
Abstract

Featured Article
Beerens, M., et al. (2018). “Multipotent adult progenitor cells support lymphatic regeneration at multiple anatomical levels during wound healing and lymphedema.” Sci Rep 8(1): 3852.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5832783/pdf/41598_2018_Article_21610.pdf
Lymphatic capillary growth is an integral part of wound healing, yet, the combined effectiveness of stem/progenitor cells on lymphatic and blood vascular regeneration in wounds needs further exploration. Stem/progenitor cell transplantation also emerged as an approach to cure lymphedema, a condition caused by lymphatic system deficiency. While lymphedema treatment requires lymphatic system restoration from the capillary to the collector level, it remains undetermined whether stem/progenitor cells support a complex regenerative response across the entire anatomical spectrum of the system. Here, we demonstrate that, although multipotent adult progenitor cells (MAPCs) showed potential to differentiate down the lymphatic endothelial lineage, they mainly trophically supported lymphatic endothelial cell behaviour in vitro. In vivo, MAPC transplantation supported blood vessel and lymphatic capillary growth in wounds and restored lymph drainage across skin flaps by stimulating capillary and pre-collector vessel regeneration. Finally, human MAPCs mediated survival and functional reconnection of transplanted lymph nodes to the host lymphatic network by improving their (lymph)vascular supply and restoring collector vessels. Thus, MAPC transplantation represents a promising remedy for lymphatic system restoration at different anatomical levels and hence an appealing treatment for lymphedema. Furthermore, its combined efficacy on lymphatic and blood vascular growth is an important asset for wound healing.
In this manuscript, the authors study multipotent bone marrow derived adult progenitor cells (MAPCs) as a potential option to promote therapeutic lymphangiogenesis. Using a variety of assays, the studies suggest that this intervention may provide a means to treat disorders of lymphatic dysfunction. Below are the findings based on this work:
1. MAPCs have lymphvasculogenic and lymphangiogenic potential: Exposure to VEGF-A (but not VEGFC) resulted in MAPCs Prox-1 and LYVE-1 induction, and MAPC conditioned medium stimulated lymphatic growth (sprouting, migration, and migration) in vitro, suggesting MAPCs provide “trophic support” to vascular endothelium. 2. MAPCs support lymphatic capillary growth in healing wounds: In a mouse wound model, exposure to mouse MAPCs demonstrated decreased wound gaps, improved scarring, and stimulation of angiogenesis and lymphangiogenesis. 3. MAPCs support lymphatic capillary and pre-collector restoration in elevated skin flaps: In a mouse model of lymphatic vessel disruption, lymphatic drainage was reestablished after treatment with MAPCs, with documentation of a restored and sustained lymphatic capillary network at the incision site. 4. hMAPCs reconnect transplanted lymph nodes to the host lymphatic network: To demonstrate the restoration of a “lymphatic collector system”, allowing for drainage of lymphatic fluid (important in the treatment of lymphedema), studies showed MAPC treated transplanted lymph node function, collector vessels, and fluid drainage.
Figure 1 summarizes the data in this study:
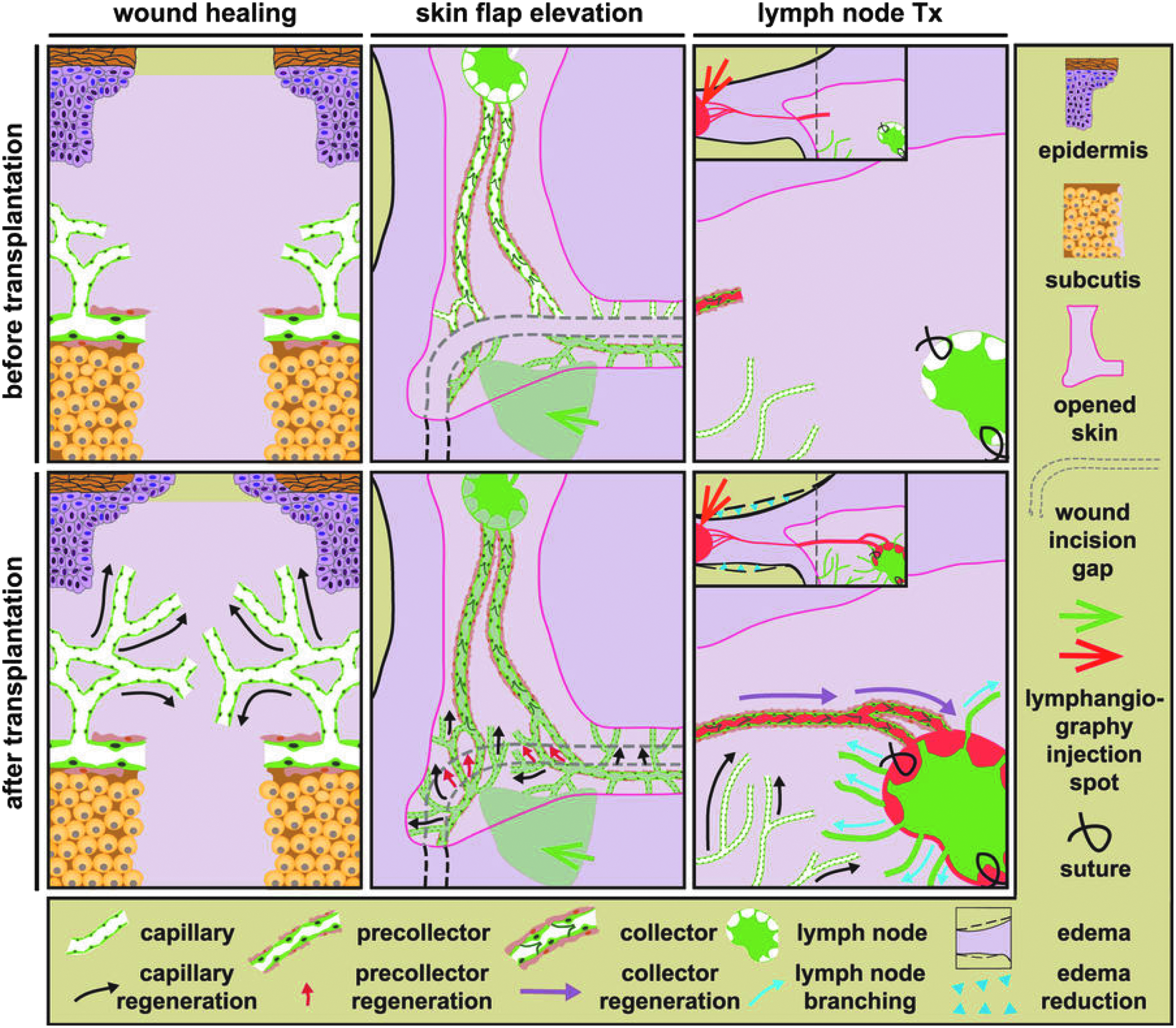
Multipotent adult progenitor cells (MAPCs) support lymphatic regeneration at multiple anatomical levels. Following transplantation in different models, MAPCs stimulated lymphatic regeneration on three different anatomical levels. MAPCs stimulated capillary growth (black arrows) in all models and in addition boosted pre-collector regeneration in the skin flap model (red arrows) and collector restoration and lymph node (LN) reconnection (purple Arrows) in the LN transplantation (Tx) model, thereby reducing edema (blue arrow heads). Finally, hMAPCs stimulated outward branching of the transplanted LN vasculature (blue arrows). Beerens M et al, “Multipotent adult progenitor cells support lymphatic regeneration at multiple anatomical levels during wound healing and lymphedema.” 2018. Sci Rep 8(1): 3852. This article is licensed under a Creative Commons Attribution 4.0 International License. A color version of this figure is available in the online article at www.liebertpub.com/LRB.
Basic Science
Alsina-Sanchis, E., et al. (2018). “ALK1 (activin-receptor like kinase 1) loss results in vascular hyperplasia in mice and humans through PI3K (phosphatidylinositol 3-kinase) activation.” Arterioscler Thromb Vasc Biol. [EPub Feb 15]
Denorme, P., et al. (2018). “Phosphatidylinositol-4,5-bisphosphate 3-kinase catalytic subunit alpha (PIK3CA)-related overgrowth spectrum: A brief report.” Pediatr Dermatol. [EPub March 1]
di Blasio, L., et al. (2018). “PI3K/mTOR inhibition promotes the regression of experimental vascular malformations driven by PIK3CA-activating mutations.” Cell Death Dis 9(2): 45.
Frosen, J. and A. Joutel (2018). “Smooth muscle cells of intracranial vessels: from development to disease.” Cardiovasc Res 114(4): 501–512.
Fujii, H., et al. (2018). “Optimal range of injection rates for a lymphatic drug delivery system.” J Biophotonics. [EPub Feb 20]
The lymphatic drug delivery system (LDDS) is a new technique that permits the injection of drugs into a sentinel lymph node (SLN) at an early stage of tumor metastasis, thereby treating metastasis in the SLN and its secondary lymph nodes (LNs). The quantity of drug required for a LDDS is much smaller than that needed for systemic chemotherapy. However, the relationship between the rate of drug injection into a SLN and the amount of drug reaching the secondary LNs has not been investigated. In this study, we used an MXH10/Mo-lpr/lpr mouse model to show that the optimal rate for the injection of a fluorescent dye by a LDDS was 10-80 muL/min. An injection rate of 10-80 muL/min was able to fill the downstream LN. However, an injection rate of 100 muL/min drove the fluorescent dye into the efferent lymphatic vessels and thoracoepigastric vein, decreasing the amount of dye retained in the downstream LN. Bolus injection (defined as an injection rate of 2,400 muL/min) was unable to deliver fluorescent dye into the downstream LN. These results agree with the impulse values calculated from the injection pressures in the upstream LN. We anticipate that our findings will facilitate the development of a LDDS for use in the clinic.
Ge, Y., et al. (2018). “Adipokine apelin ameliorates chronic colitis in Il-10(-/-) mice by promoting intestinal lymphatic functions.” Biochem Pharmacol 148: 202–212.
Both mesenteric adipose tissue (MAT) and lymphatic vessels (LVs) play important roles in the pathogenesis of Crohn's disease (CD), and adipokines have been implicated in the crosstalk between MAT and LVs. Apelin, a newly identified adipokine, has been demonstrated to be crucial in the development and stabilization of LVs. We aimed to identify the expression of apelin in MAT of CD patients and explore whether apelin influences the disease course in murine colitis and determine its contributions to LVs. Expression of apelin in MAT specimens from patients with CD (n = 24) and without CD (control, n = 12) was detected. Il-10 deficient (Il-10(-/-)) mice with established colitis were administered apelin, and untreated and wild-type mice served as controls (n = 8 for each group). Disease activity and colonic inflammation was evaluated. The LV density, lymphatic drainage function and related signaling pathways were also analyzed. We found that MAT from CD patients expressed a higher level of apelin compared with that from controls. Systemic delivery of apelin significantly ameliorated chronic colitis in Il-10(-/-) mice, demonstrated by decreased disease activity index and inflammatory scores, and lower levels of Tnf-alpha, Il-1beta and Il-6. Increased LV density and podoplanin levels indicated that apelin promoted lymphangiogenesis. Evans blue dye and fluorescent lymphangiography revealed an enhanced lymphatic drainage function in apelin-treated mice. The role of apelin was found to be related to the activation of the Akt and Erk signaling pathways. These results indicate that the adipokine apelin was highly expressed in MAT of CD patients and has a promising role in ameliorating experimental colitis by promoting intestinal lymphatic functions, suggesting the potential crosstalk between adipokines and LVs in MAT in CD status. Therapies with adipokines, such as apelin, may be a novel approach for the treatment of CD.
Glaser, K., et al. (2018). “Linkage of metabolic defects to activated PIK3CA alleles in endothelial cells derived from lymphatic malformation.” Lymphat Res Biol 16(1): 43–55.
BACKGROUND: Lymphatic endothelial cells (LECs) derived from lymphatic malformations (LMs) bear activated PIK3CA alleles yet display an inflammatory gene expression profile. A basis for the inflammatory phenotype was sought by screening for coexisting somatic mutations. METHODS AND RESULTS: Fourteen independent LEC populations bearing activated PIK3CA alleles were isolated from LM. These were characterized by the expression of growth and inflammatory genes (VEGFC, IL-6, COX-2, IL-8, HO-1, E-SEL) by qRT-PCR. Most commonly upregulated gene products were VEGFC, COX2, HO-1, and ANGPTL4. The specific inhibition of PI3K reduced VEGFC expression without resolving inflammation. Whole exome sequencing of six LM-LEC populations identified five novel somatically acquired alleles coexisting with activated PIK3CA alleles. Two affected genes regulate lipid droplet metabolism (FITM2 and ATG2A), two are gene regulators (MTA1 and TAF1L), and the fifth is an isoform of ANK3 (an endosomal/lysosomal protein). Inhibition of AMPK implicated its involvement in regulating COX-2 and HO-1 overexpression. ANGPTL4 expression was independent of AMPK and PI3K activity and reflected lipid stress demonstrated in normal LECs. AMPK activation with AICAR had a selective growth-limiting effect in a subset of LM-LEC isolates. CONCLUSIONS: Inflammatory stress displayed by LM-LECs is consistent with errors in lipid metabolism that may be linked to acquired mutations. The acquisition of PIK3CA alleles may be a permissive event that antagonizes inflammation and metabolic defect.
Gucciardo, E., et al. (2018). “Microenvironment of proliferative diabetic retinopathy supports lymphatic neovascularization.” J Pathol. [EPub March 13]
Proliferative diabetic retinopathy (PDR) is a major diabetic microvascular complication characterized by pathological angiogenesis. Several retinopathy animal models have been developed to study the disease mechanisms and putative targets. However, knowledge on the human proliferative disease remains incomplete, relying on steady-state results from thin histological neovascular tissue sections and vitreous samples. New translational models are thus required to comprehensively understand the disease pathophysiology and develop improved therapeutic interventions. We describe here a clinically relevant model, whereby the native multicellular PDR landscape and neo(fibro)vascular processes can be analyzed ex vivo and related to clinical data. As characterized by 3D whole-mount immunofluorescence and electron microscopy, heterogeneity in patient-derived PDR neovascular tissues included discontinuous capillaries coupled with aberrantly differentiated, lymphatic-like, and tortuous endothelia. Spatially-confined apoptosis and proliferation co-existed with inflammatory cell infiltration and unique vascular islet formation. Ex vivo-cultured explants sustained multicellularity, islet patterning and capillary or fibrotic outgrowth in response to vitreoretinal factors. Strikingly, PDR neovascular tissues, whose matched vitreous enhanced lymphatic endothelial cell sprouting, contained lymphatic-like capillaries in vivo and developed Prox1(+) capillaries and sprouts with lymphatic endothelial ultrastructures ex vivo. Among elaborate vitreal components, VEGFC was one factor found at lymphatic endothelium activating concentrations. These results indicate that the ischemia- and inflammation-induced human PDR microenvironment supports pathological neolymphvascularization, bringing a new concept to the PDR mechanisms and targeting options.
Hachiya, H. L., et al. (1986). “Comparative studies on insulin-like growth factor II and insulin processing by vascular endothelial cells.” Diabetes 35(10): 1065–1072.
Izen, R. M., et al. (2018). “Postnatal development of lymphatic vasculature in the brain meninges.” Dev Dyn. [EPub March 1]
BACKGROUND: Traditionally, the central nervous system (CNS) has been viewed as an immune-privileged environment with no lymphatic vessels. This view was partially overturned by the discovery of lymphatic vessels in the dural membrane that surrounds the brain, in contact with the interior surface of the skull. We here examine the distribution and developmental timing of these lymphatic vessels. RESULTS: Using the Prox1-GFP BAC transgenic reporter and immunostaining with antibodies to lymphatic markers LYVE-1, Prox1, and Podoplanin, we have carried out whole-mount imaging of dural lymphatic vasculature at postnatal stages. We have found that between birth - postnatal day 13 (P)13, lymphatic vessels extend alongside dural blood vessels from the side of the skull towards the midline. Between P13 - P20, lymphatic vessels along the transverse sinuses (TS) reach the superior sagittal sinus (SSS) and extend along the SSS towards the olfactory bulb. CONCLUSION: Compared with the embryonic developmental timing of lymphatic vessels in other tissues, e.g. skin, dural lymphatic vessel development is dramatically delayed. This study provides useful anatomical data for continuing investigations of the fundamental mechanisms that underlie dural lymphatic vessel development.
Jackson, D. G. (2018). “Hyaluronan in the lymphatics: The key role of the hyaluronan receptor LYVE-1 in leucocyte trafficking.” Matrix Biol. [EPub Feb 6]
LYVE-1, a close relative of the leucocyte receptor, CD44, is the main receptor for hyaluronan (HA) in lymphatic vessel endothelium and a widely used marker for distinguishing between blood and lymphatic vessels. Enigmatic for many years because of its anomalous HA-binding characteristics, the function of LYVE-1 has just recently been identified as that of a lymphatic docking receptor for dendritic cells, selectively engaging with their surface HA glycocalyx to regulate entry to peripheral lymphatics and migration to downstream lymph nodes for immune activation. Furthermore, LYVE-1 mediates the trafficking of macrophages, and is also exploited by HA-encapsulated Group A streptococci for lymphatic invasion and host dissemination. Consistent with a role in lymphatic trafficking, the interaction of LYVE-1 with HA and its degradation products can also activate intracellular signalling pathways for endothelial junctional retraction and lymphatic endothelial proliferation. Here we outline the latest findings on the receptor in the context of its peculiar biochemical properties and speculate on how the interaction of LYVE-1 with different HA sizes and conformations might variably influence cell function as a consequence of avidity and receptor crosslinking. Finally, we evaluate evidence that LYVE-1 can also bind growth factors and associate with kinase-linked growth factor receptors and conclude on how the LYVE-1.HA axis may be exploited as a target to either block inflammation or tissue allograft rejection, or potentiate vaccine and drug delivery.
Jaldin-Fincati, J. R., et al. (2018). “Insulin uptake and action in microvascular endothelial cells of lymphatic and blood origin.” Am J Physiol Endocrinol Metab. [EPub March 6]
Whereas the blood microvasculature constitutes a biological barrier to the action of blood-borne insulin on target tissues, the lymphatic microvasculature might act as a barrier to subcutaneously administrated insulin reaching the circulation. Here, we evaluate the interaction of insulin with primary microvascular endothelial cells of lymphatic (HDLEC) and blood (HAMEC) origin, derived from human dermal and adipose tissues, respectively. HDLEC express higher levels of insulin receptor (IR) and signal in response to insulin as low as 2.5 nM, while HAMEC only activate signalling at 100 nM (a dose that blood vessels do not normally encounter). Low insulin acts specifically through IR, while supra-physiological insulin acts through both the IR and Insulin Growth Factor-1 receptor (IGF-1R). At supra-physiological or injection site-compatible doses pertinent to lymphatic microvessels, insulin enters HAMEC and HDLEC via fluid-phase endocytosis. Conversely, at physiologically-circulating doses (0.2 nM) pertinent to blood microvessels, insulin enters HAMEC through a receptor-mediated process requiring IR autophosphorylation but not downstream insulin signalling. At physiological doses, internalized insulin is barely degraded, and is instead released intact to the extracellular medium. In conclusion, we document for the first time the mechanism of interaction of insulin with lymphatic endothelial cells, which may be relevant to insulin absorption during therapeutic injections. Further, we describe distinct action and uptake routes for insulin at physiological and supra-physiological doses in blood microvascular endothelial cells, providing a potential explanation for previously conflicting studies on endothelial insulin uptake.
Kraft, J. C., et al. (2018). “Indocyanine green nanoparticles undergo selective lymphatic uptake, distribution and retention and enable detailed mapping of lymph vessels, nodes and abnormalities.” J Drug Target: 1–11.
Lee, H. R., et al. (2018). “Deregulation of HDAC5 by viral interferon regulatory factor 3 plays an essential role in kaposi's sarcoma-associated herpesvirus-induced lymphangiogenesis.” MBio 9(1).
