral lymphatic vessels without radiation. In this lymphedema model, a significant difference in the degree of lymphedema between the surgery and control groups was maintained only for 18 days after the surgery. Radiation therapy has been used as an adjunctive method in the creation of tail and hindlimb lymphedema model. Previous study 18 demonstrated the effects of radiation therapy on the lymphatic vessels in a tail model. Researchers found that radiation therapy decreases the number of dermal capillary lymphatic vessels and LECs and that a single 15 Gy dosage is sufficient to cause the loss of lymphatic vessels. Our fluorescence lymphography and histological finding are consistent with their finding. Lymphangiogenesis was hindered in the radiation group compared with that in the control group, which may contribute to the higher lymphedema degree in the radiation group.
However, we found that the duration of secondary lymphedema was not significantly different between the two groups. Apart from lymphatic vessel drainage, interstitial flow (IF) has been indicated, another important route for lymphatic fluid clearance.19,20 From the fluorescence image in the radiation group obtained at 3 weeks, we can see that the inguinal lymph node was shown because of the lack of regenerated lymphatics. This finding suggests the tracer mainly passed through the surgical site by interstitial flow rather than regenerated lymphatics, which may result in nonsignificant difference of the lymphedema duration between the two groups. Uzarski et al. 21 also indicated that the resolution of lymphedema may become more dependent on IF than on lymphangiogenesis in a mouse tail model.
Lymphangiogenesis has only been considered as a clearance route by most studies using hindlimb models. However, our finding implicates that IF plays an important role in lymphatic fluid clearance. Modified suture technique, such as suturing the skin edges to the underlying muscle or electrocauterizing both edges of the wound, may be valuable for blocking IF. For instance, Oashi et al. 14 developed a lymphedema mouse hindlimb model. The duration of lymphedema can last several months. To block the dermal backflow, they sutured the skin edges to the underlying muscle with 6-0 nylon sutures leaving a gap of 1–2 mm between skin edges. Similarly, Iwasaki et al. 22 developed a new hindlimb model by removing both the inguinal and popliteal lymph nodes, followed by silicone splint suture in the inguinal region. The lymphedema degree and duration were significantly increased by their revised surgical method. However, in our study, the ends of the skin wound were directly sutured with 5-0 nylon sutures, which means the dermal backflow reconstructed more quickly by the acceleration of wound healing. Therefore, the lymphedema duration can only last <3 weeks. Further studies on the hindlimb lymphedema model should consider both the factors of lymphangiogenesis and interstitial flow.
There are some limitations to this study. First, we did not evaluate the effect of tissue fibrosis on lymphedema. Radiation therapy is known to cause transforming growth factor-beta 1-mediated tissue fibrosis,23–25 which is another potential mechanism to induce lymphatic stasis. Second, a single 20 Gy radiation was only administered to each mouse, yielding the results of this study. We selected 20 Gy as the dose of radiation because it was widely used in previous studies. However, we cannot exclude the possibility that the results would be affected by different dose. Considered together, the effect of various dosage radiation on the lymphatic stasis and the mechanism associated with the fibrosis are required to be investigated in the future.
Conclusions
This study showed that radiation transiently aggravated the lymphedema degree by inhibiting regenerated lymphatics in a mouse hindlimb model. However, it did not prolong the duration of lymphedema because the cutaneous interstitial flow contributes to lymphatic fluid clearance. A sustained hindlimb lymphedema model may be developed by using the combination of lymphatic components incision, radiation, and the method to block the interstitial flow.
Footnotes
Acknowledgment
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2019R1A2C1009055) and a grant (2017-478) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
Author Disclosure Statement
The authors have declared no conflict of interests.