
Abstract
Background:
This study aimed at testing whether arm-to-leg ratios of extracellular water (ECW) and ECW normalized to intracellular water (ICW), measured by bioimpedance spectroscopy (BIS), can accurately detect bilateral, lower-limb lymphedema, and whether accounting for sex, age, and body mass index (BMI) improves the diagnostic performance of cut-offs.
Methods and Results:
We conducted a dual-approach, case–control study consisting of cases of bilateral, lower-limb lymphedema and healthy controls who self-reported absence of lymphedema. The diagnostic performance using normative data-derived cut-offs (i.e., mean + 0.5 standard deviation [SD] to mean + 3 SD; n = 136, 66% controls) and receiver operating characteristic (ROC) curve-derived cut-offs (n = 746, 94% controls) was assessed. The impact of sex, age, and BMI was investigated by comparing stratified and nonstratified normative data-derived cut-offs, and ROC curves generated from adjusted and unadjusted logistic regression models. Arm-to-leg ratios of ECW between mean + 0.5 SD and mean + 1 SD showed fair to good sensitivity (0.73–0.84) and poor to good specificity (0.64 to 0.84). Arm-to-leg ratios of ECW/ICW failed to detect lymphedema (sensitivity <0.5). Stratification by sex, or by sex and age, yielded similar results to nonstratified cut-offs. Cut-offs derived from adjusted ROC curves showed both good sensitivity (0.83–0.89) and specificity (0.8–0.84).
Conclusion:
These findings represent new BIS criteria for diagnosing lower-limb lymphedema that do not rely on comparison to baseline measures or the presence of a nonaffected, contralateral limb.
Introduction
Lymphedema is a condition of impaired lymph drainage, which initially presents as swelling, tightness, heaviness, or throbbing in the affected areas.1,2 Progressive changes can lead to deposition of adipose tissue and fibrosis, resulting in gross disfiguration and loss of function. 2 Lymphedema is estimated to affect up to 250 million people worldwide, with 90% of cases reported to affect the lower limbs. 3 Approximately 1% of all cases are described as “primary lymphedema” and are idiopathic or heritable, whereas 99% of cases are described as “secondary lymphedema” and develop from acquired damage to or dysfunction of the lymphatic system. The most common causes of secondary lymphedema are parasitic infection (developing countries), cancer treatment, and obesity (developed countries). 3
Accumulating evidence from research involving women with unilateral, upper-limb lymphedema after treatment for breast cancer suggests that early detection and intervention can reduce the risk of subclinical lymphedema progressing to a chronic advanced stage, which becomes particularly difficult and expensive to treat.4–9 Currently in the clinic, lower-limb lymphedema is usually diagnosed after clinical examination following a complaint of swollen or heavy-feeling legs. In cases of unilateral lymphedema, the affected leg can be compared with the unaffected leg (e.g., using bioimpedance spectroscopy [BIS] or circumferences) to determine whether the leg is swollen. However, bilateral lymphedema is more complicated to diagnose due to the lack of availability of a comparable limb.
BIS, which measures impedance of extracellular and intracellular water (ICW) to an alternating electrical current passed through the body at a range of nondiscernible frequencies, has previously been shown to be a noninvasive, portable technology that is capable of detecting subclinical lymphedema. 9 Subclinical lymphedema is considered present when the ratio of extracellular water (ECW) between arms or between legs is outside three standard deviations (SDs) of the normative mean.10,11 However, due to the unavailability of an unaffected contralateral limb for comparison, there is a notable lack of effective criteria for detecting bilateral lymphedema in the upper or lower limbs.
Cornish et al. 12 proposed that since lymphedema is an accumulation of lymph in ECW with ICW being unchanged, the ratio of ECW/ICW within the same limb could be used as an index of the presence of lymphedema and provided preliminary supporting evidence from a small number of subjects with unilateral breast cancer-related lymphedema. In a later study, 13 the method was extended to quantification of bilateral lymphedema, although it was noted that ECW/ICW ratios varied with age, sex, and limb dominance. Recently, Steele et al. 14 published the first normative values for arm-to-leg ratios of ECW (dominant side = 1.129 ± 0.160, nondominant side = 1.165 ± 0.174) and ECW/ICW (dominant side = 1.194 ± 0.453, nondominant side = 1.117 ± 0.367) based on 808 self-reported healthy individuals with no history of lymphedema.