Lohrberg, M., et al. (2018). “Co-localization of lymphoid aggregates and lymphatic networks in nose- (NALT) and lacrimal duct-associated lymphoid tissue (LDALT) of mice.” BMC Immunol 19(1): 5.
BACKGROUND: The lymphatic vascular pattern in the head of mice has rarely been studied, due to problems of sectioning and immunostaining of complex bony structures. Therefore, the association of head lymphoid tissues with the lymphatics has remained unknown although the mouse is the most often used species in immunology. RESULTS: Here, we studied the association of nasal and nasolacrimal duct lymphatics with lymphoid aggregates in 14-day-old and 2-month-old mice. We performed paraffin sectioning of whole, decalcified heads, and immunostaining with the lymphatic endothelial cell-specific antibodies Lyve-1 and Podoplanin. Most parts of the nasal mucous membrane do not contain any lymphatics. Only the region of the inferior turbinates contains lymphatic networks, which are connected to those of the palatine. Nose-associated lymphoid tissue (NALT) is restricted to the basal parts of the nose, which contain lymphatics. NALT is continued occipitally and can be found at both sides along the sphenoidal sinus, again in close association with lymphatic networks. Nasal lymphatics are connected to those of the ocular region via a lymphatic network along the nasolacrimal duct (NLD). By this means, lacrimal duct-associated lymphoid tissue (LDALT) has a dense supply with lymphatics. CONCLUSIONS: NALT and LDALT play a key role in the immune system of the mouse head, where they function as primary recognition sites for antigens. Using the dense lymphatic networks along the NLD described in this study, these antigens reach lymphatics near the palatine and are further drained to lymph nodes of the head and neck region. NALT and LDALT develop in immediate vicinity of lymphatic vessels. Therefore, we suggest a causative connection of lymphatic vessels and the development of lymphoid tissues.
Matsuoka, R. L. and D. Y. R. Stainier (2018). “Recent insights into vascular development from studies in zebrafish.” Curr Opin Hematol. [EPub Feb 12]
PURPOSE OF REVIEW: Zebrafish has provided a powerful platform to study vascular biology over the past 25 years, owing to their distinct advantages for imaging and genetic manipulation. In this review, we summarize recent progress in vascular biology with particular emphasis on vascular development in zebrafish. RECENT FINDINGS: The advent of transcription activator-like effector nuclease and clustered regularly interspaced short palindromic repeats (CRISPR)/CRISPR-associated protein 9 genome-editing technologies has dramatically facilitated reverse genetic approaches in zebrafish, as in other models. Here, we highlight recent studies on vascular development in zebrafish which mainly employed forward or reverse genetics combined with high-resolution imaging. These studies have advanced our understanding of diverse areas in vascular biology, including transcriptional regulation of endothelial cell differentiation, endothelial cell signaling during angiogenesis and lymphangiogenesis, vascular bed-specific developmental mechanisms, and perivascular cell recruitment. SUMMARY: The unique attributes of the zebrafish model have allowed critical cellular and molecular insights into fundamental mechanisms of vascular development. Knowledge acquired through recent zebrafish work further advances our understanding of basic mechanisms underlying vascular morphogenesis, maintenance, and homeostasis. Ultimately, insights provided by the zebrafish model will help to understand the genetic, cellular, and molecular underpinnings of human vascular malformations and diseases.
Missinato, M. A., et al. (2018). “Dusp6 attenuates Ras/MAPK signaling to limit zebrafish heart regeneration.” Development 145(5).
Zebrafish regenerate cardiac tissue through proliferation of pre-existing cardiomyocytes and neovascularization. Secreted growth factors such as FGFs, IGF, PDGFs and Neuregulin play essential roles in stimulating cardiomyocyte proliferation. These factors activate the Ras/MAPK pathway, which is tightly controlled by the feedback attenuator Dual specificity phosphatase 6 (Dusp6), an ERK phosphatase. Here, we show that suppressing Dusp6 function enhances cardiac regeneration. Inactivation of Dusp6 by small molecules or by gene inactivation increased cardiomyocyte proliferation, coronary angiogenesis, and reduced fibrosis after ventricular resection. Inhibition of Erbb or PDGF receptor signaling suppressed cardiac regeneration in wild-type zebrafish, but had a milder effect on regeneration in dusp6 mutants. Moreover, in rat primary cardiomyocytes, NRG1-stimulated proliferation can be enhanced upon chemical inhibition of Dusp6 with BCI. Our results suggest that Dusp6 attenuates Ras/MAPK signaling during regeneration and that suppressing Dusp6 can enhance cardiac repair.
Oren, R., et al. (2018). “Whole organ blood and lymphatic vessels imaging (WOBLI).” Sci Rep 8(1): 1412.
Thin section histology is limited in providing 3D structural information, particularly of the intricate morphology of the vasculature. Availability of high spatial resolution imaging for thick samples, would overcome the restriction dictated by low light penetration. Our study aimed at optimizing the procedure for efficient and affordable tissue clearing, along with an appropriate immunofluorescence labeling that will be applicable for high resolution imaging of blood and lymphatic vessels. The new procedure, termed whole organ blood and lymphatic vessels imaging (WOBLI), is based on two previously reported methods, CLARITY and ScaleA2. We used this procedure for the analysis of isolated whole ovary, uterus, lung and liver. These organs were subjected to passive clearing, following fixation, immunolabeling and embedding in hydrogel. Cleared specimens were immersed in ScaleA2 solution until transparency was achieved and imaged using light sheet microscopy. We demonstrate that WOBLI allows detailed analysis and generation of structural information of the lymphatic and blood vasculature from thick slices and more importantly, from whole organs. We conclude that WOBLI offers the advantages of morphology and fluorescence preservation with efficient clearing. Furthermore, WOBLI provides a robust, cost-effective method for generation of transparent specimens, allowing high resolution, 3D-imaging of blood and lymphatic vessels networks.
Rauniyar, K., et al. (2018). “Biology of vascular endothelial growth factor C in the morphogenesis of lymphatic vessels.” Front Bioeng Biotechnol 6: 7.
Because virtually all tissues contain blood vessels, the importance of hemevascularization has been long recognized in regenerative medicine and tissue engineering. However, the lymphatic vasculature has only recently become a subject of interest. Central to the task of growing a lymphatic network are lymphatic endothelial cells (LECs), which constitute the innermost layer of all lymphatic vessels. The central molecule that directs proliferation and migration of LECs during embryogenesis is vascular endothelial growth factor C (VEGF-C). VEGF-C is therefore an important ingredient for LEC culture and attempts to (re)generate lymphatic vessels and networks. During its biosynthesis VEGF-C undergoes a stepwise proteolytic processing, during which its properties and affinities for its interaction partners change. Many of these fundamental aspects of VEGF-C biosynthesis have only recently been uncovered. So far, most-if not all-applications of VEGF-C do not discriminate between different forms of VEGF-C. However, for lymphatic regeneration and engineering purposes, it appears mandatory to understand these differences, since they relate, e.g., to important aspects such as biodistribution and receptor activation potential. In this review, we discuss the molecular biology of VEGF-C as it relates to the growth of LECs and lymphatic vessels. However, the properties of VEGF-C are similarly relevant for the cardiovascular system, since both old and recent data show that VEGF-C can have a profound effect on the blood vasculature.
Salvi, V., et al. (2016). “Dendritic cell-derived VEGF-A plays a role in inflammatory angiogenesis of human secondary lymphoid organs and is driven by the coordinated activation of multiple transcription factors.” Oncotarget 7(26): 39256–39269.
Lymph node expansion during inflammation is essential to establish immune responses and relies on the development of blood and lymph vessels. Previous work in mice has shown that this process depends on the presence of VEGF-A produced by B cells, macrophages and stromal cells. In humans, however, the cell types and the mechanisms regulating the intranodal production of VEGF-A remain elusive. Here we show that CD11c+ cells represent the main VEGF-A-producing cell population in human reactive secondary lymphoid organs. In addition we find that three transcription factors, namely CREB, HIF-1alpha and STAT3, regulate the expression of VEGF-A in inflamed DCs. Both HIF-1alpha and STAT3 are activated by inflammatory agonists. Conversely, CREB phosphorylation represents the critical contribution of endogenous or exogenous PGE2. Taken together, these results propose a crucial role for DCs in lymph node inflammatory angiogenesis and identify novel potential cellular and molecular targets to limit inflammation in chronic diseases and tumors.
Sugden, W. W. and A. F. Siekmann (2018). “Endothelial cell biology of Endoglin in hereditary hemorrhagic telangiectasia.” Curr Opin Hematol. [EPub Feb 12]
PURPOSE OF REVIEW: Mutations in the Endoglin (Eng) gene, an auxiliary receptor in the transforming growth factor beta (TGFbeta)-superfamily signaling pathway, are responsible for the human vascular disorder hereditary hemorrhagic telangiectasia (HHT) type 1, characterized in part by blood vessel enlargement. A growing body of work has uncovered an autonomous role for Eng in endothelial cells. We will highlight the influence of Eng on distinct cellular behaviors, such as migration and shape control, which are ultimately important for the assignment of proper blood vessel diameters. RECENT FINDINGS: How endothelial cells establish hierarchically ordered blood vessel trees is one of the outstanding questions in vascular biology. Mutations in components of the TGFbeta-superfamily of signaling molecules disrupt this patterning and cause arteriovenous malformations (AVMs). Eng is a TGFbeta coreceptor enhancing signaling through the type I receptor Alk1. Recent studies identified bone morphogenetic proteins (BMPs) 9 and 10 as the primary ligands for Alk1/Eng. Importantly, Eng potentiated Alk1 pathway activation downstream of hemodynamic forces. New results furthermore revealed how Eng affects endothelial cell migration and cell shape control in response to these forces, thereby providing new avenues for our understanding of AVM cause. SUMMARY: We will discuss the interplay of Eng and hemodynamic forces, such as shear stress, in relation to Alk1 receptor activation. We will furthermore detail how this signaling pathway influences endothelial cell behaviors important for the establishment of hierarchically ordered blood vessel trees. Finally, we will provide an outlook how these insights might help in developing new therapies for the treatment of HHT.
Urner, S., et al. (2018). “Mechanotransduction in blood and lymphatic vascular development and disease.” Adv Pharmacol 81: 155–208.
The blood and lymphatic vasculatures are hierarchical networks of vessels, which constantly transport fluids and, therefore, are exposed to a variety of mechanical forces. Considering the role of mechanotransduction is key for fully understanding how these vascular systems develop, function, and how vascular pathologies evolve. During embryonic development, for example, initiation of blood flow is essential for early vascular remodeling, and increased interstitial fluid pressure as well as initiation of lymph flow is needed for proper development and maturation of the lymphatic vasculature. In this review, we introduce specific mechanical forces that affect both the blood and lymphatic vasculatures, including longitudinal and circumferential stretch, as well as shear stress. In addition, we provide an overview of the role of mechanotransduction during atherosclerosis and secondary lymphedema, which both trigger tissue fibrosis.
Van de Velde, M., et al. (2018). “Ear sponge assay: A method to investigate angiogenesis and lymphangiogenesis in mice.” Methods Mol Biol 1731: 223–233.
Angiogenesis and lymphangiogenesis have become important research areas in the biomedical field. The outgrowth of new blood (angiogenesis) and lymphatic (lymphangiogenesis) vessels from preexisting ones is involved in many pathologies including cancer. In-depth investigations of molecular determinants such as proteases in these complex processes require reliable in vivo models. Here we present the ear sponge assay as an easy, rapid, quantitative and reproducible model of angiogenesis and lymphangiogenesis. In this system, a gelatin sponge soaked with tumor cells, cell-conditioned medium, or a compound to be tested is implanted, for 2-4 weeks, between the two mouse ear skin layers. The two vascular networks are next examined through histological procedures.
Yamakawa, M., et al. (2018). “Potential lymphangiogenesis therapies: Learning from current antiangiogenesis therapies-A review.” Med Res Rev. [EPub March 12]
In recent years, lymphangiogenesis, the process of lymphatic vessel formation from existing lymph vessels, has been demonstrated to have a significant role in diverse pathologies, including cancer metastasis, organ graft rejection, and lymphedema. Our understanding of the mechanisms of lymphangiogenesis has advanced on the heels of studies demonstrating vascular endothelial growth factor C as a central pro-lymphangiogenic regulator and others identifying multiple lymphatic endothelial biomarkers. Despite these breakthroughs and a growing appreciation of the signaling events that govern the lymphangiogenic process, there are no FDA-approved drugs that target lymphangiogenesis. In this review, we reflect on the lessons available from the development of antiangiogenic therapies (26 FDA-approved drugs to date), review current lymphangiogenesis research including nanotechnology in therapeutic drug delivery and imaging, and discuss molecules in the lymphangiogenic pathway that are promising therapeutic targets.
Zhang, Y., et al. (2018). “Transient loss of venous integrity during developmental vascular remodeling leads to red blood cell extravasation and clearance by lymphatic vessels.” Development 145(3).
Maintenance of blood vessel integrity is crucial for vascular homeostasis and is mainly controlled at the level of endothelial cell (EC) junctions. Regulation of endothelial integrity has largely been investigated in the mature quiescent vasculature. Less is known about how integrity is maintained during vascular growth and remodeling involving extensive junctional reorganization. Here, we show that embryonic mesenteric blood vascular remodeling is associated with a transient loss of venous integrity and concomitant extravasation of red blood cells (RBCs), followed by their clearance by the developing lymphatic vessels. In wild-type mouse embryos, we observed activated platelets extending filopodia at sites of inter-EC gaps. In contrast, embryos lacking the activatory C-type lectin domain family 1, member b (CLEC1B) showed extravascular platelets and an excessive number of RBCs associated with and engulfed by the first lymphatic EC clusters that subsequently form lumenized blood-filled vessels connecting to the lymphatic system. These results uncover novel functions of platelets in maintaining venous integrity and lymphatic vessels in clearing extravascular RBCs during developmental remodeling of the mesenteric vasculature. They further provide insight into how vascular abnormalities characterized by blood-filled lymphatic vessels arise.
Clinical
Agko, M., et al. (2018). “Staged surgical treatment of extremity lymphedema with dual gastroepiploic vascularized lymph node transfers followed by suction-assisted lipectomy-A prospective study.” J Surg Oncol. [EPub Jan 22]
Aguiar-Santos, A. M., et al. (2018). “Immunomodulation of allergic response in children and adolescents: What we can learn from lymphatic filarial infection.” Allergol Immunopathol (Madr) 46(2): 167–174.
BACKGROUND: Although it is well known that allergic diseases involve a strong Th2 immune response, with production of high levels of specific IgE allergen, knowledge on the association between filarial infection and allergies, among paediatric patients is scarce. OBJECTIVE: To evaluate the allergic response patterns in cases of filarial infection by comparing peripheral eosinophils, total IgE levels, immediate hypersensitivity and cytokine levels in children and adolescents in Brazil. METHODS: This was an exploratory study with three groups: (I) with filarial infection and without allergic diseases; (II) without filarial infection and with allergic diseases; and (III) without filarial infection and without allergic diseases. The prick test and specific IgE tests for aeroallergens were performed using five antigens. Peripheral eosinophils and total IgE were also evaluated. IL-4 and IL-5 were determined using whole-blood culture stimulated by three antigens. RESULTS: Eosinophilia and elevated levels of total IgE (>/ = 400IU/dl) were observed in all groups. The prick test was positive in 56.6% of the cases. Group I presented hypersensitive responses similar to the allergic disease groups. In the whole-blood culture stimulated by Dermatophagoides pteronyssinus, average IL-4 production did not differ significantly among the groups, but IL5 production resulting from stimulation was greater in the allergic disease groups (p < 0.05). CONCLUSIONS: The allergic response pattern in group with filarial infection was similar to that of the groups with and without allergic diseases, but the response to IL-5 in the culture stimulated by D. pteronyssinus was an exclusive characteristic of the allergic group.
Akita, S., et al. (2018). “Vectra 3D imaging for suprapubic lymphedema and volume change of the lower abdomen associated with lower extremity lymphedema.” Plast Reconstr Surg. [EPub Jan 18]
Bae, J. S., et al. (2018). “Evaluation of lymphedema in upper extremities by MR lymphangiography: Comparison with lymphoscintigraphy.” Magn Reson Imaging 49: 63–70.
Bezerra, M. L. S., et al. (2017). “Pseudotumor Cerebri and glymphatic dysfunction.” Front Neurol 8: 734.
In contrast to virtually all organ systems of the body, the central nervous system was until recently believed to be devoid of a lymphatic system. The demonstration of a complex system of paravascular channels formed by the endfeet of astroglial cells ultimately draining into the venous sinuses has radically changed this idea. The system is subsidized by the recirculation of cerebrospinal fluid (CSF) through the brain parenchyma along paravascular spaces (PVSs) and by exchanges with the interstitial fluid (IF). Aquaporin-4 channels are the chief transporters of water through these compartments. This article hypothesizes that glymphatic dysfunction is a major pathogenetic mechanism underpinning idiopathic intracranial hypertension (IIH). The rationale for the hypothesis springs from MRI studies, which have shown many signs related to IIH without evidence of overproduction of CSF. We propose that diffuse retention of IF is a direct consequence of an imbalance of glymphatic flow. This imbalance, in turn, may result from an augmented flow from the arterial PVS into the IF, by impaired outflow of the IF into the paravenous spaces, or both. Our hypothesis is supported by the facts that (i) visual loss, one of the main complications of IIH, is secondary to the impaired drainage of the optic nerve, a nerve richly surrounded by water channels and with a long extracranial course in its meningeal sheath; (ii) there is a high association between IIH and obesity, a condition related to paravascular inflammation and lymphatic disturbance, and (iii) glymphatic dysfunction has been related to the deposition of beta-amyloid in Alzheimer's disease. We conclude that the concept of glymphatic dysfunction provides a new perspective for understanding the pathophysiology of IIH; it may likewise entice the development of novel therapeutic approaches aiming at enhancing the flow between the CSF, the glymphatic system, and the dural sinuses.
Bouta, E. M., et al. (2018). “Lymphatic function measurements influenced by contrast agent volume and body position.” JCI Insight 3(2).
Several imaging modalities have been used to assess lymphatic function, including fluorescence microscopy, near-infrared fluorescence (NIRF) imaging, and Doppler optical coherence tomography (DOCT). They vary in how the mouse is positioned, the invasiveness of the experimental setup, and the volume of contrast agent injected. Here, we present how each of these experimental parameters affects functional measurements of collecting lymphatic vessels. First, fluorescence microscopy showed that supine mice have a statistically lower contraction frequency compared with mice sitting upright. To assess the effect of different injection volumes on these endpoints, mice were injected with 4, 10, or 20 mul of dye. The lowest frequencies were observed after 20-mul injections. Interestingly, lymph-flow DOCT revealed that although there was lower contraction frequency in mice injected with 20 mul versus 4 mul, mice showed a higher volumetric flow with a 20-mul injection. This indicates that contraction frequency alone is not sufficient to understand lymphatic transport. Finally, NIRF revealed that removing the skin reduced contraction frequency. Therefore, this study reveals how sensitive these techniques are to mouse position, removal of skin, and dye volume. Care should be taken when comparing results obtained under different experimental conditions.
Burke, E. and S. A. Datar (2018). “Lymphatic dysfunction in critical illness.” Curr Opin Pediatr. [EPub March 13]
PURPOSE OF REVIEW: The essential role of the lymphatic system in fluid homeostasis, nutrient transport, and immune trafficking is well recognized; however, there is limited understanding of the mechanisms that regulate lymphatic function, particularly in the setting of critical illness. The lymphatics likely affect disease severity and progression in every condition, from severe systemic inflammatory states to respiratory failure. Here, we review structural and functional disorders of the lymphatic system, both congenital and acquired, as they relate to care of the pediatric patient in the intensive care setting, including novel areas of research into medical and procedural therapeutic interventions. RECENT FINDINGS: The mainstay of current therapies for congenital and acquired lymphatic abnormalities has involved nonspecific medical management or surgical procedures to obstruct or divert lymphatic flow. With the development of dynamic contrast-enhanced magnetic resonance lymphangiography, image-directed percutaneous intervention may largely replace surgery. Because of new insights into the mechanisms that regulate lymphatic biology, pharmacologic inhibitors of mTOR and leukotriene B4 signaling are each in Phase II clinical trials to treat abnormal lymphatic structure and function, respectively. SUMMARY: As our understanding of normal lymphatic biology continues to advance, we will be able to develop novel strategies to support and augment lymphatic function during critical illness and through convalescence.
Chachaj, A., et al. (2018). “Role of the lymphatic system in the pathogenesis of hypertension in humans.” Lymphat Res Biol. [EPub Jan 18]
BACKGROUND: Recent studies, mainly on animal models, have suggested that negatively charged glycosaminoglycans, macrophages, and lymph vessels in the skin interstitium may serve as extrarenal control of sodium balance and blood pressure. The aim of the study was to prove the hypothesis that skin interstitium has a role in the pathogenesis of hypertension in humans. METHODS AND RESULTS: We have examined skin biopsies in 91 patients from the department of surgery who had elective surgery with abdominal skin incision: 43 were hypertensive, 14 had resistant hypertension, and 34 with normal blood pressure as control group (median patients' age in these groups estimated accordingly 64 vs. 64 vs. 61.5; p > 0.05). We have studied (1) the content of Na(+), water, accumulation of macrophages (CD68), and density of lymphatic vessels (D2-40) and blood vessels (CD31) in the specimens of abdominal skin taken at the time of surgery and (2) plasma NT-proANP, vascular endothelial growth factor (VEGF)-C, and VEGF-D concentrations. The study groups differed in skin expression of CD68 (control vs. hypertension vs. resistant hypertension groups were accordingly: 3.33 vs. 4.00 vs. 8.33; p = 0.005) and in serum concentration of VEGF-C (5792 vs. 4348 vs. 3974 pg/mL; p = 0.026). Differences among groups in plasma NT-proANP levels were close to statistical significance (p = 0.056). CONCLUSIONS: Our results confirm that skin interstitium may be involved in the pathogenesis of essential hypertension in humans. Lower levels of VEGF-C in hypertensive groups suggest that impairment of lymphangiogenesis and protective function of the skin lymphatic system may play a role in the pathogenesis of hypertension.
Cuadrado, G. A., et al. (2018). “Lymph drainage of the upper limb and mammary region to the axilla: anatomical study in stillborns.” Breast Cancer Res Treat. [EPub Jan 29]
PURPOSE: We studied the lymphatic drainage of the upper limb and mammary region directing to the axilla to investigate whether independent pathways can be observed or whether anastomoses and shared drainage occur between them. This analysis aimed to assess the safety of axillary reverse mapping (ARM) in breast cancer treatment and to understand the development of lymphedema after sentinel lymph node biopsy (SLNB) alone. METHODS: Seven unfixed stillborn fetuses were injected with a modified Gerota mass in the peri-areolar area, palm and dorsum of the hands, formalin fixed, and then submerged in 10% hydrogen peroxide solution. Microsurgical dissection was then performed on the subcutaneous cellular tissue of the upper limb, axillary region, and anterior thorax to expose the lymphatic vessels and lymph nodes. RESULTS: The dye injected into the upper limb reached either the lateral axillary group, known to be exclusively responsible for upper limb drainage, or the anterior group, which is typically related to breast drainage. There was great proximity among the pathways and lymph nodes. Communicating lymphatic vessels among these groups of lymph nodes were also found in all studied cases. DISCUSSION: Lymphedema remains a challenging morbidity in breast cancer treatment. ARM and SLNB aim to avoid unnecessary damage to the lymphatic drainage of the upper limb. However, our anatomical study suggests that ARM may have potential oncological risks because preserved lymph nodes may harbor malignant cells due their proximity, overlapping drainage pathways, and connecting lymph vessels among lymph nodes.
d'Udekem, Y. and M. de Leval (2018). “The elusive and ungrateful lymphatic circulation may be a key determinant of Fontan failure.” J Thorac Cardiovasc Surg. [EPub Feb 1]
Dave, R. S., et al. (2018). “Functional meningeal lymphatics and cerebrospinal fluid outflow.” J Neuroimmune Pharmacol. [EPub Febb 20]
Functional meningeal lymphatic system plays a crucial role in outflow of cerebrospinal fluid. Metabolites and neurotoxins in the cerebrospinal fluid may be excreted via this system and accumulate in the cervical lymph nodes. In this letter, we highlighted the role of functional meningeal lymphatics and cerebrospinal fluid outflow.
Fastre, E., et al. (2018). “Splice-site mutations in VEGFC cause loss of function and Nonne-Milroy-like primary lymphedema.” Clin Genet. [EPub March 15]
Gillaspie, E. A., et al. (2018). “Surgical management of chyloptysis.” Ann Thorac Surg 105(2): e79-e81.
Chyloptysis is a rare clinical presentation. Diagnosis is challenging and requires recognition of milky-sputum or bronchial casts. We describe a case of chyloptysis secondary to thoracic lymphangiectasia that necessitated surgical ligation of the main thoracic duct and accessory branches. The patient had no postoperative complications, and at 6-month follow-up remained symptom-free. A paucity of literature describes the management of chyloptysis. We review diagnosis, treatment considerations and operative principles.
Hara, H., et al. (2018). “Therapeutic lymphangiography for traumatic chylothorax.” J Vasc Surg Venous Lymphat Disord 6(2): 237–240.
Chylothorax is a challenging disease. We present a case of traumatic chylothorax that was successfully treated using lymphangiography through intranodal injection of contrast agent. A 17-year-old girl had chylothorax. It did not improve despite medical treatment. We performed lymphangiography through intranodal injection of an oil contrast agent (Lipiodol). The amount of chylothorax was reduced from 1000 to 120 mL/d, and we could remove the thoracotomy tube. Thereafter, although she had a small amount of pleural effusion, she has not demonstrated aggravation for 19 months. Lymphangiography with oil contrast agent can be one of the options to treat chylothorax.
Hase, I., et al. (2018). “Hyperplasia of lymphoid follicles and lymphangiectasia in the parietal pleura in bucillamine-induced yellow nail syndrome.” Intern Med. [EPub Feb 9]
Yellow nail syndrome (YNS) pleurisy is often difficult to control, and pathological examinations have rarely been reported. We herein report a case of bucillamine-induced YNS in which histopathology of the parietal pleura revealed hyperplasia of the lymphoid follicles and lymphangiectasia. Even after the discontinuation of bucillamine, the pleurisy and lymphedema showed no change. Based on the histopathological findings showing similarity to rheumatoid pleurisy, we administered corticosteroid treatments, and both the pleurisy and lymphedema improved. The findings in the present case suggest that, in bucillamine-induced YNS, pleurisy may be related to inflammation caused by rheumatoid arthritis in addition to abnormalities in lymphatic vessels.
Hvidsten, S., et al. (2018). “A scintigraphic method for quantitation of lymphatic function in arm lymphedema.” Lymphat Res Biol. [EPub Jan 18]
BACKGROUND: Lymphoscintigraphy is commonly used to assess breast cancer-related lymphedema. However, a reliable quantitative method that clearly distinguishes normal lymphatic function from lymphedema is desired. We propose a quantitative method based upon the physiological mean transit time (MTT) measure of lymph fluid passing through the arm. METHODS AND RESULTS: Eleven patients, aged 34-68 years, with unilateral arm lymphedema following breast cancer treatment underwent simultaneous bilateral lymphoscintigraphy using intradermal injection of (99m)Tc-labeled human serum albumin (HSA). Imaging was performed at 30-45 minute intervals for 5 hours. Time activity curves from each injection site and each arm region were recorded. The input into the arm region was obtained as the (minus) time derivative of the injection site activity curve. In the proposed model the arm activity curve was considered to arise from the convolution of the retention function and the input function. The retention function was obtained by fitting the calculated arm activity curve to the measured arm activity curve. The MTT of activity passing through the arm was calculated as the time integral of the resulting retention function. All measured time activity curves were well described by the model. The MTT of the lymphedema arm (mean 60.1 minutes, range 22-105 minutes) was markedly different from that of the contralateral normal arm (mean 5.4 minutes, range 1.2-8.7 minutes), p < 0.0001. CONCLUSION: The proposed model showed great similarity with measured time activity curves and was capable of quantitatively distinguishing lymphatic function of the lymphedema arm from that of the normal arm in terms of calculated MTT.
Jones, D., et al. (2018). “Methicillin-resistant Staphylococcus aureus causes sustained collecting lymphatic vessel dysfunction.” Sci Transl Med 10(424).
Methicillin-resistant Staphylococcus aureus (MRSA) is a major cause of morbidity and mortality worldwide and is a frequent cause of skin and soft tissue infections (SSTIs). Lymphedema-fluid accumulation in tissue caused by impaired lymphatic vessel function-is a strong risk factor for SSTIs. SSTIs also frequently recur in patients and sometimes lead to acquired lymphedema. However, the mechanism of how SSTIs can be both the consequence and the cause of lymphatic vessel dysfunction is not known. Intravital imaging in mice revealed an acute reduction in both lymphatic vessel contractility and lymph flow after localized MRSA infection. Moreover, chronic lymphatic impairment is observed long after MRSA is cleared and inflammation is resolved. Associated with decreased collecting lymphatic vessel function was the loss and disorganization of lymphatic muscle cells (LMCs), which are critical for lymphatic contraction. In vitro, incubation with MRSA-conditioned supernatant led to LMC death. Proteomic analysis identified several accessory gene regulator (agr)-controlled MRSA exotoxins that contribute to LMC death. Infection with agr mutant MRSA resulted in sustained lymphatic function compared to animals infected with wild-type MRSA. Our findings suggest that agr is a promising target to preserve lymphatic vessel function and promote immunity during SSTIs.
Kenworthy, E. O., et al. (2018). “Double vascularized omentum lymphatic transplant (VOLT) for the treatment of lymphedema.” J Surg Oncol. [EPub March 8]
BACKGROUND AND OBJECTIVES: Orthotopic vascularized lymph node transplant has been successfully used to treat lymphedema. A second, heterotopic lymph node transplant in the distal extremity may provide further improvement. The vascularized omentum lymphatic transplant (VOLT) provides adequate tissue for two simultaneous flap transfers to one limb. The purpose of this study was to review our experience with this technique. METHODS: We conducted a retrospective study of patients who underwent VOLT, with a subgroup analysis of patients who underwent double VOLT. Technical aspects of the procedure, complications, and early outcomes were reviewed. RESULTS: From May 2015 to August 2017, 54 VOLTs were performed in 38 patients, of whom 16 received double VOLT. Among patients in the double VOLT group with postoperative imaging at 1 year, uptake into the transplanted omentum was seen in three of six (50%) patients on lymphoscintigraphy and in one of five (20%) patients on indocyanine green lymphangiography. One patient (3.1%) in the double VOLT group required a return to the operating room. There were no donor site complications in the double VOLT group. The overall complication rate was 15.8%. CONCLUSIONS: Double VOLT to the mid-level and proximal extremity is a safe and viable option.
Liu, D., et al. (2018). “Unilateral pedal lymphangiography plus computed tomography angiography for location of persistent idiopathic chyle leakage not detectable by ordinary contrast computed tomography.” BMC Urol 18(1): 9.
BACKGROUND: To identify the value of unilateral pedal lymphangiography (LPG) plus computed tomography angiography (CTA) in accurate depiction of persistent idiopathic chyluria undetectable by ordinary contrast CT. METHODS: Eighteen patients 44-63 years of age with persistent idiopathic chyluria who failed conservative management were included. Ordinary CT had not revealed a chyle leak. Cystoscopy, unilateral LPG, and post-LPG CT angiography (CTA) were sequentially performed. Ligation and stripping of the perirenal lymphatics were subsequently performed guided by lymphangiography and CTA. RESULTS: LPG and post-LPG CTA detected 17 unilateral and one bilateral chyle leaks in the 18 patients, with clear images of the communication of lymphatic vessels and the renal collecting or vascular system. The success rate was significantly better than cystoscopy (100% vs 50.0%, P = 0.005) or LPG alone (100% vs. 72.2%, P = 0.016). Chyluria resolved after surgery in all patients; no relapses were found. CONCLUSIONS: LPG plus post-LPG CTA accurately characterized perirenal lymphangiectasia that was not demonstrated by routine contrast-enhanced CT or not suitable for magnetic resonance imaging. Despite of its invasiveness, this method is a good diagnostic alternative to LPG in patients with persistent chyluria requiring surgery.
Muller, M., et al. (2018). “Manual lymphatic drainage and quality of life in patients with lymphoedema and mixed oedema: a systematic review of randomised controlled trials.” Qual Life Res. [EPub Febb 5]
PURPOSE: To assess the impact of manual lymphatic drainage (MLD) on the health-related quality of life (HRQoL) of adults with lymphoedema or mixed oedema, through a systematic review of randomised controlled trials (RCTs). METHODS: MEDLINE, EMBASE, PsycINFO, CENTRAL, the Cochrane Database of Systematic Reviews and ClinicalTrials.gov were searched to identify RCTs evaluating HRQoL after a MLD intervention compared to non-MLD interventions (PROSPERO 2016:CRD42016042255). We extracted the effect of the interventions on the HRQoL (primary outcome) as well as data on volume and functional changes, and adverse events when available (secondary outcomes). RESULTS: Eight studies were eligible. The studies were heterogeneous in the aetiology of oedema, schemes of MLD applied, additional treatments offered with MLD, length of follow-up, instruments used to assess HRQoL and interventions offered to the control group. Five studies included patients with breast cancer-related arm lymphoedema; one study reported increased HRQoL among patients randomised to the MLD group. The two RCTs that involved patients with leg mixed oedema due to chronic venous insufficiency did not find between-group differences in the overall HRQoL. One trial included patients with hand oedema from systemic sclerosis and showed higher HRQoL in the group that received MLD. No studies reported reductions in HRQoL, or severe adverse events after MLD. The small numbers of patients analysed in all studies may have resulted in lack of power to detect between-group differences in HRQoL. CONCLUSIONS: The effect of MLD on the HRQoL of patients with chronic oedema is unclear.
Pereira de Godoy, L. M., et al. (2018). “Lymphatic drainage of legs reduces edema of the arms in children with lymphedema.” Case Rep Pediatr 2018: 6038907.
Objective: The aim of the present study is to report on the reduction of edema of lymphedematous arms just by treating the lower limbs. Methods: A 16-year-old girl reported that she has started having right lower limb edema at the age of three. At age 13, she performed a lymphoscintigraphy that confirmed the diagnosis of primary lymphedema of the four limbs. Recently she sought treatment at the Clinica Godoy in Sao Jose do Rio Preto where she was submitted to intensive treatment for eight hours per day for five days using manual (Godoy & Godoy technique) and mechanical lymphatic therapy (RA Godoy((R))) of the lower limbs, cervical lymphatic therapy (cervical stimulation), and the continuous use of a grosgrain stocking. Results: At the end of treatment, reductions in the sizes of both arms and legs were noted even without the use of any specific therapy for the arms. After four years, the size of the arms was normal. Conclusion: Treatment of lymphedema of the legs has systemic repercussions that may lead to the reduction in swelling of other untreated regions of the body.
Rehal, S., et al. (2018). “Acute small intestinal inflammation results in persistent lymphatic alterations.” Am J Physiol Gastrointest Liver Physiol 314(3): G408-G417.
Inflammatory bowel disease (IBD) has a complex pathophysiology with limited treatments. Structural and functional changes in the intestinal lymphatic system have been associated with the disease, with increased risk of IBD occurrence linked to a history of acute intestinal injury. To examine the potential role of the lymphatic system in inflammation recurrence, we evaluated morphological and functional changes in mouse mucosal and mesenteric lymphatic vessels, and within the mesenteric lymph nodes during acute ileitis caused by a 7-day treatment with dextran sodium sulfate (DSS). We monitored whether the changes persisted during a 14-day recovery period and determined their potential consequences on dendritic cell (DC) trafficking between the mucosa and lymphoid tissues. DSS administration was associated with marked lymphatic abnormalities and dysfunctions exemplified by lymphangiectasia and lymphangiogenesis in the ileal mucosa and mesentery, increased mesenteric lymphatic vessel leakage, and lymphadenopathy. Lymphangiogenesis and lymphadenopathy were still evident after recovery from intestinal inflammation and correlated with higher numbers of DCs in mucosal and lymphatic tissues. Specifically, a deficit in CD103(+) DCs observed during acute DSS in the lamina propria was reversed and further enhanced during recovery. We concluded that an acute intestinal insult caused alterations of the mesenteric lymphatic system, including lymphangiogenesis, which persisted after resolution of inflammation. These morphological and functional changes could compromise DC function and movement, increasing susceptibility to further gastrointestinal disease. Elucidation of the changes in mesenteric and intestinal lymphatic function should offer key insights for new therapeutic strategies in gastrointestinal disorders such as IBD. NEW & NOTEWORTHY Lymphatic integrity plays a critical role in small intestinal homeostasis. Acute intestinal insult in a mouse model of acute ileitis causes morphological and functional changes in mesenteric and intestinal lymphatic vessels. While some of the changes significantly regressed during inflammation resolution, others persisted, including lymphangiogenesis and altered dendritic cell function and movement, potentially increasing susceptibility to the recurrence of gastrointestinal inflammation.
Romano, V., et al. (2018). “Detection and imaging of lymphatic and other vessels in corneal neovascular complexes.” Cornea 37(4): e22-e23.
Schaverien, M. V., et al. (2018). “Vascularized jejunal mesenteric lymph node transfer for lymphedema: A novel approach.” Plast Reconstr Surg 141(3): 468e-469e.
Shirotsuki, R., et al. (2018). “Novel thoracoscopic navigation surgery for neonatal chylothorax using indocyanine-green fluorescent lymphography.” J Pediatr Surg. [EPub Feb 1]
BACKGROUND: Postoperative chylothorax after surgery for esophageal atresia/tracheoesophageal fistula (TEF) is a rare but serious complication, especially in neonates. This study aimed to identify the thoracic duct and ligate chylous leakage sites, using thoracoscopic navigation of an indocyanine-green (ICG)-based near-infrared (NIR) fluorescence imaging system. METHODS: From November 2014 to April 2017, thoracoscopic intraoperative ICG-NIR imaging was performed in 10 newborns (11 surgeries) with first TEF operation or with persistent postoperative chylothorax after TEF operation. NIR imaging was performed 1h after an inter-toe injection of ICG. Thoracoscopic ligations against the NIR-detected leakage sites were performed with sutures. RESULTS: The thoracic duct or lymphatic leakage was directly visualized in each patient. In 8 surgeries with first thoracoscopic TEF operation, one case had suspected minor chylous leakage without postoperative chylothorax. Another case with no chylous leakage at the first operation resulted in chylothorax at postoperative day 11. In three neonates with postoperative chylothorax, leakage points were detected near the ablation site of the azygos vein during the first operation. These points were properly ligated, and postoperative chylous leakage ceased with no adverse events. CONCLUSIONS: Thoracoscopic ICG-NIR imaging encourages the repair of refractory chylothorax and seems reliable. LEVEL OF EVIDENCE: IV.
Srinivasa, R. N., et al. (2017). “Endolymphatic balloon-occluded retrograde abdominal lymphangiography (BORAL) and embolization (BORALE) for the diagnosis and treatment of chylous ascites: Approach, technical success, and clinical outcomes.” Ann Vasc Surg. [EPub Dec 5]
BACKGROUND: To describe endolymphatic balloon-occluded retrograde abdominal lymphangiography (BORAL) and embolization (BORALE) for diagnosis and treatment of chylous ascites in patients with previously unidentifiable leakage site or failed lymphatic embolization. METHODS: Two (66%) men and 1 (33%) woman with mean age of 52 years (range: 14-79 years) presented with chylous ascites and underwent BORAL or BORALE between March 2016 and February 2017. Patients presented with chylous ascites (n = 3) and with renal cell carcinoma after left nephrectomy and lymph node dissection (n = 1), metastatic Merkel cell carcinoma after left nephrectomy and adrenalectomy (n = 1), and heart transplantation after failed Fontan procedure (n = 1). Pelvic lymphangiography technical successes, complications, radiation dose, contrast volume, clinical response, and follow-up were recorded. RESULTS: Pelvic lymphangiography and BORAL were technically successful in 3 (100%) patients. BORALE was attempted in 2 (66%) patients and was technically successful in both patients (100%). No minor or major complications occurred. Mean radiation dose was 1,037 mGy (range: 391-2,264 mGy). Mean contrast was 83 mL (range: 25-150 mL). Mean blood loss was 15 mL (range: 5-30 mL). Chylous ascites resolved in all 3 (100%) patients. CONCLUSIONS: BORAL and BORALE provide a rational and effective approach for the diagnosis and treatment of patients with chylous ascites and previously unidentifiable leakage site or failed lymphatic embolization.