Updated values for inter-arm (ECW = 0.987 ± 0.067, ECW/ICW = 0.957 ± 0.188) and inter-leg (ECW = 1.005 ± 0.072, ECW/ICW = 1.024 ± 0.183) ratios, with and without stratification by sex, age, and body mass index (BMI) were also reported. Key findings were that arm-to-leg ratios (but not inter-arm or inter-leg ratios) were significantly affected by sex and age in accord with the observations of Ward et al., 10 and to a lesser extent by BMI, and that normalizing ECW to ICW led to larger within- and between-subject variation. 14 Based on these results, we predicted that arm-to-leg ratios of ECW and ECW/ICW, possibly stratified by sex and age, could be used to develop effective criteria for identifying bilateral lymphedema.
Therefore, the first aim of this case
Methods
Participants
We conducted a dual-approach, case

Flowchart showing the flow of participant data through the study. BIS, bioimpedance spectroscopy; BMI, body mass index; ROC, receiver operating characteristic.
Briefly, a sample (n = 898) of self-reported healthy males and females with no history of lymphedema, removal or irradiation of lymph nodes, or cancer were recruited from five centers across Australia and New Zealand. Our first approach involved randomizing controls 9:1 into a “training” set (n = 808), which was previously used for calculating normative means and SDs, 14 and a “test” set (n = 90), which was retained for use in testing the prediction of normative data-derived cut-offs in this study in an independent set of observations. A 9:1 split was chosen to maximize the number of controls used for generating normative data-derived cut-offs and to allow stratification of cut-offs by sex, age, and BMI. Further, a test set of 90 controls was considered sufficient, given that we only had access to 46 cases of bilateral lower-limb lymphedema.
Our second approach involved using all controls with complete data (n = 700; data for 198 participants were excluded due to missing sex, age, BMI, or specific BIS measurements; see Fig. 1) and all cases (n = 46). Appropriate ethical approvals were obtained from the relevant institutions for the conduct of all initial studies, as well as this study (ACTRN1500001072), and all participants provided written informed consent.
Procedures
All contributing studies implemented the same validated protocol as previously published 14 and as outlined by Impedimed 15 to measure impedance of total body water (TBW) (Rinf), ICW (Ri), and ECW (R0) in arms and legs by using either a portable, Impedimed SFB7, SFB3, or U400 BIS device. BIS measurements were taken with the participant lying supine with legs apart.
For any given measure, two measurement electrodes were placed at either end of the arm or leg (i.e., wrist for arm measures and ankle for leg measures) with a current drive electrode placed at the base of the middle finger or toe, respectively, and another placed on the ipsilateral or contralateral foot or hand, respectively. 16 Each limb segment was measured in this manner, and the resistances corresponding to ECW (R0) and to TBW (Rinf) were determined. ICW resistance (Ri) was subsequently calculated with the manufacturer's software (Bioimp 4.15.0.0; ImpediMed Ltd., Brisbane), which uses the formula: Ri = (R0 × Rinf)/(R0 − Rinf). Sex, age, height, weight, and self-reported dominant hand were recorded for each participant.
Data analysis
Characteristics of cases and controls were summarized and compared by using unpaired t-tests and chi-squared tests. The following inter-limb ratios were calculated for each participant: dominant arm/nondominant arm (R0 and Ri:R0); dominant leg/nondominant leg (R0 and Ri:R0); dominant arm/dominant leg (R0 and Ri:R0); and nondominant arm/nondominant leg (R0 and Ri:R0). Inter-limb ratios of cases were compared with controls by using boxplots and Wilcoxon signed-rank tests.