Suehiro, K., et al. (2018). “Venous hemodynamics assessed with air plethysmography in legs with lymphedema.” Vasc Med: 1358863X17745372.
This study was conducted to identify specific abnormalities using the results from air plethysmography in legs with lymphedema. A routine air plethysmography exercise protocol was performed in 31 patients with unilateral leg lymphedema, and the results were compared with those of 53 patients with unilateral great saphenous vein reflux and 15 normal subjects. The venous filling index in legs with lymphedema (2.1 +/- 1.2 mL/sec) was smaller than in legs with great saphenous vein reflux (6.4 +/- 4.1 mL/sec, p < 0.05), but was not different from that in normal legs (1.9 +/- 1.2 mL/sec). The ejection fraction was similar in all groups. The residual volume fraction in legs with lymphedema (35 +/- 32%) was larger than that in normal subjects (13 +/- 23%, p < 0.05), but was not significantly different from that in the contralateral leg of the lymphedema patients (32 +/- 27%). In conclusion, we found no specific air plethysmography findings in uncomplicated lymphedema.
Taoka, T. and S. Naganawa (2018). “Gadolinium-based contrast media, cerebrospinal fluid and the glymphatic system: Possible mechanisms for the deposition of gadolinium in the brain.” Magn Reson Med Sci. [EPub Jan 25]
After Kanda's first report in 2014 on gadolinium (Gd) deposition in brain tissue, a considerable number of studies have investigated the explanation for the observation. Gd deposition in brain tissue after repeated administration of gadolinium-based contrast medium (GBCM) has been histologically proven, and chelate stability has been shown to affect the deposition. However, the mechanism for this deposition has not been fully elucidated. Recently, a hypothesis was introduced that involves the 'glymphatic system', which is a coined word that combines 'gl' for glia cell and 'lymphatic' system. According to this hypothesis, the perivascular space functions as a conduit for cerebrospinal fluid to flow into the brain parenchyma. The perivascular space around the arteries allows cerebrospinal fluid to enter the interstitial space of the brain tissue through water channels controlled by aquaporin 4. The cerebrospinal fluid entering the interstitial space clears waste proteins from the tissue. It then flows into the perivascular space around the vein and is discharged outside the brain. In addition to the hypothesis regarding the glymphatic system, some reports have described that after GBCM administration, some of the GBCM distributes through systemic blood circulation and remains in other compartments including the cerebrospinal fluid. It is thought that the GBCM distributed into the cerebrospinal fluid cavity via the glymphatic system may remain in brain tissue for a longer duration compared to the GBCM in systemic circulation. Glymphatic system may of course act as a clearance system for GBCM from brain tissue. Based on these findings, the mechanism for Gd deposition in the brain will be discussed in this review. The authors speculate that the glymphatic system may be the major contributory factor to the deposition and clearance of gadolinium in brain tissue.
Tummalapalli, S. R., et al. (2018). “Discovery of a stress-activated protein kinase inhibitor for lymphatic filariasis.” ACS Med Chem Lett 9(3): 210–214.
Lymphatic filariasis infects over 120 million people worldwide and can lead to significant disfigurement and disease. Resistance is emerging with current treatments, and these therapies have dose limiting adverse events; consequently new targets are needed. One approach to achieve this goal is inhibition of parasitic protein kinases involved in circumventing host defense mechanisms. This report describes structure-activity relationships leading to the identification of a potent, orally bioavailable stress activated protein kinase inhibitor that may be used to investigate this hypothesis.
Turpin, S. and R. Lambert (2018). “Lymphoscintigraphy of chylous anomalies: chylothorax, chyloperitoneum, chyluria and lymphangiomatosis. Fifteen year experience in a pediatric setting and review of the literature.” J Nucl Med Technol. [EPub Feb 2]
Objective: In the pediatric setting, lymphoscintigraphy is mostly used for the evaluation of lymphedema. Only a few cases of chylous anomalies and lymphatic malformations imaged with lymphoscintigraphy, have been reported in the literature. The aim of this study was to review the use of lymphoscintigraphy in those pathologies. Methods: All lymphoscintigraphies obtained between 2001 and 2017 in our hospital for chylous anomalies were retrospectively reviewed. Results were correlated to clinical and radiological findings. Lymphoscintigraphy consisted of sequential imaging after injection of 100-250 muci (99m)Tc-filtered sulfur colloid at the level of the feet and/or hands. Results: Twenty five studies were performed in 21 patients. Fourteen studies were obtained for the evaluation of chylothorax. Eleven were performed for chyloperitoneum, chyluria, chylopericardium, exsudative enteropathy or lymphangiomatosis. Ten studies were positive for lymphatic leak, 1 was dubious. After correlation with radiological findings and follow-up, there were seven true negative and five false negative (previous (67)Ga interfering activity in 1, injection on the hands only in 3, low lipid diet in 1). One study became positive after injecting on the feet and another one after switching to a high lipid diet. Conclusion: Lymphoscintigraphy is a useful tool to image lymphatic anomalies in children. To optimize results, it is suggested to inject the 4 extremities, to have the patient under a high lipid diet, to withhold octreotide and use single photon emission tomography with computed tomography (SPECT/CT).
Yang, J. C., et al. (2018). “Targeting reflux-free veins with a vein visualizer to identify the ideal recipient vein preoperatively for optimal lymphaticovenous anastomosis in treating lymphedema.” Plast Reconstr Surg 141(3): 793–797.
Lymphaticovenous anastomosis is one of the main surgical treatments nowadays for alleviating lymphedema. A successful lymphaticovenous anastomosis relies on being able to identify “functional” lymphatic collecting vessels that are still capable of transporting lymph, and a nearby vein that is, ideally, reflux-free. This is a retrospective study. A total of 28 lymphedema patients were enrolled from October of 2016 to March of 2017 in Kaohsiung Chang Gung Hospital, Kaohsiung, Taiwan. A noninvasive vein visualizer was used to preselect reflux-free veins for lymphaticovenous anastomosis from five female patients. As a control, the total number of veins used for lymphaticovenous anastomoses without the use of a vein visualizer from 23 consecutive lymphedema patients was also recorded and compared. In the experimental group, a total of 12 of 13 veins (92 percent sensitivity) preselected by using the VeinViewer were confirmed to be reflux-free intraoperatively during lymphaticovenous anastomosis. In the control group, 21 of 56 veins (37.5 percent sensitivity) showed no venous reflux. Statistical analysis with the chi-square test showed a value of p < 0.001 (number needed to treat = 2.706). The odds of identifying reflux-free veins can be increased significantly with the use of a vein visualizer. CLINICAL QUESTION/LEVEL OF EVIDENCE: Diagnostic, II.
Oncology
Armani, G., et al. (2018). “Blood and lymphatic vessels contribute to the impact of the immune microenvironment on clinical outcome in non-small-cell lung cancer.” Eur J Cardiothorac Surg. [EPub Jan 15]
OBJECTIVES: Lymphangiogenesis plays a critical role in the immune response, tumour progression and therapy effectiveness. The aim of this study was to determine whether the interplay between the lymphatic and the blood microvasculature, tumour-infiltrating lymphocytes and the programmed death 1 (PD-1)/programmed death ligand 1 (PD-L1) immune checkpoint constitutes an immune microenvironment affecting the clinical outcome of patients with non-small-cell lung cancer. METHODS: Samples from 50 squamous cell carcinomas and 42 adenocarcinomas were subjected to immunofluorescence to detect blood and lymphatic vessels. CD3pos, CD8pos and PD-1pos tumour-infiltrating lymphocytes and tumour PD-L1 expression were assessed by immunohistochemical analysis. RESULTS: Quantification of vascular structures documented a peak of lymphatics at the invasive margin together with a decreasing gradient of blood and lymphatic vessels from the peritumour area throughout the neoplastic core. Nodal involvement and pathological stage were strongly associated with vascularization, and an increased density of vessels was detected in samples with a higher incidence of tumour-infiltrating lymphocytes and a lower expression of PD-L1. Patients with a high PD-L1 to PD-1 ratio and vascular rarefaction had a gain of 10 months in overall survival compared to those with a low ratio and prominent vascularity. CONCLUSIONS: Microvessels are an essential component of the cancer immune microenvironment. The clinical impact of the PD-1/PD-L1-based immune contexture may be implemented by the assessment of microvascular density to potentially identify patients with non-small-cell lung cancer who could benefit from immunotherapy and antiangiogenic treatment.
Ernst, B. P., et al. (2018). “Association of eIF4E and SPARC expression with lymphangiogenesis and lymph node metastasis in hypopharyngeal cancer.” Anticancer Res 38(2): 699–706.
BACKGROUND/AIM: Head and neck squamous cell carcinomas (HNSCC) are characterized by aggressiveness, early recurrence and lymph node metastasis. Therefore, there is an urgent need to identify new biomarkers and drug targets. MATERIALS AND METHODS: Neck dissection specimens from 11 patients diagnosed with hypopharyngeal cancer were analyzed for their lymphatic vessel density (LVD) by lymphatic vessel endothelial hyaluronan receptor 1 (LYVE-1) immunostaining, expression of eukaryotic initiation factor 4E (eIF4E) and levels of secreted protein acidic and rich in cysteine (SPARC) using immunoblot analysis. RESULTS: Compared to lymph node biopsies of healthy controIs, LVD was significantly increased in metastatic lymph nodes as well as in advanced primary tumors. Overexpression of eIF4E and SPARC was demonstrated in all hypopharyngeal cancer specimens. Notably, we observed that increased LVD significantly correlated with the expression of eIF4E as well as SPARC levels. CONCLUSION: eIF4E- and SPARC-associated signaling pathways may be associated with lymphangiogenesis and could be exploited to counteract the spread of hypopharyngeal cancer cells.
Garcia-Caballero, M., et al. (2017). “Targeting VEGFR-3/-2 signaling pathways with AD0157: a potential strategy against tumor-associated lymphangiogenesis and lymphatic metastases.” J Hematol Oncol 10(1): 122.
BACKGROUND: Lymphatic metastasis is one of the leading causes of death in patients with different types of cancer and is the main prognostic factor for the disease survival. The formation of new lymphatic vessels (lymphangiogenesis) in primary tumors facilitates tumor cell dissemination to regional lymph nodes and correlates with distant metastases. Lymphangiogenesis has thus emerged as a suitable therapeutic target to block metastases, but no anti-lymphangiogenic compounds have been approved for clinical use to date. Therefore, new or improved therapies blocking lymphatic metastases are urgently required. METHODS: We established murine breast tumors to assess the effect of AD0157 on tumor growth, lymphangiogenesis, and lymphatic dissemination. Then, a battery of in vivo (mouse corneal neovascularization and ear sponges), ex vivo (mouse lymphatic rings and rat mesentery explants), and in vitro (proliferation, tubulogenesis, wound-healing, Boyden chambers, and spheroids) assays was used to give insight into the lymphangiogenic steps affected by AD0157. Finally, we investigated the molecular pathways controlled by this drug. RESULTS: AD0157 was found to inhibit the growth of human breast cancer xenografts in mice, to strongly reduce tumor-associated lymphangiogenesis and to block metastatic dissemination to both lymph nodes and distant organs. The high anti-lymphangiogenic potency of AD0157 was further supported by its inhibitory activity at low micromolar range in two in vivo pathological models and in two ex vivo assays. In addition, AD0157 inhibited lymphatic endothelial cell proliferation, migration and invasion, cellular sprouting, and tube formation. Mechanistically, this compound induced apoptosis in lymphatic endothelial cells and decreased VEGFR-3/-2, ERK1/2, and Akt phosphorylations. CONCLUSIONS: These findings demonstrate the suitability of AD0157 to suppress tumor-associated lymphangiogenesis. Beyond discovering a new potent anti-lymphangiogenic drug that is worth considering in future clinical settings, our study supports the interest of designing anti-lymphangiogenic therapies to avoid distant metastatic processes.
Grarup, K. R., et al. (2018). “The Danish version of Lymphoedema Functioning, Disability and Health Questionnaire (Lymph-ICF) for breast cancer survivors: Translation and cultural adaptation followed by validity and reliability testing.” Physiother Theory Pract: 1–14.
PURPOSE: To translate and culturally adapt the Lymphoedema Functioning, Disability and Health Questionnaire (Lymph-ICF) for breast cancer survivors with arm lymphedema into Danish and examine its content validity and reliability. METHODS: (1) Translation and cultural adaptation was performed in 10 steps following international guidelines (International Society for Pharmacoeconomics and Outcome Research); (2) cognitive interviewing (step 7) was conducted in 15 women with breast cancer related arm lymphedema to explore understandability, interpretation, and cultural relevance; (3) after adjustments, content validity (N = 52) was explored by interviews; and (4) reliability (N = 50) examined by intraclass correlation coefficients (ICC) statistics and Cronbach alpha analysis. RESULTS: Cognitive interviewing lead to an adapted and improved version of the translated questionnaire. Content validity was supported. Internal consistency (alpha) for all questions was .98 and ranged for the different domains between 0.92 and 0.97. Test-retest reliability for the total score was highly satisfactory, ICC = 0.95, standard error of measurement (SEM) = 4.5 and smallest detectable change = 12.5. ICC values for the domains ranged from 0.84 to 0.94. SEM values differed for the domains, 6.4 (physical function), 5.7 (mobility activities), 7.09 (life and social activities), 9.1 (mental functions), and 10.2 (household activities). CONCLUSION: The translated and adjusted Lymph-ICF DK (Denmark) is reliable and valid, allowing for assessing self-reported impairments in function, activity limitations, and participation restrictions in Danish patients with breast cancer-related arm lymphedema.
Guo, R. L., et al. (2018). “The regulatory role of SLP-2 and mechanism on CCBE1 gene expression in rectal carcinoma and adjacent lymphatic tube tissues.” Eur Rev Med Pharmacol Sci 22(1): 87–94.
OBJECTIVE: The incidence of rectal carcinoma (RC) has been increasing recently, and becomes the second most common digestive tumors besides gastric cancer, with a rise in the incidence of RC in younger populations. The early diagnosis and treatment are thus critical for the improvement of survival rate and life quality of patients. Stomatin-like protein 2 (SLP-2) is a type of membrane factor, which is generally found highly expressed in various tumors. Collagen and calcium-binding EGF domain (CCBE1) belongs to lymphatic tube genesis factor. The regulatory role of SLP-2 gene on CCBE1 expression in RC tumor and adjacent lymphatic tube tissues, however, has not been studied. PATIENTS AND METHODS: 52 RC patients were recruited, and tumor and adjacent lymphatic tube tissues were collected. Real-time PCR, western blotting and immunohistochemistry (IHC) staining were used to analyze SLP-2 and CCBE1 expressions. Human lymphatic endothelial cells (LECs) were cultured in vitro and were assigned to control, scramble, and SLP-2 siRNA group. MTT assay was used to detect cell proliferation, while caspase 3 activity was detected. RESULTS: SLP-2 and CCBE1 levels were significantly elevated in tumor lymphatic tissues, compared to that in adjacent tissues. Statistically positive correlation between SLP-1 and CCBE2 was found (p < 0.05). The downregulation of SLP-2 by siRNA inhibited cell proliferation, elevated caspase3 activity, and decreased CCBE1 expression (p < 0.05 compared to control group). CONCLUSIONS: SLP-2 is up-regulated in RC lymphatic tissues, and is positively correlated with the level of CCBE1, which provides the academic the basis for the development of medicine targeting SLP-2 in the anti-rectal carcinoma therapy.
Hadizadeh, M., et al. (2018). “GJA4/Connexin 37 mutations correlate with secondary lymphedema following surgery in breast cancer patients.” Biomedicines 6(1).
Lymphedema is a condition resulting from mutations in various genes essential for lymphatic development and function, which leads to obstruction of the lymphatic system. Secondary lymphedema is a progressive and incurable condition, most often manifesting after surgery for breast cancer. Although its causation appears complex, various lines of evidence indicate that genetic predisposition may play a role. Previous studies show that mutations in connexin 47 are associated with secondary lymphedema. We have tested the hypothesis that connexin 37 gene mutations in humans are associated with secondary lymphedema following breast cancer surgery. A total of 2211 breast cancer patients were screened and tested for reference single nucleotide polymorphisms (SNPs) of the GJA4 gene (gap junction protein alpha 4 gene). The results presented in this paper indicate that two SNPs in the 3' UTR (the three prime untranslated region) of the GJA4 gene are associated with an increased risk of secondary lymphedema in patients undergoing breast cancer treatment. Our results provide evidence of a novel genetic biomarker for assessing the predisposition to secondary lymphedema in human breast cancer patients. Testing for the condition-associated alleles described here could assist and inform treatment and post-operative care plans of breast cancer patients, with potentially positive outcomes for the management of disease progression.
Hahamoff, M., et al. (2018). “A lymphedema surveillance program for breast cancer patients reveals the promise of surgical prevention.” J Surg Res. [EPub Febb 1]
BACKGROUND: Breast cancer-related lymphedema (BCRL) is one of the most significant survivorship issues in breast cancer management. Presently, there is no cure for BCRL. The single greatest risk factor for developing BCRL is an axillary lymph node dissection (ALND). Lymphatic Microsurgical Preventative Healing Approach (LYMPHA) is a surgical procedure to reduce the risk of lymphedema in patients undergoing an ALND. We present our single institution results after offering LYMPHA in the context of an established lymphedema surveillance program. MATERIALS AND METHODS: A retrospective review of our lymphedema surveillance program at the University of Florida was performed over a 2-year period (March 2014-March 2016). LYMPHA was offered to patients undergoing ALND beginning in March 2015. Patients who developed lymphedema were compared with those who did not. Demographics and potential risk factors for development of lymphedema such as age, body mass index, clinical stage, radiotherapy, and chemotherapy were reviewed. RESULTS: Eighty-seven patients participated in the surveillance program over the study period with an average age of 60 y (range 32-83) and body mass index of 30 kg/m(2) (range 17–46). The single most significant risk factor for the development for lymphedema was an ALND (P < 0.001). One of 67 patients undergoing a sentinel lymph node biopsy developed lymphedema (1.5%). Four of 10 patients who underwent an ALND alone developed lymphedema (40%). One of 8 patients in the ALND + LYMPHA group developed transient lymphedema (12.5%). CONCLUSIONS: Offering LYMPHA with ALND decreased our institutional rate of lymphedema from 40% to 12.5%. Long-term follow-up and randomized control trials are necessary to further elucidate the promise of this surgical technique to reduce the incidence of BCRL.
Ikari, N., et al. (2018). “Somatic mutations and increased lymphangiogenesis observed in a rare case of intramucosal gastric carcinoma with lymph node metastasis.” Oncotarget 9(12): 10808–10817.
Background and aim: Intramucosal gastric adenocarcinoma of the well-moderately differentiated type only exhibits lymph node metastasis in extremely rare cases. We encountered such case and investigated both the lymphangiogenic properties and somatic mutations in the cancer to understand the prometastatic features of early-stage gastric cancer. Methods: We quantitatively measured the density of lymphatic vessels and identified mutations in 412 cancer-associated genes through next-generation target resequencing of DNA extracted from tumor cells in a formalin-fixed and paraffin-embedded tissue. Functional consequence of the identified mutation was examined in vitro by means of gene transfection, immunoblot, and the quantitative real-time polymerase chain reaction assay. Results: The intramucosal carcinoma was accompanied by abundant lymphatic vessels. The metastatic tumor harbored somatic mutations in NBN, p.P6S, and PAX8, p.R49H. The PAX8(R49H) showed significantly higher transactivation activity toward E2F1 than the wild-type PAX8 (P < 0.001). Conclusions: Our data suggest that increased lymphangiogenesis and somatic mutations of NBN and/or PAX8 could facilitate lymph node metastasis from an intramucosal gastric carcinoma. These findings may potentially inform evaluations of the risk of developing lymph node metastasis in patients with intramucosal gastric cancer.
Iyer, N. S., et al. (2018). “Lymphedema in ovarian cancer survivors: Assessing diagnostic methods and the effects of physical activity.” Cancer. [EPub Feb 13]
BACKGROUND: Lymphedema is a poorly understood side effect of gynecologic cancer treatment. This study was designed to determine the prevalence of lower limb lymphedema (LLL) in a sample of ovarian cancer survivors via 3 different diagnostic methods and to assess the effect of a randomized exercise intervention. METHODS: Physically inactive ovarian cancer survivors (n = 95) were enrolled in a 6-month randomized trial of exercise (primarily brisk walking) versus attention control. LLL was measured at baseline and 6-month visits via a self-report questionnaire, optoelectronic perometry, and an evaluation by a certified lymphedema specialist. RESULTS: LLL prevalence ranged from 21% to 38% according to the diagnostic method, and there was substantial agreement between the self-report questionnaire and the lymphedema specialist evaluation (kappa = 0.61). There was no agreement between the evaluation with optoelectronic perometry and the specialist evaluation. With LLL defined by any method, the baseline prevalence was 38% in both groups. At 6 months, both groups experienced a decreased LLL prevalence: 28% in the exercise group and 35% in the control group. There was no difference in the change in lymphedema prevalence between the 2 groups (P = .64). Body mass index was a significant predictor of LLL. CONCLUSIONS: With a potential prevalence of LLL as high as 40%, further evaluation of diagnostic methods is required to better characterize this side effect of ovarian cancer treatment. No adverse effect of exercise on LLL was found. Further research is strongly needed to evaluate predictors of LLL and the effects of exercise on LLL in order to develop effective physical activity recommendations for women with ovarian cancer. Cancer 2018. (c) 2018 American Cancer Society.
Li, B. and Z. Wang (2018). “Stewart-Treves syndrome: Magnetic resonance imaging data compared with pathological results from a single center.” Oncol Lett 15(1): 1113–1118.
The aim of the present study was to evaluate the magnetic resonance imaging (MRI) data of patients with Stewart-Treves Syndrome (STS), and to compare them with the corresponding pathological data. A total of 4,289 cases of secondary upper limb lymphedema (LE) from a single center, including 5 female cases of STS who underwent modified-radical post mastectomy, were included in the study. All cases were diagnosed pathologically, and by conventional and contrast-enhanced (ce)MRI scans. A total of 43 tumor nodules (Phi >/ = 4 mm) were examined. According to the immunohistochemical results, the 5 cases of STS were divided into 2 types; 4 patients exhibited STS type I [angiosarcoma (AS)] and 1 patient exhibited STS type 2 [mixed lymphangiosarcoma (mLAS)]. The MRI signal intensity (SI) of all the nodules was compared with the pathological results. In the T1WI sequences, all nodules showed isointensity compared with normal muscle tissues in the same image. However, in the T2WI sequences, there were the visually recognizable differences in the SI compared with the LE tissues in the two STS types. The SI of mLAS was more markedly decreased compared with that of AS. The SI of mLAS was closer to that of normal muscle tissues compared with the SI of AS. In the ceMRI, the SI of the tumor nodules was markedly increased in the two STS types, compared with non-enhancement imaging. Overall, MRI is a useful tool for the evaluation and diagnosis of STS. A chronic case of LE, in which MRI examination demonstrates nodules within the LE, may suggest a diagnosis of STS.
Liang, L., et al. (2018). “A meta-analysis of the lymphatic microvessel density and survival in gastric cancer with 1809 cases.” Oncotarget 9(4): 5406–5415.
Lymph node metastasis commonly occurs in gastric cancer. Previous studies have demonstrated that the overexpression of lymphatic microvessel density (LVD) is correlated with various malignancies. To evaluate the potential role of LVD in various malignancies, we conducted a systematic review and meta-analysis to thoroughly investigate the association of LVD expression with tumor progression and survival in gastric cancer. We performed a comprehensive search of common databases and selected studies demonstrating the relationship between LVD expression and gastric cancer prognosis. Hazard ratios (HR) were used to determine the value of LVD for predicting gastric cancer metastasis and prognosis. The data were extracted from the included studies and pooled with the appropriate effects model using STATA 12.0. The results showed that high LVD expression obviously impacted the prognosis of gastric cancer, based on an overall survival (OS) HR of 2.58 (95% CI: 1.91-3.48, P < 0.001) and a disease-free survival (DFS) HR of 2.51 (95% CI: 1.35-4.68, P = 0.004) in the univariate analysis. In addition, the results of the multivariate analysis indicated a remarkable relationship between high LVD expression and gastric neoplasm prognosis. The pooled OS HR was 4.12 (95% CI: 3.45-4.91, P < 0.001). The current meta-analysis shows that high LVD is closely related to tumor metastasis and poor prognosis in gastric malignancy. LVD could be a key factor in tumor lymphatic metastasis. Moreover, LVD is likely a potential index and an effective biomarker for the prediction of patient prognosis.
Mitrofanova, I., et al. (2018). “The effect of neoadjuvant chemotherapy on the correlation of tumor-associated macrophages with CD31 and LYVE-1.” Immunobiology 223(6-7): 449–459.
Angiogenesis and lymphangiogenesis play a crucial role in tumor growth, invasion and metastasis. Tumor-associated macrophages (TAM) induce both angiogenesis and lymphangiogenesis in mouse breast cancer models and positively correlate with these processes in human breast cancer patients. Neoadjuvant chemotherapy (NAC) is a widely used therapeutic option for cancer treatment. However, the effect of NAC on the distribution of TAM within intratumoral compartments and their correlation with angiogenesis and lymphangiogenesis remained unknown. In the present study we analyzed the effect of NAC on the distribution of CD68+ and stabilin-1+ TAM in five functionally distinct areas of human breast cancer and their correlations with microvessel density (MVD) and lymphatic microvessel density (LMVD), identified by CD31 and LYVE1, respectively. We found that NAC enhances blood vessel density in soft fibrous stroma and in coarse fibrous stroma. Without NAC the amount of CD68+ TAM in gaps of ductal tumor structures positively correlate with CD31+ microvessel density in soft fibrous stroma. NAC had enhancing effect on the amount of CD68+ TAM but not stabilin-1+ TAM in soft fibrous stroma. However, no correlation between TAM and CD31+ microvessel density was identified after NAC. NAC did not enhance the lymphatic microvessel density. But after NAC stabilin-1 expressing subpopulation of TAM positively correlated with expression of LYVE-1. We hypothesized that CD68+ TAM can support tumor angiogenesis primarily before NAC, while stabilin-1+ TAM can contribute to the maintenance of lymphatic microvessel density after NAC.
Parmar, P., et al. (2018). “Clinicopathological significance of tumor lymphatic vessel density in head and neck squamous cell carcinoma.” Indian J Otolaryngol Head Neck Surg 70(1): 102–110.
Various studies have demonstrated that the lymphatic system is the additional route for solid tumor metastasis. Lymph nodes metastasis in Head and neck squamous cell carcinoma (HNSCC) is a major prognostic indicator for disease progression and a guide for therapeutic strategies. We conducted a study to compare intratumoral (IT) and peritumoral (PT) lymphatic vessel density (LVD) in HNSCC using lymphatic marker D2-40 and its correlation with lymph node metastasis, histological grading and other clinicopathological parameters. Fifty specimen of HNSCC with modified radical neck dissection tissue were included in the study group. Tissue from tumor, peritumoral tissue, tumor margin and all the lymph nodes were processed for paraffin wax blocks and histopathological diagnosis. Immunohistochemical profile of lymphatic vessels in intratumoral and peritumoral tissue was assessed by subjecting one section each from the tumor and peritumoral tissue to D2-40 immunostain. To determine LVD, four fields with the highest LVD (hot spots) were identified. The mean values were calculated by taking an average of all the measurements. The comparison of LVD between peritumoral and intratumoral area revealed significantly higher PT-LVD (P = 0.001). No significant association was seen between LVD, IT-LVD and PT-LVD and different age groups, gender, site of tumor, risk factors, size of tumor, tumor inflammation, pushing/infiltrating margin and stage of tumors. Significantly higher LVD, IT-LVD and PT-LVD was seen in association with lymph node metastasis. Both high intratumoral and peritumoral LVD were found significantly associated with the presence of lymph node metastasis, however lymphatic vessels were found to be significantly more numerous and larger in peritumoral areas as compared to intratumoral lymphatics. The specificity of D2-40 as a lymphatic endothelial marker was also confirmed. The results of our study support the possibility of using the determination of tumor lymphangiogenesis to identify patients of HNSCC who are at risk of developing the lymph node metastasis.
Sezgin Ozcan, D., et al. (2018). “Complex decongestive therapy enhances upper limb functions in patients with breast cancer-related lymphedema.” Lymphat Res Biol. [EPub Jan 22]
BACKGROUND: We aimed to evaluate the effects of complex decongestive therapy (CDT) on upper extremity functions, the severity of pain, and quality of life. We also searched the impact of the sociodemographic and clinical characteristics on the improvement in upper extremity functions. METHODS: A total of 37 women with breast cancer-related lymphedema (BCRL) [age, 53.6 +/- 11.2 (28-72)] were included in this study. All patients underwent CDT-phase 1 program, including meticulous skin care, manual lymphatic drainage, remedial exercises, and compression bandages. Arm volume was calculated by a formula for truncated cone using circumferential measurements. A baseline questionnaire, including sociodemographic and clinical properties, was used for each patient. Short Form-36 (SF-36), Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire, and Visual Analog Scale (VAS) for pain and heaviness were used as clinical assessment scales. RESULTS: The mean of the posttreatment volume of the affected limb was lower compared to pretreatment volume (2741.81 +/- 696.85 and 2990.67 +/- 745.49, respectively), and the mean percentage change in edema volume was 38.1% +/- 26.5%. We observed a statistically significant reduction in pain and heaviness VAS scores and improvement of shoulder mobility among upper extremities with lymphedema (p < 0.001) after CDT. The mean of posttreatment DASH score was lower compared to pretreatment score (37.19 +/- 16.01, 49.81 +/- 18.84, respectively, p < 0.001). All subgroups of the SF-36 parameters were increased after the CDT application (p < 0.01). Besides being under 65 years old, having a body mass index above 30 and short duration of lymphedema were found to be related to greater improvement in upper extremity functions. CONCLUSIONS: CDT provides enhancement of upper extremity functions and quality of life in patients with BCRL. The reduction in lymphedema volume, pain, and heaviness and the improvement in shoulder mobility may be the contributed factors.
Siotos, C., et al. (2018). “Breast reconstruction and risk of arm lymphedema development: A meta-analysis.” J Plast Reconstr Aesthet Surg. [EPub Feb 21]
BACKGROUND: Lymphedema remains a significant complication following breast cancer surgery when there is axillary lymph node intervention. Previous systematic reviews have identified risk factors for breast cancer-related lymphedema, including increased BMI, number of lymph nodes dissected and radiotherapy. However, they have not examined the effect of breast reconstruction on lymphedema occurrence. In this systematic review and meta-analysis, we sought to evaluate the association between breast reconstruction (BR) and lymphedema. METHODS: We searched PubMed (1966–2016), Embase (1966–2016), Scopus (2004–2016) and Google Scholar (2004–2016) for studies involving breast reconstruction and upper-extremity lymphedema or breast cancer-related lymphedema. Our primary outcome was lymphedema occurrence. We performed a meta-analysis using random effects due to heterogeneity of the studies. RESULTS: Our search strategy identified 934 articles. After screening, 19 studies were included in our meta-analysis evaluating outcomes based on number of patients (7501) or number of breasts surgically treated (2063). Breast reconstruction was significantly associated with lower odds of lymphedema (p < 0.001) compared to mastectomy only or breast-conserving surgery. Lymphedema rates were not statistically significantly different between patients undergoing implant-based or autologous BR. CONCLUSIONS: Breast reconstruction is associated with lower rates of lymphedema compared to mastectomy only or breast conserving surgery patients. Although the study does not prove causation, we hypothesize that this association is likely due to multiple factors, including a self-selecting population and mechanisms through which BR may contribute to primary or secondary prevention of lymphedema. Further prospective studies are needed to clarify this beneficial relationship between breast reconstruction and reduced lymphedema risk.
Tanaka, N., et al. (2018). “Mapping of the three-dimensional lymphatic microvasculature in bladder tumours using light-sheet microscopy.” Br J Cancer. [EPub Mar 8]
BACKGROUND: Cancers are heterogeneous and contain various types of irregular structures that can go undetected when examining them with standard two-dimensional microscopes. Studies of intricate networks of vasculature systems, e.g., the tumour lymphatic microvessels, benefit largely from three-dimensional imaging data analysis. METHODS: The new DIPCO (Diagnosing Immunolabeled Paraffin-Embedded Cleared Organs) imaging platform uses three-dimensional light-sheet microscopy and whole-mount immunolabelling of cleared samples to study proteins and micro-anatomies deep inside of tumours. RESULTS: Here, we uncovered the whole three-dimensional lymphatic microvasculature of formalin-fixed paraffin-embedded (FFPE) tumours from a cohort of 30 patients with bladder cancer. Our results revealed more heterogeneous spatial deviations in more advanced bladder tumours. We also showed that three-dimensional imaging could determine tumour stage and identify vascular or lymphatic system invasion with higher accuracy than standard two-dimensional histological diagnostic methods. There was no association between sample storage times and outcomes, demonstrating that the DIPCO pipeline could be successfully applied on old FFPE samples. CONCLUSIONS: Studying tumour samples with three-dimensional imaging could help us understand the pathological nature of cancers and provide essential information that might improve the accuracy of cancer staging.
Wang, J., et al. (2018). “NRP-2 in tumor lymphangiogenesis and lymphatic metastasis.” Cancer Lett 418: 176–184.
Neuropilin-2 (NRP-2) not only functions as a receptor for semaphorins, a family of neural axon guidance factors, but also interacts with VEGFs, a family of vascular endothelial growth factors. As an independent receptor or a co-receptor, NRP-2 binds to ligands VEGF-C/D, activates the VEGF-C/D-NRP-2 signaling axis, and further regulates lymphangiogenesis-associated factors in both lymphatic endothelial cells (LECs) and some tumor cells during tumor progression. Via VEGF-C/D-NRP-2 axis, NRP-2 induces LEC proliferation, reconstruction and lymphangiogenesis and subsequently promotes tumor cell migration, invasion and lymphatic metastasis. There are similarities and differences among NRP-1, NRP-2 and VEGFR-3 in chemical structure, ligand specificity, chromosomal location, soluble protein forms, cellular functions and expression profiles. High expression of NRP-2 in LECs and tumor cells has been observed in different anatomic sites, histological patterns and progression stages of various tumors, especially during tumor lymphangiogenesis and lymphatic metastasis, and therefore the NRP-2 and VEGF-C/D-NRP-2 axis are closely related to tumor development, progression, invasion, and metastasis. In addition, it is important for prognosis of tumor. The studies on NRP-2 targeted therapy have recently achieved some successes, utilizing NRP-2 blocking antibodies, NRP-2 inhibitory peptides, soluble NRP-2 antagonists, small molecule inhibitors and various NRP-2 gene therapeutic strategies.
Wang, Q. S., et al. (2018). “FOXF2 deficiency permits basal-like breast cancer cells to form lymphangiogenic mimicry by enhancing the response of VEGF-C/VEGFR3 signaling pathway.” Cancer Lett 420: 116–126.
Lymphatic metastasis is the main route of breast cancer metastasis. It is known that lymphangiogenesis facilitates lymphatic metastasis through vascular endothelial growth factor-C (VEGF-C)/VEGF receptor 3 (VEGFR3) pathway-linked interactions between the tumor and its microenvironment. Here, we report a novel mechanism of lymphatic metastasis by which aggressive basal-like breast cancer (BLBC) cells form lymphatic vessel-like structures that are identified by the positive expression of lymphatic endothelial cell markers lymphatic vessel endothelial hyaluronan receptor 1 (LYVE-1), podoplanin, and VEGFR3, and termed as lymphangiogenic mimicry (LM), for the first time. Our clinical evidence and experimental data in vivo and in vitro revealed that forkhead box F2 (FOXF2) deficiency promotes the lymphatic metastasis of BLBC by conferring a lymphangiogenic mimetic feature upon cancer cells through directly activating VEGFR3 transcription. The fact that FOXF2 controls the activation of the VEGF-C/VEGFR3 signaling pathway in BLBC cells provides potential molecular diagnostic and therapeutic strategies for lymphatic metastasis in BLBC patients.
Yamamoto, T., et al. (2018). “Lymphatic vessel diameter in female pelvic cancer-related lower extremity lymphedematous limbs.” J Surg Oncol. [EPub Jan 22]
BACKGROUND: Lymphaticovenular anastomosis (LVA) has become one of the useful surgical treatments for compression-refractory lower extremity lymphedema (LEL). It is important to anastomose larger lymphatic vessels with abundant lymph flows in LVA surgery. This study aimed to clarify factors associated with lymphatic vessel diameter. METHODS: One hundred thirty-four LEL patients who underwent pre-operative indocyanine green (ICG) lymphography and LVA from June 2009 to August 2014 in a single institution were included in this retrospective observational study. Clinical, ICG lymphography, and intraoperative findings were collected from medical charts. A lymphatic vessel with external diameters of 0.5 mm or larger was defined as a large lymphatic vessel (LLV). Independent factors associated with LLV were identified using logistic regression analysis. RESULTS: Nine hundred sixty-two lymphatic vessels were identified, among which 438 (45.5%) were LLVs. Independent factors associated with LLV were older age (odds ration [OR], 1.408; 95% confidence interval [CI], 1.026-1.931; P = 0.034), positive history of radiation (OR, 1.634; 95%CI 1.228-2.173; P = 0.001), incision site in the thigh/lower leg compared with in the groin (OR, 1.617/1.685; 95%CI 1.076-2.432/1.148-2.473; P = 0.021/0.008). Inverse associations were observed in S-region/D-region on ICG lymphography compared with L-region (OR, 0.537/0.048; 95%CI, 0.397-0.726/0.006-0.371; P < 0.001/0.004). CONCLUSIONS: D-region on ICG lymphography had the lowest OR to find LLV, representing that lymphatic vessels found in D-region on ICG lymphography would be significantly smaller than those in L-region. In LVA surgery, D-region should be avoided.
Zou, L., et al. (2018). “The incidence and risk factors of related lymphedema for breast cancer survivors post-operation: a 2-year follow-up prospective cohort study.” Breast Cancer. [EPub Feb3]
PURPOSE: To investigate the incidence rate, severity and risk factors of related lymphedema in breast cancer survivors. METHODS: A 2-year follow-up prospective study of 387 women who had operation from four hospitals from January 1, to December 31, 2014 was conducted. Limb volume was measured by circumference and symptoms were measured using questionnaires pre-treatment and 1, 3, 6, 12, 18, 24 months after surgery separately. The incidence rates and the severity of lymphedema were evaluated, respectively. Risk factors for the development of breast cancer-related lymphedema (BCRL) were analyzed using log-rank test and Cox regression. RESULTS: The incidences of BCRL were 4.4, 10.1, 15.2, 28.6, 31.2 and 32.5% at 1, 3, 6, 12, 18, 24 months after surgery, respectively, measured by Norman questionnaire. The rates measured by arm circumference were 2.5, 6.7, 13.4, 21.4, 26.3 and 29.4%, respectively. About 114 (29.4% of 387) women were diagnosed with BCRL, and 78 of them got mild lymphedema. Axillary lymph node dissection (ALND) (HR = 5.2, 95% CI 1.6-17.3), radiotherapy (HR = 3.9, 95% CI 2.0-7.5), modified radical mastectomy (MRM) (HR = 2.1, 95% CI 1.3-3.4), the number of positive lymph nodes (HR = 1.1, 95% CI 1.0-1.2) and body mass index (BMI) (HR = 1.1, 95% CI 1.0-1.1) were independent risk factors for BCRL. CONCLUSIONS: BCRL is a common complication for breast cancer patients after surgery. It can be fairly diagnosed only 1 month post-operation and the cumulative incidence of BCRL seems to be increasing over time, especially in the first year after surgery. ALND, radiotherapy, MRM, the number of positive axillary lymph nodes and BMI were found to be independent risk factors in the development of BCRL in this study.