Normative data-derived cut-offs
Binary cut-offs ranging from mean + 0.5 to 3 SD were calculated based on the stratified (sex, and sex and age) and nonstratified means and SDs of the normative inter-limb ratios previously published. 14 All cut-offs were evaluated for their ability to distinguish cases of bilateral lower-limb lymphedema (n = 46) from controls in the test dataset (n = 90) by calculating and comparing sensitivity and specificity (total n = 136).
ROC curve-derived cut-offs
All participants with complete demographic (sex, age, and BMI) and bioimpedance data, that is controls from training and test datasets (n = 700) plus cases (n = 46), were used for generating ROC curve-derived cut-offs (total n = 746). Univariable (dependent variable = lymphedema status; independent variable = inter-limb R0 or Ri:R0 ratio) and multivariable (dependent variable = lymphedema status; independent variables = inter-limb R0 or Ri:R0 ratio, sex, age, and BMI) logistic regression models were fit to establish factors associated with lymphedema status and produce probabilities for generating ROC curves.
McFadden's pseudo R2 values were calculated to assess model fit. Pseudo R2 values for logistic regression models are typically lower than traditional R2 values for linear regression models. According to McFadden, 17 pseudo R2 values between 0.2 and 0.4 represent an excellent fit. All covariates were retained in the multivariable logistic regression models (independent of their association with lymphedema status) based on evidence that sex, age, and BMI significantly affect arm-to-leg ratios. 14
ROC curves were created by using raw impedance ratios (equivalent to the unadjusted logistic regression models) and probabilities generated from the multivariable logistic regression models. ROC curves were compared by using the bootstrap test for two correlated ROC curves, and the area under the ROC curve (AUC) was calculated as a measure of diagnostic performance for all predictors (AUC of 0.5–0.6 = fail, 0.6–0.7 = poor, 0.7–0.8 = fair, 0.8–0.9 = good, 0.9–1 = excellent).
Optimal cut-offs were selected by using clinical reasoning, where we considered sensitivity to be more important than specificity in the context of diagnosing lymphedema. A priori we considered sensitivity above 80% and specificity above 70% as being indicative of a clinically useful diagnostic threshold for lymphedema. All analyses were conducted in R version 3.3.1. The R packages, pROC and epiR, were used to construct ROC curves and calculate measures of diagnostic performance. 18
Results
Characteristics of participants
Data from a total of 944 participants (controls = 898, cases = 46) were assessed in this study. The characteristics of all participants are presented in Table 1. There was a greater proportion of females among cases compared with controls (89% vs. 65%, p = 0.002); cases were significantly older (64 ± 13 vs. 48 ± 15 years; p < 0.001) and had higher BMI (34 ± 8 vs. 26 ± 4 kg/m2; p < 0.001). Comparable differences in demographic variables between cases and controls were observed when assessed in each of these subsets (i.e., between the cases and controls used in the normal distribution approach and the ROC curve approach).
Characteristics of Participants
Two-sample t-tests (continuous variables) and chi-squared tests (categorical variables) were used to compare characteristics of cases and controls.
BMI, body mass index; SD, standard deviation.
Comparison of inter-limb ratios between cases and controls
Inter-limb ratios of cases (n = 46) versus controls with complete data (n = 700) are presented in Figure 2. Arm-to-leg ratios of R0 were larger for cases compared with controls, with a mean difference of 0.318 (p < 0.01) on the dominant side of the body and 0.336 (p < 0.01) on the nondominant side. Arm-to-leg ratios of Ri:R0 also showed differences between cases and controls, with mean differences of 0.470 (p < 0.01) and 0.548 (p < 0.01) on the dominant and nondominant sides, respectively. For completeness, inter-arm and inter-leg ratios were also compared (data not shown). Inter-arm ratios of R0, inter-leg ratios of R0, and inter-arm ratios of Ri:R0 did not differ between cases and controls; whereas inter-leg ratios of Ri:R0 differed by 0.158 (p < 0.01).