Vascular Anomalies
Boulouis, G., et al. (2017). “Arterial spin-labeling to discriminate pediatric cervicofacial soft-tissue vascular anomalies.” AJNR Am J Neuroradiol 38(3): 633–638.
BACKGROUND AND PURPOSE: Differentiating major subtypes of cervicofacial vascular lesions is crucial for appropriate management. The aim of our study was to evaluate the performance of an MR imaging arterial spin-labeling perfusion sequence in discriminating pediatric cervicofacial soft-tissue vascular anomalies. MATERIALS AND METHODS: We conducted a retrospective analysis of data from a prospectively maintained registry including pediatric patients at a tertiary pediatric center between January 2012 and January 2014. We included pediatric patients with a final diagnosis of soft-tissue vascular anomalies and an MR imaging, including an arterial spin-labeling sequence at presentation. We performed an analysis of lesion perfusion, blinded to clinical data, by using concurrent spiral 3D pseudocontinuous arterial spin-labeling (1.5T magnet; spiral matrix, 512 x 8 mm; postlabeling delay, 1025 ms). Lesional flow was recorded with calibrated intralesional ROIs. Perfusion characteristics were compared among lesion subtypes with the Mood Median test. RESULTS: Among 840 patients screened, 46 matched the inclusion criteria and were included (median age, 1.45 years; interquartile range, 0.4-5.1 years; 27 females). Hemangiomas, including infantile hemangiomas (n = 18 patients) and noninvoluting (n = 2) and rapidly involuting (n = 1) congenital types, demonstrated marked hyperperfusion (median flow, 436 mL/min/100 g; interquartile range, 212.5-603 mL/min/100 g), significantly higher than that of lymphatic malformations (median, 22.5 mL/min/100 g; interquartile range, 16-60 mL/min/100 g; P < .001) or venous malformations (median, 25 mL/min/100 g; interquartile range, 15-66.5 mL/min/100 g; P = .003). CONCLUSIONS: MR imaging arterial spin-labeling is a valuable tool for the assessment of soft-tissue vascular anomaly hemodynamics and for the classification of major lesion subtypes.
Chang, L., et al. (2018). “Intralesional bleomycin injection for propranolol-resistant hemangiomas.” J Craniofac Surg 29(2): e128-e130.
Propranolol has been the first-line treatment for alarming hemangiomas. However, some hemangiomas are propranolol-resistant. The authors reported 1 propranolol-resistant hemangioma which was treated with intralesional bleomycin injections. Sixteen months after 3 injections, the lesion still remained stable. Its potential mechanism was clarified by ultrasonic monitoring. Intralesional bleomycin injection can be considered an ideal option in treating propranolol-resistant hemangiomas.
Crenshaw, M. M., et al. (2018). “Orthopaedic management of leg-length discrepancy in proteus syndrome: A case series.” J Pediatr Orthop 38(3): e138-e144.
INTRODUCTION: Proteus syndrome (PS) is a rare mosaic disorder comprising asymmetric bony and soft tissue overgrowth leading to significant morbidity. Placement of growth inhibition hardware with subsequent epiphyseal arrest improves leg-length and angular deformities in pediatric patients without PS. The purpose of this study was to review the surgical approach and present outcomes, complications, and recommendations in 8 patients with PS and leg-length discrepancy (LLD). METHODS: We conducted a retrospective chart review of 8 patients with PS whose primary reason for surgery was LLD. Patients were eligible if they met clinical diagnostic criteria for PS and if the National Institutes of Health team performed at least 1 of their surgical interventions between 2005 and 2015. Surgical techniques included growth inhibition, with tension band plates, applied >/ = 1 times, and epiphyseal arrest. RESULTS: Eight patients, followed for an average of 4.6 years (range, 1.0 to 7.1 y) after the index procedure, were included in this analysis. Average age at first LLD surgery was 9.4 years (range, 6.1 to 13.6 y); the average LLD was 3.4 cm (range, 0.4 to 7.0 cm) at presentation, and 5.0 cm (range, 1.8 to 10.0 cm) at the time of the first LLD surgery. Participants underwent 23 total surgeries (range, 1 to 5 per patient) and 7 patients have completed surgical intervention. For the 7 patients who did not require overcorrection the average LLD at the last clinical encounter was 2.6 cm (range, 0.6 to 7.2 cm). We encountered 2 complications: 2 patients developed mild knee valgus, which responded to standard guided growth techniques. CONCLUSIONS: This case series suggests that growth inhibition and epiphyseal arrest in children with PS can reduce LLD with few complications. Careful monitoring, rapid mobilization, deep venous thrombosis prophylaxis, and sequential compression devices were also integral elements of our surgical protocol. LEVEL OF EVIDENCE: Level IV.
Duran, D., et al. (2018). “Human genetics and molecular mechanisms of vein of Galen malformation.” J Neurosurg Pediatr: 1–8.
Vein of Galen malformations (VOGMs) are rare developmental cerebrovascular lesions characterized by fistulas between the choroidal circulation and the median prosencephalic vein. Although the treatment of VOGMs has greatly benefited from advances in endovascular therapy, including technical innovation in interventional neuroradiology, many patients are recalcitrant to procedural intervention or lack accessibility to specialized care centers, highlighting the need for improved screening, diagnostics, and therapeutics. A fundamental obstacle to identifying novel targets is the limited understanding of VOGM molecular pathophysiology, including its human genetics, and the lack of an adequate VOGM animal model. Herein, the known human mutations associated with VOGMs are reviewed to provide a framework for future gene discovery. Gene mutations have been identified in 2 Mendelian syndromes of which VOGM is an infrequent but associated phenotype: capillary malformation-arteriovenous malformation syndrome ( RASA1) and hereditary hemorrhagic telangiectasia ( ENG and ACVRL1). However, these mutations probably represent only a small fraction of all VOGM cases. Traditional genetic approaches have been limited in their ability to identify additional causative genes for VOGM because kindreds are rare, limited in patient number, and/or seem to have sporadic inheritance patterns, attributable in part to incomplete penetrance and phenotypic variability. The authors hypothesize that the apparent sporadic occurrence of VOGM may frequently be attributable to de novo mutation or incomplete penetrance of rare transmitted variants. Collaboration among treating physicians, patients' families, and investigators using next-generation sequencing could lead to the discovery of novel genes for VOGM. This could improve the understanding of normal vascular biology, elucidate the pathogenesis of VOGM and possibly other more common arteriovenous malformation subtypes, and pave the way for advances in the diagnosis and treatment of patients with VOGM.
El Hachem, M., et al. (2017). “Safety and effectiveness of oral propranolol for infantile hemangiomas started before 5 weeks and after 5 months of age: an Italian multicenter experience.” Ital J Pediatr 43(1): 40.
BACKGROUND: Despite not being licensed for the treatment of infantile hemangiomas (IH) in infants younger than 5 weeks or older than 5 months, propranolol is often used in these age groups to prevent or to treat potentially severe complications. The objective of the present study was to review the experience of 8 Italian pediatric and dermatologic centers regarding propranolol treatment for IH started before 5 weeks or after 5 months of age. METHODS: We retrospectively reviewed the records of patients followed up for IH, on propranolol treatment started before 5 weeks or after 5 months of age, and collected information on sociodemographic data, treatment indications, IH involution, IH relapse, and treatment side effects. RESULTS: A total of 343 patients were enrolled; 15 were started on propranolol before 5 weeks (group 1), 328 were started after 5 months of age (group 2). The most frequent indications were permanent aesthetical disfigurement (91.8%) and function threatening complications (42.6%). In most cases, the treatment was effective. The involution was partial in 67.7% of patients. In 11.8% of cases a relapse was observed. No relapse was observed in group 1. Treatment complications were reported in 15.8% of children, most frequently sleep disorders (6.6%), followed by irritability (5.1%) and diarrhea (2.2%). Only a case of mild constipation was observed in group 1. CONCLUSION: The safety and effectiveness profile of propranolol in infants younger than 5 weeks or older than 5 months may be acceptable. Taking in account propranolol's potential in preventing severe complications, further studies should assess the acceptability of propranolol treatment, especially in the <5-week age group.
Gamboa, N. T., et al. (2018). “Clinical presentation and treatment paradigms of brain arteriovenous malformations in patients with hereditary hemorrhagic telangiectasia.” J Clin Neurosci. [EPub Feb 23]
Hereditary hemorrhagic telangiectasia (HHT) is characterized by recurrent spontaneous epistaxis, mucocutaneous telangiectases, and multisystem arteriovenous malformations (AVMs). Brain AVMs typically present at birth and are identified in approximately 10-20% of patients with HHT. A retrospective review was undertaken of all HHT patients with known single or multiple brain AVMs treated at our institution. Thirty-nine patients with brain AVM(s) were diagnosed with HHT. Most patients presented with at least one Curacao criterion. A total of 78 brain AVMs were identified in 39 patients. Two-thirds of patients had solitary brain AVMs, whereas 33% of patients harbored at least two lesions (range: 2-16). Brain AVMs of the supratentorial cerebral hemispheres comprised 83% of all lesions, whereas infratentorial lesions accounted for only 17%. Of the 55 brain AVMs assigned Spetzler-Martin grading, the majority of patients were Grade 1 (73%), and 23% and 4% were Grades 2 and 3, respectively. Patients were treated with surgery alone (51%), embolization alone (6%), embolization followed by surgery (9%), stereotactic radiosurgery (11%), stereotactic radiosurgery followed by surgery (3%), or observation (20%). Of patients who underwent genetic analysis, 62% possessed mutations in ENG (HHT type 1), whereas 38% had mutations in ACVRL1 (HHT type 2). This robust patient cohort of brain AVMs in 39 patients with HHT advances the collective understanding of this disease's varied presentation, diagnostic workup, genetic underpinnings, and available treatment options.
Gossage, J. R. (2018). “The current role of bevacizumab in the treatment of hereditary hemorrhagic telangiectasia-related bleeding.” Mayo Clin Proc 93(2): 130–132.
Guo, X., et al. (2017). “Continuous delivery of propranolol from liposomes-in-microspheres significantly inhibits infantile hemangioma growth.” Int J Nanomedicine 12: 6923–6936.
PURPOSE: To reduce the adverse effects and high frequency of administration of propranolol to treat infantile hemangioma, we first utilized propranolol-loaded liposomes-in-microsphere (PLIM) as a novel topical release system to realize sustained release of propranolol. METHODS: PLIM was developed from encapsulating propranolol-loaded liposomes (PLs) in microspheres made of poly(lactic-co-glycolic acid)-b-poly(ethylene glycol)-b-poly(lactic-co-glycolic acid) copolymers (PLGA-PEG-PLGA). The release profile of propranolol from PLIM was evaluated, and its biological activity was investigated in vitro using proliferation assays on hemangioma stem cells (HemSCs). Tumor inhibition was studied in nude mice bearing human subcutaneous infantile hemangioma. RESULTS: The microspheres were of desired particle size (∼77.8 mum) and drug encapsulation efficiency (∼23.9%) and achieved sustained drug release for 40 days. PLIM exerted efficient inhibition of the proliferation of HemSCs and significantly reduced the expression of two angiogenesis factors (vascular endothelial growth factor-A [VEGF-A] and basic fibroblast growth factor [bFGF]) in HemSCs. Notably, the therapeutic effect of PLIM in hemangioma was superior to that of propranolol and PL in vivo, as reflected by significantly reduced hemangioma volume, weight, and microvessel density. The mean hemangioma weight of the PLIM-treated group was significantly lower than that of other groups (saline = 0.28 g, propranolol = 0.21 g, PL = 0.13 g, PLIM = 0.03 g; PLIM vs saline: P < 0.001, PLIM vs propranolol: P < 0.001, PLIM vs PL: P < 0.001). The mean microvessel density of the PLIM-treated group was significantly lower than that of other groups (saline = 40 vessels/mm(2), propranolol = 31 vessels/mm(2), PL = 25 vessels/mm(2), PLIM = 11 vessels/mm(2); PLIM vs saline: P < 0.001, PLIM vs propranolol: P < 0.01, PLIM vs PL: P < 0.05). CONCLUSION: Our findings show that PLIM is a very promising approach to locally and efficiently deliver propranolol to the hemangioma site leading to a significant inhibition of infantile hemangioma.
Hu, P. A. and Z. R. Zhou (2018). “Clinical and imaging features of kaposiform hemangioendothelioma.” Br J Radiol: 20170798.
PURPOSES: Kaposiform hemangioendothelioma (KHE) is a unique locally aggressive vascular tumor with poor prognosis. The aim of this study is to assess the clinical and imaging features of KHE, and to compare the differences between solitary and diffusive infiltrative subtype further. METHODS: The clinical and radiological findings of a cohort of 25 cases with histologically proven KHE, between June 2011 and June 2016, were reviewed retrospectively. Seven solitary and 18 diffusive infiltrative subtypes KHE were included. The differences of clinical and imaging features between these two subtypes were compared statistically by Wilcoxon rank sum test and Fisher exact test. RESULTS: The median age was 4 months old. Twenty cases (80%) were accompanied by Kasabach-merritt phenomenon (KMP). Most KHE located in trunk and/or extremity. The masses showed inhomogeneous echogenicity and were rich in vascularity on ultrasound; showed iso- attenuation relative to muscle on unenhanced CT, iso-(n = 15) or slightly hyper- (n = 7) intense T1WI signal relative to muscle, mainly heterogeneous hyper- or slightly hyper- with speckled hypo- intense (n = 17) T2WI signal (77%) relative to muscle, and notable (n = 15) and moderate (n = 3) enhancement. Feeding and draining vessels were revealed in 15 cases. Five masses with DWI showed slightly restricted diffusivity, with average ADC value of (1.28 +/- 0.09) x 10(−3)mm(2) s(-)(1). Necrosis and hemorrhage were also found. Compared with solitary ones, diffusive infiltrative KHE were larger, more commonly accompanied by KMP and reticular lymphedema, and more frequently located in trunk and/or extremity. CONCLUSION: Five masses with DWI showed slightly restricted diffusivity. A hyper-vascular mass accompanied by KMP and reticular lymphedema, with speckled hypo- intense signal T2WI signal, especially in pediatric patients, is highly suggestive of the diagnosis of KHE. Advances in knowledge: Speckled hypo- intense signal T2WI signal, and notable enhancement were unique features of KHE. KHE showed slightly restricted diffusivity on DWI, commonly accompanied by KMP and reticular lymphedema.
Ivars, M., et al. (2018). “Fern-shaped patch as a hallmark of blue rubber bleb nevus syndrome in neonatal venous malformations.” Eur J Pediatr. [EPub Mar 8]
Blue rubber bleb nevus syndrome (BRBNS) is a rare congenital vascular disease associated with important morbidity and non-insignificant risk of mortality in cases of severe gastrointestinal or neurological involvement. Early diagnosis in the neonatal period can be difficult as very often skin lesions appear progressively during childhood having no correlation with gastrointestinal lesion development. The appearance of one large venous malformation (VM) in the neonatal period has suggested a characteristic finding of this syndrome. The objective of the study was to identify a specific clinical sign in the congenital venous malformations (VMs) of the BRBNS to distinguish them from the conventional VMs. Clinical histories of all patients diagnosed with BRBNS were reviewed, including those who presented a large VM at birth. Clinical characteristics of congenital VM associated with BRBNS were recorded. Five patients with BRBNS were found to have a large VM since birth. All of them presented a fern-shaped patch over the surface of the VM. CONCLUSION: The finding of this macroscopic sign in the evaluation of the newborn with a VM could be considered as a guiding syndromic herald which should raise suspicion for BRBNS and allow for more accurate evaluation and surveillance for complications. What is Known: * BRBNS is a rare vascular disease associated with important morbidity and non-insignificant risk of mortality in cases of severe gastrointestinal or neurological involvement. * Early diagnosis in the neonatal period can be difficult as very often skin lesions appear progressively during childhood having no correlation with gastrointestinal lesion development. What is New: * Recognition of a fern-shaped patch in neonates with a VM should raise suspicion for BRBNS and allow for more accurate evaluation and surveillance for complications.
Iyer, V. N., et al. (2018). “Intravenous bevacizumab for refractory hereditary hemorrhagic telangiectasia-related epistaxis and gastrointestinal bleeding.” Mayo Clin Proc 93(2): 155–166.
OBJECTIVE: To present a multiyear clinical experience with intravenous bevacizumab for the management of severe gastrointestinal bleeding and/or epistaxis in patients with hereditary hemorrhagic telangiectasia (HHT). PATIENTS AND METHODS: All patients treated with intravenous bevacizumab for severe hereditary hemorrhagic telangiectasia-related bleeding from June 1, 2013, through January 31, 2017, were included in this report. Severity of epistaxis (determined using the Epistaxis Severity Score questionnaire); hemoglobin, iron, and ferritin levels; and quality of life data were collected serially in all patients. RESULTS: Intravenous bevacizumab was administered to 34 patients using a standardized treatment protocol. Anemia was primarily related to severe epistaxis (n = 15, 44%), severe gastrointestinal bleeding (n = 4, 12%), or both (n = 15, 44%), with a median baseline hemoglobin level of 9.1 g/dL (range, 8.3-10.5 gm/dL; to convert to mmol/L, multiply by 0.62). Red blood cell (RBC) transfusions had been administered to 28 patients (82%). Of these, 16 patients (47%) were RBC transfusion dependent and had received a median of 75 RBC transfusions (range, 4->500 RBC units) before bevacizumab initiation. The median length of follow-up was 17.6 months from the beginning of bevacizumab treatment (range, 3-42.5 months). There was a significant reduction in epistaxis severity scores (P < .001) and RBC transfusion requirements (P = .007) after completion of the initial bevacizumab treatment cycle. New-onset or worsened hypertension was noted in 4 patients, with 1 patient experiencing hypertensive urgency with a temporary decline in renal function. CONCLUSION: Intravenous bevacizumab is an effective treatment option for patients with severe anemia related to epistaxis and/or gastrointestinal bleeding. Further studies are needed to establish a dose-response relationship as well as clinical, genetic, and biomarker predictors of response.
Jiang, X., et al. (2018). “Inactivating mutations in Drosha mediate vascular abnormalities similar to hereditary hemorrhagic telangiectasia.” Sci Signal 11(513).
The transforming growth factor-beta (TGF-beta) and bone morphogenetic protein (BMP) family of cytokines critically regulates vascular morphogenesis and homeostasis. Impairment of TGF-beta or BMP signaling leads to heritable vascular disorders, including hereditary hemorrhagic telangiectasia (HHT). Drosha, a key enzyme for microRNA (miRNA) biogenesis, also regulates the TGF-beta and BMP pathway through interaction with Smads and their joint control of gene expression through miRNAs. We report that mice lacking Drosha in the vascular endothelium developed a vascular phenotype resembling HHT that included dilated and disorganized vasculature, arteriovenous fistulae, and hemorrhages. Exome sequencing of HHT patients who lacked known pathogenic mutations revealed an overrepresentation of rare nonsynonymous variants of DROSHA Two of these DROSHA variants (P100L and R279L) did not interact with Smads and were partially catalytically active. In zebrafish, expression of these mutants or morpholino-directed knockdown of Drosha resulted in angiogenesis defects and abnormal vascular permeability. Together, our studies point to an essential role of Drosha in vascular development and the maintenance of vascular integrity, and reveal a previously unappreciated link between Drosha dysfunction and HHT.
Kato, H., et al. (2016). “Craniofacial CT findings of Gorham-Stout disease and generalized lymphatic anomaly.” Neuroradiology 58(8): 801–806.
INTRODUCTION: The present study aimed to assess the craniofacial CT imaging features for differentiating between Gorham-Stout disease (GSD) and generalized lymphatic anomaly (GLA). METHODS: Seven patients with GSD and four patients with GLA were included in this study. All patients underwent CT examinations that encompassed the craniofacial bones. The presence, distribution, and type of craniofacial osteolysis were assessed. The clinical symptoms that were associated with craniofacial osteolysis were also reviewed. RESULTS: Craniofacial osteolysis including cranial osteolysis was seen in four of seven (57 %) patients with GSD and in three of four (75 %) patients with GLA. Facial osteolysis was seen in two (29 %) patients with GSD, but this was not observed in patients with GLA. Among patients with craniofacial osteolysis, those with GSD showed diffuse involvement, whereas those with GLA showed multifocal involvement. The craniofacial osteolysis of GSD could be classified into three patterns: medullary involvement, thinning bone, and disappearing bone. The clinical symptoms of craniofacial osteolysis were observed in all patients with GSD but were not present in patients with GLA. CONCLUSION: Craniofacial involvement was observed in both groups. The craniofacial osteolysis of GSD showed diffuse involvement with clinical symptoms, whereas that of GLA showed multifocal involvement without clinical symptoms.
Khanwalkar, A., et al. (2018). “Thirty-day perioperative outcomes in resection of cervical lymphatic malformations.” Int J Pediatr Otorhinolaryngol 106: 31–34.
INTRODUCTION: Limited information exists regarding short-term morbidity in the resection of lymphatic malformations. In order to make informed collaborative medical decisions, clinicians and families would benefit from information on 30-day outcomes and the expected course associated with surgical excision of lymphatic malformations. METHODS: A retrospective chart review was conducted to develop a case series of patients who underwent resection of lymphatic malformation at a pediatric tertiary care center between June 1, 2007 and September 30, 2016. Demographic data, disease characteristics, operative details, post-operative care, and adverse events in the 30-day post-operative period were analyzed. Primary outcomes included facial nerve dysfunction, seroma formation, re-admission, and overall rate of any complications. Secondary outcomes included operative time, duration of stay, and duration of drain placement. RESULTS: Forty-nine excisions were performed in 46 patients (21 male, 25 female). Median age was 5 years. All but 7 cases were performed as the initial primary intervention. Median operative time was 96min (range 22-224). Higher stage lesions (3-5) were associated with a longer operative time (p = .03). Median length of stay was 2 days (range 0-35). Higher stage lesions were associated with an increased length of stay (p = .0004). Median duration of drain placement was 2 days (range 0-14), and was longer in higher stage lesions (p = .0002). Higher stage lesions (p = .002) and cases ultimately found to have residual disease (p = .019) were associated with an increased overall rate of complications; there was no association between cyst type and rate of complications. Seroma formation (31%) and transient facial nerve weakness (26%) were the two most common complications observed. There was no association between stage or cyst type and likelihood of seroma formation. Seromas resolved after a median duration of 3 months and transient facial nerve weakness resolved after a median duration of 2 months. 3 patients required return to the OR and 1 patient was readmitted. CONCLUSION: The overall rate of adverse events after surgical excision of cervical lymphatic malformations is relatively low. Increased rates of complications can be expected with higher stage. Similarly, for these higher stage lesions, a longer operative time, hospital stay, and duration of drain placement can be expected.
Lihua, J., et al. (2017). “Somatic KRAS mutation in an infant with linear nevus sebaceous syndrome associated with lymphatic malformations: A case report and literature review.” Medicine (Baltimore) 96(47): e8016.
RATIONALE: Linear nevus sebaceous syndrome (LNSS) is a rare neurocutaneous syndrome, characterized by nevus sebaceous,central nervous system (CNS), ocular and skeletal abnormalities. The present study describes KRAS somatic mosaic mutation in a case of LNSS with lymphatic malformations (LMs). PATIENT CONCERNS: A 4-month-old female with a clinical diagnosis of LNSS presented with infantile spasms, mental retardation, skull dysplasia, ocular abnormalities, congenital atrial septal defect, and LMs. DIAGNOSIS: Cervical ultrasonography revealed a 4.6 x 4.6 x 2.2cm no echo packet with clear boundary in the subcutaneous tissues of the right neck. The neck MRI indicated a cyst in the subcutaneous tissues of the right neck. Whole-exome sequencing revealed a low-level heterozygous mutation of the KRAS gene (c.35C > T; p.G12D, 19%) in the skin lesion sample. This mutation was not present in the blood samples of the patient and her parents. INTERVENTIONS: The patient received sclerotherapy with paicibanil (OK-432) injection for the cyst. OUTCOMES: Following 1 year of treatment, the patient exhibited fewer seizures. The mental and motor development was significantly improved. The patient can currently walk with assistance and speak simple words. LESSONS: LNSS is a rare, congenital neurocutaneous syndrome consisting of a spectrum of abnormalities involving the skin, central nervous system, eyes, LMs and other systems. LNSS can be caused by postzygotic somatic mutation in the RAS family of genes. Multidisciplinary evaluation and treatment is needed.
Mahon, C., et al. (2018). “Oral propranolol for infantile haemangioma may be associated with transient gross motor delay.” Br J Dermatol.
Oral propranolol, first-line therapy for infantile haemangioma (IH) threatening functional impairment or cosmetic disfigurement, readily crosses the blood-brain barrier. Subsequently therefore, there are concerns about potential effects on infant development. Phillips et al. followed 200 children prescribed propranolol, observing sedative effects during treatment and reported gross motor abnormalities in 13 of 188 children, 7 of whom had delayed age (17-20 months) at first walking. This article is protected by copyright. All rights reserved.
Michelini, S., et al. (2018). “Genetic tests in lymphatic vascular malformations and lymphedema.” J Med Genet. [EPub Jan 12]
Syndromes with lymphatic malformations show phenotypic variability within the same entity, clinical features that overlap between different conditions and allelic as well as locus heterogeneity. The aim of this review is to provide a comprehensive clinical genetic description of lymphatic malformations and the techniques used for their diagnosis, and to propose a flowchart for genetic testing. Literature and database searches were performed to find conditions characterised by lymphatic malformations or the predisposition to lymphedema after surgery, to identify the associated genes and to find the guidelines and genetic tests currently used for the molecular diagnosis of these disorders. This search allowed us to identify several syndromes with lymphatic malformations that are characterised by a great heterogeneity of phenotypes, alleles and loci, and a high frequency of sporadic cases, which may be associated with somatic mutations. For these disorders, we found many diagnostic tests, an absence of harmonic guidelines for molecular diagnosis and well-established clinical guidelines. Targeted sequencing is the preferred method for the molecular diagnosis of lymphatic malformations. These techniques are easy to implement and have a good diagnostic success rates. In addition, they are relatively inexpensive and permit parallel analysis of all known disease-associated genes. The targeted sequencing approach has improved the diagnostic process, giving patients access to better treatment and, potentially, to therapy personalised to their genetic profiles. These new techniques will also facilitate the prenatal and early postnatal diagnosis of congenital lymphatic conditions and the possibility of early intervention.
Nassiri, N., et al. (2018). “An institution-wide algorithm for direct-stick embolization of peripheral venous malformations.” J Vasc Surg Venous Lymphat Disord. [EPub Jan 29]
OBJECTIVE: No standardized therapeutic algorithm or embolic agent of choice has yet been identified for management of congenital peripheral venous malformations (VMs). Treatment options and reported outcomes therefore vary widely. Herein, we present an institution-wide algorithm for management of symptomatic congenital peripheral VMs using a single embolotherapeutic modality. METHODS: During 36 months, patients with symptomatic congenital peripheral VMs underwent contrast-enhanced magnetic resonance imaging. Hematologic monitoring for localized intravascular coagulopathy was performed in all. Perioperative anticoagulation was administered accordingly. When applicable, venous duplex ultrasound was performed to assess for presence and patency of a deep venous system and superficial venous reflux. If superficial venous reflux was identified, radiofrequency ablation was performed per standard protocol before or at the time of initial embolization. Direct-stick embolizations (DSEs) were performed by a single operator using two concentrations (1% and 3%) of sodium tetradecyl sulfate (STS; Sotradecol; AngioDynamics, Latham, NY) without foam preparation. Patients were followed up clinically for resolution of symptoms, coagulopathic monitoring, and development of complications. All data were prospectively maintained and retrospectively reviewed. RESULTS: There were 71 DSEs performed in 40 patients (1.8 procedures per patient [range, 1-8]; 12 male patients; mean age, 22 years [range, 2-53 years]). Mean follow-up was 17.1 months (range, 0.8-31.6 months). Presenting symptoms included pain (n = 40 [100%]), swelling (n = 36 [90%]), and cosmetic disfigurement (n = 32 [80%]). Anatomic distribution was upper extremity (n = 16 [23%]), lower extremity (n = 37 [52%]), head and neck (n = 7 [10%]), trunk (n = 10 [14%]), and visceral (n = 1 [1%]). There were 33 sporadic cases, 4 (10%) Klippel-Trenaunay syndrome cases, 2 (5%) blue rubber bleb nevus syndrome cases, and 1 (2.5%) CLOVES (congenital lipomatous overgrowth, vascular malformations, epidermal nevus, and skeletal deformities) syndrome case. Four patients presented with localized intravascular coagulopathy, two of whom required perioperative enoxaparin. Twenty-six patients (65%) required a single DSE session with complete symptom relief. Fourteen patients (35%) required repeated DSE. Two patients (5%) required adjunctive surgical excision. There was one postoperative death (1.4%) secondary to massive pulmonary embolism. Complications were otherwise limited to skin necrosis (n = 2 [3%]). Mean volume of sclerosant per session was 7 mL of 1% STS (range, 3-14 mL), and 15 mL of 3% STS (range, 3-42.5 mL). CONCLUSIONS: In the absence of allergic reactions, most congenital peripheral VMs can be safely embolized with liquid STS, thereby avoiding the well-documented toxicity of ethanol. Venous thromboembolism remains a major source of morbidity and mortality in this population of patients despite close hematologic scrutiny. Prospective randomized trials are needed for embolotherapeutic standardization.
Nikolaev, S. I., et al. (2018). “Somatic activating KRAS mutations in arteriovenous malformations of the brain.” N Engl J Med 378(3): 250–261.
BACKGROUND: Sporadic arteriovenous malformations of the brain, which are morphologically abnormal connections between arteries and veins in the brain vasculature, are a leading cause of hemorrhagic stroke in young adults and children. The genetic cause of this rare focal disorder is unknown. METHODS: We analyzed tissue and blood samples from patients with arteriovenous malformations of the brain to detect somatic mutations. We performed exome DNA sequencing of tissue samples of arteriovenous malformations of the brain from 26 patients in the main study group and of paired blood samples from 17 of those patients. To confirm our findings, we performed droplet digital polymerase-chain-reaction (PCR) analysis of tissue samples from 39 patients in the main study group (21 with matching blood samples) and from 33 patients in an independent validation group. We interrogated the downstream signaling pathways, changes in gene expression, and cellular phenotype that were induced by activating KRAS mutations, which we had discovered in tissue samples. RESULTS: We detected somatic activating KRAS mutations in tissue samples from 45 of the 72 patients and in none of the 21 paired blood samples. In endothelial cell-enriched cultures derived from arteriovenous malformations of the brain, we detected KRAS mutations and observed that expression of mutant KRAS (KRAS(G12V)) in endothelial cells in vitro induced increased ERK (extracellular signal-regulated kinase) activity, increased expression of genes related to angiogenesis and Notch signaling, and enhanced migratory behavior. These processes were reversed by inhibition of MAPK (mitogen-activated protein kinase)-ERK signaling. CONCLUSIONS: We identified activating KRAS mutations in the majority of tissue samples of arteriovenous malformations of the brain that we analyzed. We propose that these malformations develop as a result of KRAS-induced activation of the MAPK-ERK signaling pathway in brain endothelial cells. (Funded by the Swiss Cancer League and others.).
Parambil, J. G., et al. (2018). “Pazopanib effective for bevacizumab-unresponsive epistaxis in hereditary hemorrhagic telangiectasia.” Laryngoscope. [EPub Feb 16]
Hereditary hemorrhagic telangiectasia (HHT) most commonly manifests with nasal mucosal telangiectasias, and vascular endothelial growth factor (VEGF) plays a significant role in this angiodysplasia. We describe a patient with HHT with epistaxis recalcitrant to several endonasal procedures and six cycles of intravenous bevacizumab, for which he was dependent on iron infusions and packed red blood cells transfusions. He then started pazopanib at 100 mg with dramatic improvements in epistaxis and normalization of hemoglobin and iron levels, without replenishment needs for 12 months. This is the first report on the efficacy of pazopanib with high selectivity for abrogating VEGF receptor-2 signaling in HHT, and needs to be explored further. Laryngoscope, 2018.
Park, S. M., et al. (2017). “5q14.3 microdeletions: A contiguous gene syndrome with capillary malformation-arteriovenous malformation syndrome and neurologic findings.” Pediatr Dermatol 34(2): 156–159.
Deletions within chromosome region 5q14.3q15 have been associated with a spectrum of disorders including developmental delay, hypotonia, absent speech, mild facial dysmorphism, seizures, and brain anomalies. Some cases of concomitant neurologic abnormalities and cutaneous vascular malformation associated with 5q14.3 deletion have been reported. Previously reported cases had similar features, including multiple capillary malformations, and neurologic abnormalities, including epilepsy, hypotonia, and developmental delay. We report a case of 5q14.3 neurocutaneous syndrome presenting with multiple capillary malformations, neurologic abnormalities, and microdeletion in chromosome 5q14.3.
Petrovic, J., et al. (2017). “Oral propranolol for infantile hemangiomas: A prospective study on the role of 48-hour Holter monitoring in additional safety assessment.” J Dermatolog Treat 28(6): 554–558.
PURPOSE: Oral propranolol has been recently approved for infantile hemangiomas (IHs), but potential side effects stay a challenge. We sought to make an additional assessment on oral propranolol safety for this indication. MATERIALS AND METHODS: Prospective study included 108 infants consecutively treated for IHs at the University Children's Hospital Tirsova, Belgrade from January 2010 to December 2013. Propranolol was administered orally at a daily dose of 0.5 mg/kg and doubled every 48 hours in the absence of side effects until reaching the maximum dose of 2 mg/kg daily. Systolic and diastolic blood pressure and heart rate were measured every 48 hours with clinical observation. Heart rate was monitored by standard electrocardiogram (ECG) and 48-hour Holter ECG. RESULTS: Statistically significant, but asymptomatic decreases in systolic blood pressure and heart rate recorded by Holter ECG were observed during the first doubling of dose and then remained stable. Arrhythmias were not detected. Despite mild sleep disturbance observed in 31% of infants in the hospital milieu, Holter monitoring indicated circadian rhythm maintenance. CONCLUSIONS: Oral propranolol for IHs does not remarkably affect heart rhythm including circadian variations throughout hospital initiation. Therefore, there is no necessity for Holter monitoring in additional safety assessment.
Pinto, R. S., et al. (2018). “Surgical trauma induces overgrowth in lower limb gigantism: Regulation with use of rapamycin is promising.” BMJ Case Rep 2018. [EPub Jan 4]
We describe an unclassified overgrowth syndrome characterised by unregulated growth of dermal fibroblasts in the lower limbs of a 35-year-old woman. A PIK3CA gene mutation resulted in lower limb gigantism. Below the waist, she weighed 117 kg with each leg measuring over 100 cm in circumference. Her total adiposity was 50% accounted for by her legs mainly. Liposuction and surgical debulking were performed to reduce the size of the limbs but had exacerbated the overgrowth in her lower limbs. Systemic sepsis from an infected foot ulcer necessitated treatment by an above-knee amputation. Postoperatively, the stump increased in size by 19 kg. A trial of rapamycin to reverse the growth of the stump has shown promise. We discuss the clinical and genetic features of this previously unclassified disorder and the orthopaedic considerations involved.
Robard, L., et al. (2017). “Guidelines of the French Society of Otorhinolaryngology (SFORL) (short version). Specific treatment of epistaxis in Rendu-Osler-Weber disease.” Eur Ann Otorhinolaryngol Head Neck Dis 134(1): 37–41.
OBJECTIVES: The authors present the guidelines of the French Oto-Rhino-Laryngology - Head and Neck Surgery Society (Societe Francaise d'Oto-Rhino-Laryngologie et de Chirurgie de la Face et du Cou: SFORL) concerning specific treatment of epistaxis in Rendu-Osler-Weber disease. METHODS: A multidisciplinary work-group was entrusted with a review of the scientific literature on the above topic. Guidelines were drawn up, based on the articles retrieved and the group members' individual experience. They were then read over by an editorial group independent of the work group. The final version was established in a coordination meeting. The guidelines were graded as A, B, C or expert opinion, by decreasing level of evidence. RESULTS: Rendu-Osler-Weber disease is diagnosed from the presence of at least three of Curacao's four criteria. In acute epistaxis, bidigital compression is recommended. Embolization is reserved for resistant epistaxis. Non-resorbable nasal packing and cauterization are contraindicated. Patient education is essential. Telangiectasia of the nasal mucosa can be treated by various local means. In the event of insufficient control, systemic administration of tranexamic acid is recommended.
Rodriguez-Laguna, L., et al. (2018). “CLAPO syndrome: identification of somatic activating PIK3CA mutations and delineation of the natural history and phenotype.” Genet Med. [EPub Feb 15]
PurposeCLAPO syndrome is a rare vascular disorder characterized by capillary malformation of the lower lip, lymphatic malformation predominant on the face and neck, asymmetry, and partial/generalized overgrowth. Here we tested the hypothesis that, although the genetic cause is not known, the tissue distribution of the clinical manifestations in CLAPO seems to follow a pattern of somatic mosaicism.MethodsWe clinically evaluated a cohort of 13 patients with CLAPO and screened 20 DNA blood/tissue samples from 9 patients using high-throughput, deep sequencing.ResultsWe identified five activating mutations in the PIK3CA gene in affected tissues from 6 of the 9 patients studied; one of the variants (NM_006218.2:c.248T>C; p.Phe83Ser) has not been previously described in developmental disorders.ConclusionWe describe for the first time the presence of somatic activating PIK3CA mutations in patients with CLAPO. We also report an update of the phenotype and natural history of the syndrome. GENETICS in MEDICINE advance online publication, 15 February 2018; doi:10.1038/gim.2017.200.
Shimura, M., et al. (2018). “Predicting the intrauterine fetal death of fetuses with cystic hygroma in early pregnancy.” Congenit Anom (Kyoto). [EPub Jan 11]
We investigated whether it was possible to predict the prognosis of fetuses with cystic hygroma in early pregnancy based on the degree of neck thickening. We retrospectively analyzed 57 singleton pregnancies with fetuses with cystic hygroma who were examined before the 22nd week of pregnancy. The fetuses were categorized according to the outcome, structural abnormalities at birth, and chromosomal abnormalities. Here, we proposed a new sonographic predictor with which we assessed neck thickening by dividing the width of the neck thickening by the biparietal diameter, which is expressed as the cystic hygroma width/biparietal diameter ratio. The median cystic hygroma width/biparietal diameter ratio in the intrauterine fetal death group (0.51) was significantly higher than that in the live birth group (0.27). No significant difference in the median cystic hygroma width/biparietal diameter ratio was found between the structural abnormalities group at birth and the no structural abnormalities group, and no significant difference in the median cystic hygroma width/biparietal diameter ratio was found between the chromosomal abnormality group and the no chromosomal abnormality group. We used receiver operating characteristic analysis to evaluate the cystic hygroma width/biparietal diameter ratio to predict intrauterine fetal death. When the cystic hygroma width/biparietal diameter ratio cut-off value was 0.5, intrauterine fetal death could be predicted with a sensitivity of 52.9% and a specificity of 100%. It is possible to predict intrauterine fetal death in fetuses with cystic hygroma in early pregnancy if cystic hygroma width/biparietal diameter ratio is measured. However, even if cystic hygroma width/biparietal diameter ratio is measured, predicting the presence or absence of a structural abnormality at birth or a chromosomal abnormality is difficult.