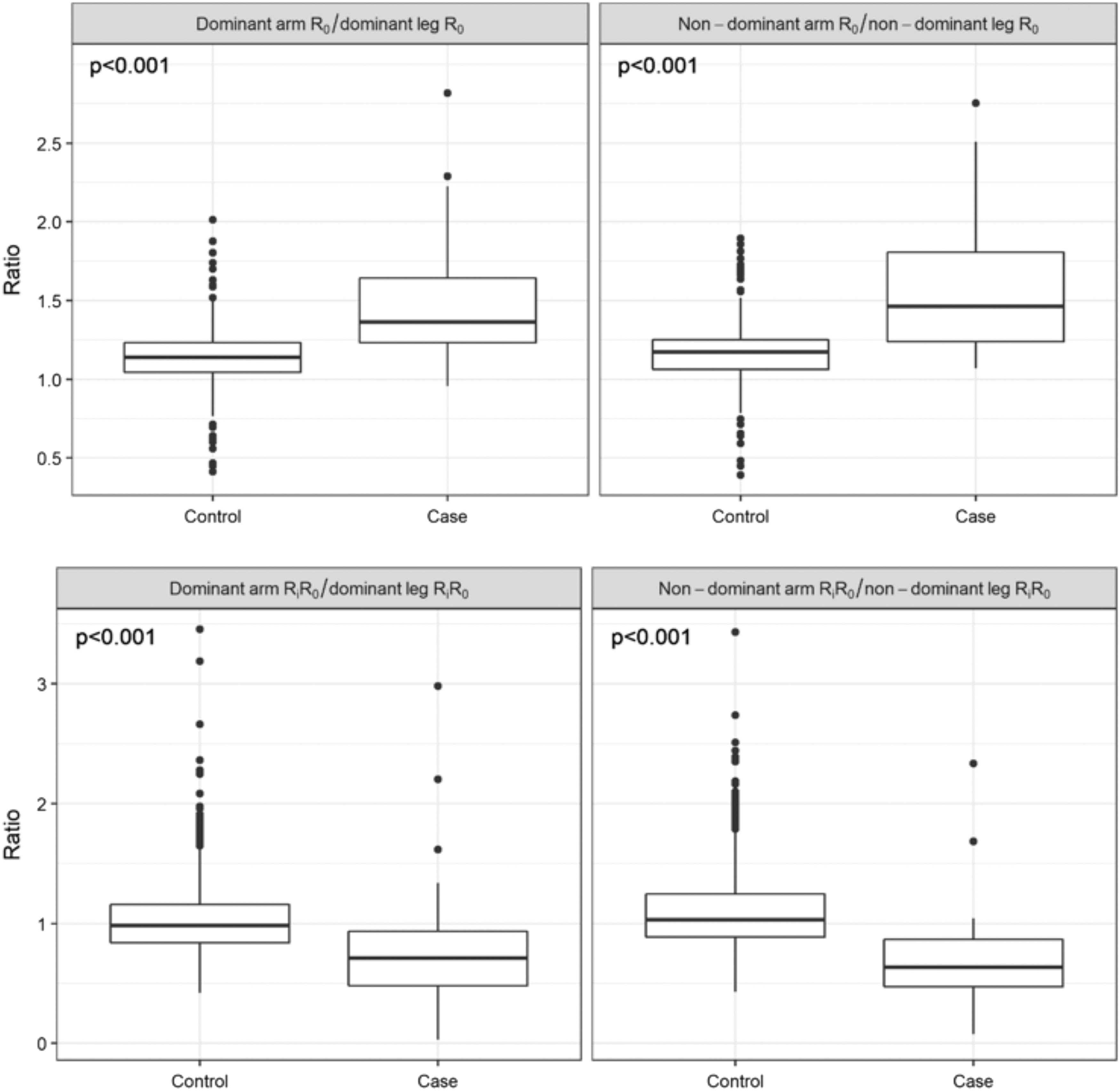
Interlimb ratios of R0 and Ri:R0 of controls compared with lymphedema cases. The Wilcoxon signed-rank test was used to test whether inter-limb ratios of lymphedema cases were statistically different from controls (p < 0.05).
Normative data-derived cut-offs
Sensitivity and specificity were calculated to describe the ability of cut-offs derived from normative inter-leg R0 ratios, arm-to-leg R0 ratios, and arm-to-leg Ri:R0 ratios (see Supplementary Table S1 for sensitivity and specificity findings). Both the inter-leg R0 ratios and the arm-to-leg Ri:R0 ratios performed poorly with very low sensitivity (<0.5) for all cut-offs. Arm-to-leg ratios of R0 performed relatively well at cut-offs between mean + 0.5 SD and mean + 1 SD, with sensitivity ranging from 0.73 to 0.84 and specificity ranging from 0.64 to 0.84.
Cut-offs stratified by demographic factors (i.e., sex, and sex and age) also performed relatively well, with sensitivity ranging from 0.65 to 0.80 and from 0.65 to 0.75, between mean + 0.5 and mean + 1 SD for sex-stratified, and sex- and age-stratified cut-offs, respectively. Specificity ranged from 0.61 to 0.81 and from 0.66 to 0.80, between mean + 0.5 and mean + 1 SD for sex-stratified, and sex- and age-stratified cut-offs, respectively. Therefore, stratification by sex, or by sex and age, did not appear to improve diagnostic performance of normative data-derived cut-offs.
ROC curve-derived cut-offs
Table 2 presents model coefficients for the four adjusted logistic regression models (dependent variable = lymphedema status, independent variables = inter-limb ratios, sex, age, and BMI), alongside McFadden's pseudo R2 values for the adjusted and unadjusted models. With the exception of one (unadjusted model for dominant Ri:R0 ratio), all pseudo R2 values were above 0.2, indicating excellent fit. However, all pseudo R2 values for the adjusted models were approximately twice that of the unadjusted models, indicating superiority of the adjusted models (Table 2).
Model Coefficients and Fit
McFadden's pseudo R2 values between 0.2 and 0.4 represent an excellent fit.
Unadjusted and adjusted ROC curves are presented in Figure 3, and the diagnostic performance of predictors is summarized in Table 3. All AUC values were significantly larger than 0.5 (p < 0.001), and the adjusted models performed significantly better than unadjusted ratios at classifying cases of lymphedema (p < 0.001). There were no significant differences between comparable ROC curves for R0 and Ri:R0 (p > 0.05). Cut-offs with maximal sensitivity and adequate specificity were derived from ROC curves and are presented in Table 4.