Steiner, J. E., et al. (2018). “Scarring in patients with PIK3CA-related overgrowth syndromes.” JAMA Dermatol. [EPub Mar 7]
Importance: Patients with somatic overgrowth commonly require surgical intervention to preserve function and improve cosmesis. To our knowledge no observation of scarring outcomes in this population has been published to date. Objective: To observe the frequency of abnormal scarring in patients with somatic overgrowth and sequencing-verified mutations in the PIK3CA gene. Design, Setting, and Participants: This retrospective study evaluated scarring outcomes in patients with PIK3CA-related overgrowth. Samples of affected tissue were sequenced between July 2015 and October 2016. Medical records from multiple large academic tertiary care centers were reviewed for surgical history and scar descriptions, and clinical photographs were assessed by 2 surgeons (J.N.J. and D.M.K.) to confirm abnormal scarring. Analysis of medical records and photographs was performed between April 2017 and June 2017 by a multidisciplinary team from dermatology, plastic surgery, orthopedic surgery, radiology, and genetics departments. All patients considered for the study were diagnosed with somatic overgrowth and previously had affected tissue sent for next-generation sequencing. Those with pathogenic PIK3CA variants and 1 or more prior surgical procedures were reviewed. Main Outcomes and Measures: Presence of excessive scarring in patients with PIK3CA overgrowth. Results: A total of 57 patients with segmental overgrowth syndromes were sequenced. Of the 57 patients, 25 (44%) had pathogenic or likely pathogenic variants in PIK3CA. Of those with pathogenic PIK3CA variants, 6 (24%) had past surgical procedures, all with preoperative and postoperative photographs. Of 6 patients with PIK3CA-related overgrowth and a history of 1 or more surgical procedure, 4 (67%) developed excessive scarring. The cohort with abnormal scarring comprised 3 females and 1 male, with a median age of 8.5 years. All abnormal scarring occurred in affected overgrowth tissue. Three of the 4 patients developed the excessive scarring after debulking procedures for overgrowth and/or vascular malformations of the upper or lower extremity. Conclusions and Relevance: Excessive scarring occurred frequently in patients with PIK3CA-related overgrowth syndromes. The risk of abnormal scarring should therefore be discussed preoperatively. Given the activating nature of these PIK3CA variants, we suggest that the excessive scarring may be owing in part to up-regulation of the PI3K-Akt-mTOR pathway. Additional studies are needed to assess scarring outcomes in patients with other types of overgrowth.
Tan, A. P. and W. K. Chong (2018). “A child with Apert syndrome and Sturge-Weber syndrome: could fibronectin or the RAS/MAPK signaling pathway be the connection?” Childs Nerv Syst. [EPub Feb 23]
BACKGROUND: Apert syndrome is one of the most common craniosynostosis syndrome caused by mutation in genes encoding fibroblast growth factor receptor 2 (FGFR2). Craniosynostosis, midfacial hypoplasia, and syndactyly/symphalangism are features of this syndrome. Sturge-Weber syndrome (SWS) on the other hand is a congenital neurocutaneous disorder characterized by facial port-wine stains (PWSs) and leptomeningeal vascular capillary malformations. In 2013, the causative mutation underlying SWS (p.R183Q somatic activating mutation in the guanine nucleotide-binding protein alpha-q (GNAQ) gene) was identified. This mutation increases downstream signaling along the RAS/MAPK pathway, resulting in increased cell proliferation. The interaction between FGFR and the RAS/MAPK signaling pathway was proposed in recent years. Elevated synthesis of fibronectin in the calvaria of patients with Apert syndrome and increased fibronectin gene expression in port wine-derived fibroblasts of patients with Sturge-Weber disease have also been reported. CASE PRESENTATION: We report a unique case of Apert and Sturge-Weber syndromes occurring in the same patient. The child was noted to demonstrate features suggestive of Apert syndrome at birth, including brachycephaly, midface hypoplasia, and syndactyly. In addition, a left-sided facial port wine stain in the forehead was noted. Magnetic resonance imaging (MRI) of the brain was performed and confirmed the diagnosis of Sturge-Weber syndrome by demonstrating the presence of left sided leptomeningeal vascular capillary malformation and left-sided cerebral hemiatrophy. CONCLUSION: To the best of our knowledge, there has been no prior described case of Apert and Sturge-Weber syndromes occurring in the same patient. This case report identifies an area of potential research on fibronectin and derangement of the RAS/MAPK signaling pathway in relation to Apert syndrome and Sturge-Weber syndrome. In view of the rare concurrence of Apert and Sturge-Weber syndromes, the underlying pathogenesis is thought to be multifactorial, one of which may be related to either increased fibronectin gene expression or derangement of the RAS/MAPK signaling pathway.
Ueno, S., et al. (2018). “Treatment of mediastinal lymphatic malformation in children: An analysis of a nationwide survey in Japan.” Surg Today. [EPub Feb 26]
PURPOSE: Clinical guidelines on lymphatic malformation (LM) influencing the airway have been crafted in the Research Project for Intractable Diseases. We herein report an analysis of a nationwide survey of mediastinal LM and the therapeutic recommendations. METHODS: Eighty-seven registered cases with mediastinal involvement were analyzed with a review of the literature. RESULTS: Mediastinal LM was located more often in the upper and anterior mediastinum and was found without any accompanying symptoms in 56/87 cases. Tracheostomy was required in 23/87 cases, mostly <2 years of age (87%). All patients who needed tracheostomy had a lesion in contact with the airway, while only 55% of those without tracheostomy had contact. Tracheostomy tended to be placed more when the longer segment of the airway was in contact with the LM. Multimodal treatments were performed in 29 patients, but the lesions remained in most cases, and chylothorax, hemorrhaging, nerve palsy, and infections were noted as complications. CONCLUSIONS: In patients with mediastinal LM, tracheostomy may be necessary, especially when the lesion is extensive and contacts the airway. Extirpation of the mediastinal LM may be the only therapeutic option, but in cases with few or no symptoms, non-surgical treatment should be considered in light of potential postoperative complications.
Unolt, M., et al. (2018). “Primary lymphedema and other lymphatic anomalies are associated with 22q11.2 deletion syndrome.” Eur J Med Genet. [EPub Feb 12]
BACKGROUND: Lymphedema is an abnormal accumulation of interstitial fluid within the tissues. Primary lymphedema is caused by aberrant lymphangiogenesis and it has been historically classified based on age at presentation. Although most cases are sporadic, primary lymphedema may be familial or present in association with chromosomal abnormalities and syndromic disorders. To the best of our knowledge, primary lymphedema has never been described in patients with 22q11.2 deletion syndrome. METHODS AND RESULTS: We identified 4 patients with 22q11.2 deletion syndrome and primary lymphedema via our International 22q11.2 Deletion Syndrome Consortium. All patients underwent comprehensive clinical, laboratory and imaging assessments to rule out other causes of lymphedema. All patients had de novo typical deletions and family histories were negative for lymphedema. CONCLUSIONS: We report the novel association of primary lymphedema with 22q11.2 deletion syndrome. Importantly, animal models demonstrated Tbx1 playing a critical role in lymphangiogenesis by reducing Vegfr3 expression in lymphatic endothelial cells. Moreover, the VEGFR3 pathway is essential for lymphangiogenesis with mutations identified in hereditary primary lymphedema. Accordingly, our findings provide a new insight into understanding cellular mechanisms of lymphangiogenesis disorders.
Vivanti, A., et al. (2018). “Loss of function mutations in EPHB4 are responsible for vein of Galen aneurysmal malformation.” Brain. [EPub Feb 9]
Vein of Galen aneurysmal malformation is a congenital anomaly of the cerebral vasculature representing 30% of all paediatric vascular malformations. We conducted whole exome sequencing in 19 unrelated patients presenting this malformation and subsequently screened candidate genes in a cohort of 32 additional patients using either targeted exome or Sanger sequencing. In a cohort of 51 patients, we found five affected individuals with heterozygous mutations in EPHB4 including de novo frameshift (p.His191Alafs*32) or inherited deleterious splice or missense mutations predicted to be pathogenic by in silico tools. Knockdown of ephb4 in zebrafish embryos leads to specific anomalies of dorsal cranial vessels including the dorsal longitudinal vein, which is the orthologue of the median prosencephalic vein and the embryonic precursor of the vein of Galen. This model allowed us to investigate EPHB4 loss-of-function mutations in this disease by the ability to rescue the brain vascular defect in knockdown zebrafish co-injected with wild-type, but not truncated EPHB4, mimicking the p.His191Alafs mutation. Our data showed that in both species, loss of function mutations of EPHB4 result in specific and similar brain vascular development anomalies. Recently, EPHB4 germline mutations have been reported in non-immune hydrops fetalis and in cutaneous capillary malformation-arteriovenous malformation. Here, we show that EPHB4 mutations are also responsible for vein of Galen aneurysmal malformation, indicating that heterozygous germline mutations of EPHB4 result in a large clinical spectrum. The identification of EPHB4 pathogenic mutations in patients presenting capillary malformation or vein of Galen aneurysmal malformation should lead to careful follow-up of pregnancy of carriers for early detection of anomaly of the cerebral vasculature in order to propose optimal neonatal care. Endovascular embolization indeed greatly improved the prognosis of patients.
Waelti, S. L., et al. (2018). “Ultrasound findings in rapidly involuting congenital hemangioma (RICH) - beware of venous ectasia and venous lakes.” Pediatr Radiol 48(4): 586–593.
BACKGROUND: Bleeding, ulceration and cardiac failure can occur in rapidly involuting congenital hemangioma (RICH). Bleeding intensity ranges from superficial to life-threatening. OBJECTIVE: To determine whether there are sonographic criteria associated with an increased risk of bleeding, ulceration or cardiac failure in RICH in order to identify children who need close monitoring or prophylactic treatment. MATERIALS AND METHODS: This retrospective single-center study included RICH patients over a period of 13 years. We evaluated sonographic features of RICH on B-mode and Doppler ultrasound. We correlated the occurrence of bleeding, ulceration and cardiac failure with four sonographic findings: (1) visible vessel, (2) venous ectasia, (3) venous lake and (4) arteriovenous shunting. RESULTS: We included 24 patients. Ulceration occurred in five cases, bleeding in four cases, one of which was life-threatening. Cardiac failure was observed more frequently in RICH with venous lakes (P = 0.028). Bleeding and ulceration appeared more frequently in RICH with venous ectasia and venous lakes. Cardiac failure was associated with the presence of venous ectasia. All children with cardiac failure or ulceration had arteriovenous shunts. CONCLUSION: RICH with venous lakes on ultrasound is prone to develop bleeding, cardiac failure and ulceration. This association was only significant for cardiac failure.
Wright, J. N. and V. Wycoco (2017). “Asymmetric Meckel cave enlargement: A potential marker of PHACES Syndrome.” AJNR Am J Neuroradiol 38(6): 1223–1227.
BACKGROUND AND PURPOSE: PHACES syndrome is a complex of morphologic abnormalities of unknown cause and includes posterior fossa abnormalities; head and neck infantile hemangiomas; arterial, cardiac, and eye anomalies; and sternal or abdominal wall defects. Accurate identification of the syndrome is important for optimal treatment. The purpose of this study was to investigate the incidence of asymmetric Meckel cave enlargement, a potential novel imaging marker, in a population of patients referred for evaluation of possible PHACES syndrome. MATERIALS AND METHODS: Eighty-five patients referred for neuroimaging evaluation of possible PHACES syndrome were identified and stratified on the basis of their ultimate clinical PHACES diagnosis categorization into PHACES, possible PHACES, or not PHACES. MR imaging studies were subsequently reviewed for the presence or absence of unilateral Meckel cave enlargement, with the reviewer blinded to the ultimate PHACES syndrome categorization. RESULTS: Twenty-five of 85 patients (29%) were ultimately categorized as having PHACES or possible PHACES according to consensus guidelines. Asymmetric Meckel cave enlargement was present in 76% (19/25) of these patients and in 82% (19/23) of only those patients with definite PHACES. This finding was present in none of the 60 patients determined not to have PHACES syndrome. In 7/19 patients (37%) with this finding, subtle MR imaging abnormalities consistent with PHACES were missed on the initial MR imaging interpretation. CONCLUSIONS: Asymmetric Meckel cave enlargement was a common feature of patients with PHACES in our cohort and may serve as a novel imaging marker. Increased awareness of this imaging feature has the potential to increase the diagnostic accuracy of PHACES.
Yuan, S. M., et al. (2017). “Over-expression of PPAR-gamma2 gene enhances the adipogenic differentiation of hemangioma-derived mesenchymal stem cells in vitro and in vivo.” Oncotarget 8(70): 115817–115828.
Background: Most of infantile hemangiomas involute into fibrofatty tissue in childhood, which indicates adipogenesis during this period. Mesenchymal stem cells (MSCs) contribute to the adipogenesis in IH. In this study, we investigated the effects of overexpression of PPAR-gamma2 gene on the adipogenic differentiation of Hemangioma-derived MSCs (Hem-MSCs), and discussed the possibility of targeted therapy via PPAR-gamma pathway. Methods: MSCs were isolated from proliferating hemangioma by their selective adhesion to plastic culture dishes. Recombinant lentivirus with PPAR-gamma2 gene were prepared, and used to transfect Hem-MSCs. Transfected cells were cultured in adipogenic medium to observe the differentiation in vitro. And the cells were mixed with Matrigel, then subcutaneously injected into the back of nude mice to observe the differentiation in vivo. Results: In the in vitro tests, Hem-MSCs with overexpression of PPAR-gamma2 gene showed enhanced adipogenic differentiation with increased expression of adipogenic-related genes, including PPAR-gamma2, ADD1, LPL, and CEBPA genes. In the in vivo tests, Hem-MSCs/Matrigel plugs with overexpression of PPAR-gamma2 gene also showed accelerated adipogenesis and time-phased changes of above genes. Conclusions: Overexpression of PPAR-gamma2 gene enhances and accelerates the adipogenic differentiation of Hem-MSCs in vitro and in vivo. The results may provide the preliminary evidences for the targeted therapy of IH via PPAR-gamma signal pathway.
Zhang, G., et al. (2018). “Sirolimus for treatment of Kaposiform hemangioendothelioma with Kasabach-Merritt phenomenon: A retrospective cohort study.” Br J Dermatol. [EPub Feb 1]
Kaposiform hemangioendothelima (KHE) is a locally aggressive vascular tumor that mainly occurs during childhood and invades adjacent tissue and organ. It is commonly complicated by Kasabach-Merritt phenomenon (KMP) in about 50%-70% of the cases. KMP is most often associated with a rapidly growing, large solitary tumor that may result in severe hemorrhage and directly responsible for high mortality and morbidity. This article is protected by copyright. All rights reserved.
Zhao, H., et al. (2016). “Dysregulated exocytosis of angiopoietin-2 drives cerebral cavernous malformation.” Nat Med 22(9): 971–973.
Zheng, L. and Y. Li (2018). “Effect of topical timolol on response rate and adverse events in infantile hemangioma: A meta-analysis.” Arch Dermatol Res. [EPub Jan 23]
A number of clinical trials evaluated the effect of topical timolol in the treatment of infantile hemangioma and provided inconsistent results. The present study assessed the response rate and adverse events of topical timolol in the treatment of infantile hemangioma. Pubmed, Embase, China National Knowledge Infrastructure (CNKI), Wanfang, and Cochrane library were searched until October 2016. Specific inclusion criteria were used to evaluate articles. Risk ratios (RRs) with 95% confidence intervals (CIs) were calculated. The meta-analysis was performed using a random effect model. A total of 10 studies, comprising 887 infants with hemangioma, were included. The response rate was reported in eight trials; these studies compared the topical timolol to laser, observation, placebo, or propranolol. The heterogeneity was statistically significant (P < 0.00001, I(2) = 83%). The difference in the response rate was significant (RR = 2.86, 95% CI 1.31-6.24) while comparing the topical timolol to the controls. However, no significant difference in the response rate was observed while comparing the topical timolol to propranolol (RR = 0.99, 95% CI 0.70-1.42). The difference in the adverse events was found to be significant (RR = 0.21, 95% CI 0.05-0.97) when the timolol group was compared to the control group. This meta-analysis confirmed that the topical timolol alone was more beneficial on response rate and adverse event than laser, placebo, and observation. The response rate did not differ significantly when comparing the topical timolol to propranolol. However, further studies are essential using an improved design of the study.
Zhu, X., et al. (2017). “Promotion of propranolol delivery to hemangiomas by using anti-VEGFR antibody-conjugated poly(lactic-co-glycolic acid) nanoparticles.” J Biomed Nanotechnol 13(12): 1694–1705.
Infantile hemangiomas are the most common tumors affecting children. Although infantile hemangiomas are benign, they could result in morbidity and mortality. The only US Food and Drug Administration-approved drug for infantile hemangiomas is propranolol hydrochloride (Hemangeol); however, its adverse effects and high frequency of administration hamper its clinical application. Vascular endothelial growth factor receptor (VEGFR) is crucial to the angiogenesis of infantile hemangiomas, and thus it is considered a valuable therapeutic target for infantile hemangiomas. To reduce the adverse effects and high administration frequency of propranolol, we developed propranolol-loaded nanoparticles conjugated with anti-VEGFR antibody (PNP-VEGFR) as a controlled- and targeted-release system to treat infantile hemangiomas. The characteristics, anti-hemangioma activity, and mechanisms of PNP-VEGFR were examined in vitro and in vivo. The developed PNP-VEGFR exhibited a small size (approximately 100 nm), drug encapsulation efficiency (approximately 60%), and sustained drug release for 8 days. PNP-VEGFR was efficiently bound to human umbilical vein endothelial cells and human hemangioma endothelial cells in a VEGFR-dependent manner, resulting in enhanced cytotoxic effects and stronger inhibition of VEGF expression, compared to that of the untargeted propranolol-loaded nanoparticles (PNP) and propranolol. Notably, the in vivo therapeutic effects of PNP-VEGFR in infantile hemangiomas were superior to that of propranolol and PNP, as reflected by significantly reduced hemangioma volume, weight, and microvessel density, without any noticeable behavioral changes or weight loss. PNP-VEGFR was shown to provide targeted delivery and sustained release of propranolol to infantile hemangiomas. Therefore, it represents a promising treatment for infantile hemangiomas.
Zhu, X., et al. (2018). “Significant inhibition of infantile hemangioma growth by sustained delivery of urea from liposomes-in-microspheres.” Oncol Rep 39(1): 109–118.
Infantile hemangioma (IH) is a benign pediatric tumor, and rapid growth of IH can result in serious morbidity and even mortality. Only one drug Hemangeol (propranolol hydrochloride oral solution) has been approved for the treatment of IH, whereas patients suffer from its adverse effects and high frequency of administration. We have used urea, an organic compound and a normal body metabolite, in the treatment of IH for 20 years, and demonstrated that urea is an effective and well-tolerated treatment for IH. To reduce the daily administration of urea, we firstly utilized urea-loaded liposomes-in-microspheres (ULIM) as a novel topical controlled release system to realize the sustained release of urea. ULIM were fabricated from the encapsulation of urea-loaded liposomes in poly(lactic-co-glycolic acid)-b-poly(ethylene glycol)-b-poly(lactic-co-glycolic acid) microspheres. The characteristics, activity and mechanism against IH of ULIM were examined in vitro and in vivo. ULIM were of a desired particle size (∼62.4 microm), drug encapsulation efficiency (∼51.5%) and sustained drug release for 40 days. ULIM inhibited the proliferation of hemangioma endothelia cells (HemECs) and expression of vascular endothelial growth factor-A in HemECs. The therapeutic effect of ULIM in IH was better than propranolol, urea, urea-loaded liposomes and urea-loaded microspheres in vivo, as reflected by markedly decreased hemangioma weight, volume and microvessel density. None of the treated mice showed behavioral changes, severe sideeffects and weight loss. Our results suggest that use of ULIM is a potential and safe approach with which to locally and efficiently deliver urea to hemangioma, and is a promising alternative to propranolol in the treatment of IH.