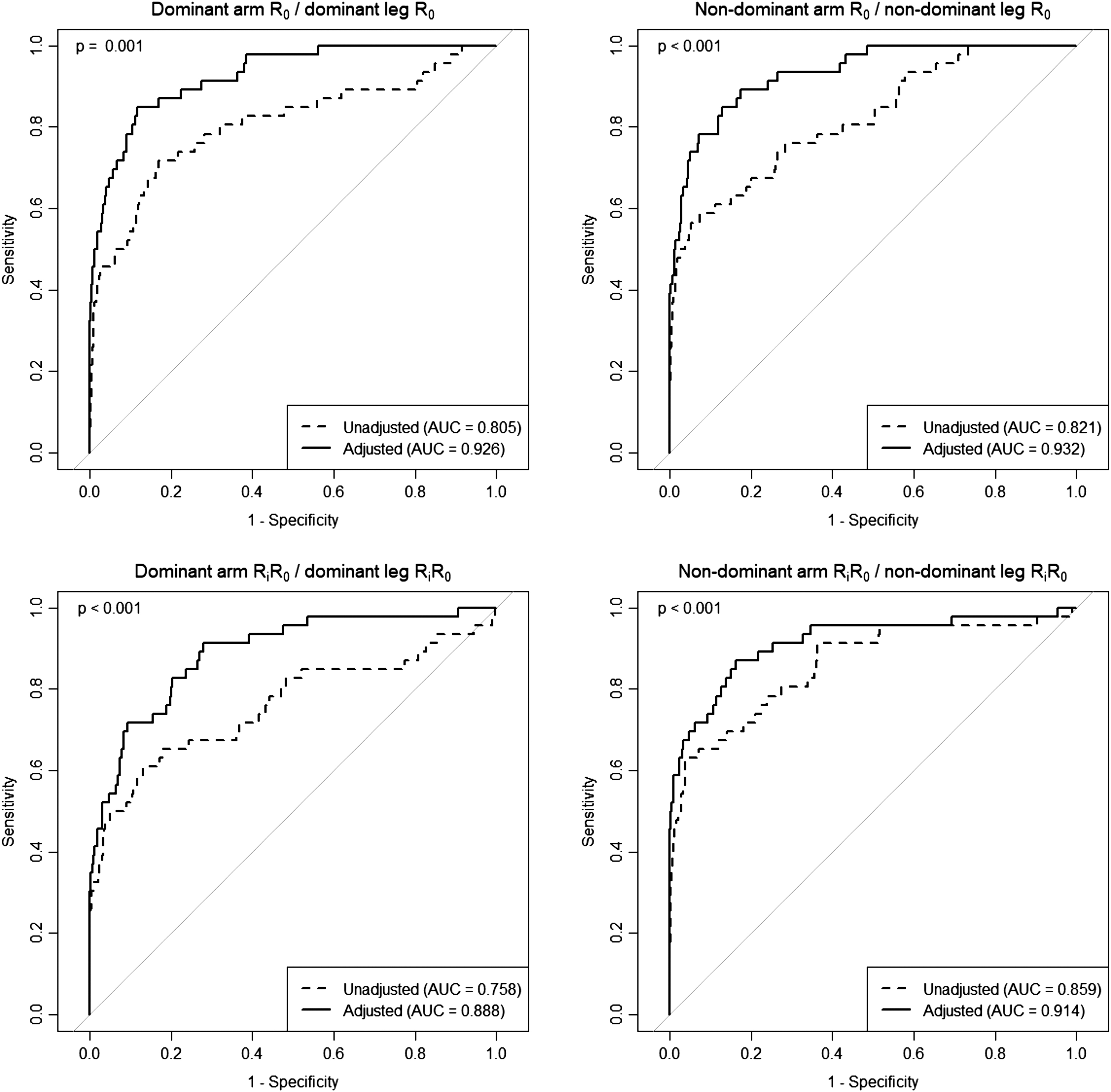
ROC curves for inter-limb ratios of R0 and Ri:R0. Unadjusted and adjusted ROC curves were compared by using the bootstrap test for two correlated ROC curves. AUC, area under the ROC curve.
Diagnostic Performance of Unadjusted and Adjusted Inter-Limb Ratios of R0 and Ri:R0
A p-value <0.05 indicates that the true AUC is not equal to 0.5.
AUC, area under the receiver operating characteristic curve; CI, confidence interval; SE, standard error.
Sensitivity and Specificity of Receiver Operating Characteristic Curve-Derived Cut-offs
Cut-offs derived from unadjusted ROC curves showed fair to good sensitivity (0.72–0.80) and poor to fair specificity (0.63–0.73), similar to that of the normative data-derived cut-offs. Cut-offs derived from adjusted ROC curves showed both good sensitivity (0.83–0.89) and specificity (0.8–0.84).
Discussion
Detection of bilateral lymphedema is complicated by the unavailability of an unaffected comparable limb. This study investigated whether arm-to-leg ratios of ECW or ECW/ICW can be used to detect lymphedema in individuals at risk of bilateral lymphedema. Ratios differed significantly between individuals with and without bilateral lower-limb lymphedema, providing support for the use of arm-to-leg ratios. Diagnostic cut-off values were derived by using two different approaches.
The first approach used binary cut-offs derived from normative data using the normal (Gaussian) distribution method. This involved calculation of nonstratified, sex-stratified, and sex- and age-stratified cut-offs ranging from the normative mean + 0.5 SD up to +3 SD. Arm-to-leg ratios of R0 performed relatively well at cut-offs between mean + 0.5 SD and mean + 1 SD, which equates to cut-off values of 1.209 to 1.289 on the dominant side of the body and 1.252 to 1.339 on the nondominant side. Neither stratification by demographic variables nor normalization of ECW to ICW improved diagnostic performance of arm-to-leg ratios.
The second approach for deriving cut-offs involved construction of ROC curves by using unadjusted and adjusted arm-to-leg ratios and selection of optimal cut-offs based on clinically informed decision making. Comparison of McFadden's R2 values (as a measure of model fit) and AUCs (as a measure of accuracy) of unadjusted and adjusted logistic regression models suggests that adding sex, age, and BMI to the model significantly improves diagnostic performance of arm-to-leg ratios. Indeed, unadjusted ratios produced AUCs of 0.79 to 0.86, indicative of fair to good accuracy; whereas adjusted models produced AUCs between 0.89 and 0.93, indicative of good to excellent accuracy.
In selecting optimal cut-offs, we considered the relative consequences of false-negative and false-positive test results (e.g., missed opportunity for prevention and development of chronic lymphedema versus unnecessary follow-up screening and/or provision of a noninvasive therapy such as lymphatic drainage massage) and chose to maximize sensitivity while maintaining acceptable specificity (>0.7). Interestingly, our ROC curve-derived cut-offs for unadjusted R0 ratios (dominant = 1.217, nondominant = 1.211) were similar to cut-offs based on the normative mean + 0.5 SD (dominant = 1.209, nondominant = 1.252).
In contrast, the ROC curve-derived cut-offs for Ri:R0 ratios (dominant = 0.903, nondominant = 0.905) were smaller than normative data-derived cut-offs (dominant = 1.421, nondominant = 1.301), and significantly better at detecting lymphedema. Cut-offs derived from adjusted ROC curves showed significantly better sensitivity and specificity than cut-offs derived from unadjusted ROC curves and normative data-derived cut-offs. Therefore, we propose that the following predictive equations based on regression coefficients from the adjusted logistic regression models, could be used for accurately detecting bilateral, lower-limb lymphedema:
Dominant side of the body:
predictor = −18.41 + 5.58(arm R0/leg R0) − 0.45(male = 1|female = 0) + 0.03(age) +0.24(BMI)
probability = exp(predictor)/(1+exp(predictor))
probability >0.045 = lymphedema
Nondominant side of the body:
predictor = −18.59 + 6.11(arm R0/leg R0) − 0.44(male = 1|female = 0) + 0.02(age) +0.24(BMI)
probability = exp(predictor)/(1+exp(predictor))
probability >0.042 = lymphedema
Further, despite having reduced sensitivity and specificity, the following raw arm-to-leg ratios of ECW could be used for detection of lower-limb lymphedema if demographic data were unavailable or as a quick and easy, but less reliable preliminary diagnostic tool.
Dominant side of the body:
arm R0/leg R0 > 1.217 = lymphedema
Nondominant side of the body:
arm R0/leg R0 > 1.211 = lymphedema
Although a limited number of studies have explored the potential of using BIS for detecting lower-limb lymphedema,10,12,13,19,20 we present the first sensitive and specific BIS-based diagnostic cut-offs that do not rely on baseline (prelymphedema) measures and can be easily applied in the clinic.
Novackova et al. 20 have previously tested two BIS-based methods of detecting lower-limb lymphedema in 29 patients who were assessed by using BIS before and 6 months after surgery for vulvar cancer. The first method diagnosed lymphedema if leg ECW at 6 months postsurgery was greater than 1.645 SD from the leg ECW presurgery, whereas the second method diagnosed lymphedema if the leg ECW at 6 months was 140% of leg ECW presurgery. Both methods showed a sensitivity of 0.67, but the second method showed greater specificity (0.6 vs. 0.45). However, not only does this method rely on the collection of a baseline measurement, but also it appears to be less sensitive and less specific than the criteria presented herein.
BIS-based diagnosis has been used extensively in the detection of breast cancer-related lymphedema. The diagnostic performance of our proposed criteria for detecting lower-limb lymphedema (sensitivity = 0.87–89; specificity = 0.83; AUC = 0.93) is in line with the published performance of cut-offs for unilateral, upper-limb lymphedema. For example, Smoot et al. 21 assessed the diagnostic ability of the BIS cut-offs for unilateral, upper-limb lymphedema published by Cornish et al., 22 and they found a sensitivity of 0.31 to 0.87, a specificity of 0.47 to 1, and an AUC of 0.88. More recently, Dylke et al. 23 assessed the ability of a range of BIS cut-offs to detect unilateral, upper-limb lymphedema and found that sensitivity ranged from 0.93 to 0.96 and specificity ranged from 0.67 to 0.87.
Although the findings presented here are relevant and ready for use in the research and clinical setting, limitations to this work need to be acknowledged. First, our control and case data come from convenience sampling, with males under-represented in each dataset and cases having higher BMI on average compared with controls. Group differences between cases and controls may partly explain why the prediction equation performs better than the unstratified and age- and sex-stratified diagnostic thresholds, as presented here.
Second, although the majority of our lymphedema cases were more likely to have stage II+ lymphedema, we have limited information on the cause or composition of their lymphedema. Consequently, we were unable to explore any potential impact of these factors on the performance of the diagnostic criteria. Future research in evaluating the diagnostic potential of the proposed cut-offs in a sample with mixed lymphedema stage, as well as testing the performance of the cut-offs in the bilateral, upper-limb lymphedema setting, is clearly warranted.
It is well known that the outcomes of sensitivity and specificity analysis are highly dependent on the choice of the reference method. 24 Although there exists no gold standard for the diagnosis of lymphedema, a strength of this work is that our cases had clinically confirmed lower-limb lymphedema, as assessed by an experienced lymphedema therapist. As noted earlier, we prioritized sensitivity over specificity in identifying the proposed diagnostic thresholds. This was not only standard for analysis that seeks to identify a diagnostic threshold, but it was also particularly appropriate here, given that our controls did not undergo a clinical evaluation and may have included individuals with increases in extracellular fluid unrelated to cancer.
Nonetheless, by prioritizing sensitivity over specificity, and in acknowledgment that BIS measures fluid changes and differences, irrespective of cause, the diagnostic threshold specified may be more likely to over- than underdiagnose cases. Overdiagnosis through use of these criteria could be reduced by also considering patient-reported symptoms and/or other clinical assessments. Further, we have reported the sensitivity and specificity of a range of cut-offs in the Supplementary Table S1 to allow for future use of different cut-offs based on different criteria or priorities.
In conclusion, we present BIS criteria for detecting lymphedema in individuals at risk of lower-limb lymphedema who do not rely on comparison to baseline or contralateral limb measures. Further, findings suggest that unstratified arm-to-leg ratios of ECW are sensitive and specific; whereas the prediction equations based on sex, age, and BMI-adjusted logistic regression models showed excellent sensitivity and specificity, and they are easily translatable to the clinic.
Footnotes
Author Disclosure Statement
No competing financial interests exist. L.C.W. provides consultancy services to ImpediMed Limited. Impedimed Limited donated dual-tab electrodes to S.G. S.D.P. holds the Fonterra Chair in Human Nutrition at the University of Auckland. AR is an employee of Fonterra Co-Operative Group. A.O. is the founder and managing director of SurgicalPerformance Pty Ltd., an Australian, private company that provides surgeons with a platform for collection of surgical outcome audit data; A.O. received travel grants from the O.R. Company (formerly Tyco Healthcare) and is a consultant for Covidien, NSW, Australia.
Funding Information
The authors wish to thank and acknowledge the following organizations for contribution of funds that enabled this work to be completed: Impedimed Limited (funds supported the data analysis for this body of work but not the original data collection studies), Cancer Council Queensland (SH fellowship and RB grant), National Health and Medical Research Council (MJ fellowship), Department of Health and Aging (RB grant), Fonterra Co-operative Group, and the New Zealand Ministry for Primary Industries (funds supported the New Zealand Primary Growth Partnership post-farm gate dairy program). Funding received had no influence over data analysis and reporting.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.