
Abstract
Background:
Early lymphedema detection may reduce the symptoms and improve clinical outcomes. However, the lack of reliable serum biomarkers capable of predicting lymphedema development is a current medical problem. In this study, we investigated if serum levels of hyaluronic acid (HA) and leukotriene B4 (LTB4), two molecules involved in lymphedema development, may work as predictors of this condition.
Methods and Results:
A mouse model of acquired lymphedema was generated through ablation of tail dermal lymphatic network. Tail diameter was measured daily, and HA and LTB4 serum levels were analyzed before and during the development of lymphedema. We found increased serum levels of HA and reduced levels of LTB4 at early days before the appearance of lymphedema signs. Similar results were observed in the lymphedema tissue. Increased local and systemic inflammation was also detected at early time points. Moreover, the ratio LTB4/HA arises as the strongest predictor for lymphedema development. In fact, we found an inverse correlation in our model, where reduced LTB4/HA levels showed increased lymphedema signs.
Conclusions:
These findings suggest that serum ratio of LTB4/HA may be a useful biomarker to predict acquired lymphedema development, with potential to be used in clinical conditions such as breast cancer patients.
Introduction
Lymphedema is a progressive clinical condition generated by lymphatic dysfunction with the concomitant accumulation of interstitial fluid, called lymph, that leads to edema and fibrosis of the affected region, with subsequent functional problems, swelling, chronic pain, recurrent infection, and overall decreasing the quality of life. 1 Lymphedema is subdivided in primary lymphedema, which occurs less frequently and usually due to congenital or inherited condition, and secondary lymphedema, more common and triggered by an acquired damage that occurs after surgical lymph node dissection for malignant diseases, including breast cancer. Incidence of secondary lymphedema associated with cancer survivors varies according to the type of cancer; going from melanoma patients (9%–13%), breast cancer (9%–30%) to vulval cancer (28.8%).2–4 Despite the importance of early detection to achieve favorable outcomes in lymphedema treatment, the current detection methods include arm circumference measurement, water displacement, and bioimpedance spectroscopy or perometry. All these methods are based in the detection of clinical signs and when subclinical lymphedema has already occurred, which leads to poor clinical outcomes.5–8 In recent years, several efforts, including the use of indocyanine green lymphography, subcutaneous ultrasound, or machine learning methods, have been developed to improve early lymphedema detection, but the search of new methods based on reliable biomarkers remains challenging.9–11
Hyaluronic acid (HA) is an anionic, nonsulfated glycosaminoglycan and one of the major components of the extracellular matrix. HA is transported by the lymph, and defects in the lymph transport, as observed in lymphedema, promote HA accumulation in the lymphedematous limb.12,13 The role of HA in promoting lymphedema development has been recently addressed. 14 Using a mouse model of secondary lymphedema, Roh et al. showed that repeated injections of hyaluronidase, enzyme that catalyzes the degradation of HA, alleviate swollen tissue, promoting lymphangiogenesis on the lymphedematous limb. 14 To evaluate the mechanism used by HA to aggravate lymphedema, Cho et al. evaluated the immune cell response in the lymphedematous limb with or without hyaluronidase treatment. 15 They found that hyaluronidase treatment reduces interleukin (IL)-6, but increases IL-12 and interferon-γ, two cytokines involved in T-helper 1 cell response that counteracts fibrosis, suggesting that HA mediates lymphedema damage, in part, by modulating immune cell responses and promoting fibrosis. 15 Despite the importance of HA in lymphedema development, its role as predictor of secondary lymphedema development has not been yet addressed.
Leukotriene B4 (LTB4) is a pro-inflammatory lipid molecule generated as an end product of the leukotriene biosynthetic pathway. LTB4 can be produced by activated leukocytes, working as a potent chemoattractant for neutrophils and stimulating the production of pro-inflammatory cytokines.16–18 The role of LTB4 in lymphedema has been explored by a recent seminal work showing that LTB4 antagonism reversed edema and improved lymphatic function in a murine model of lymphedema. 19 In this work, using specific LTB4 antagonist, Tian et al. found improved lymphatic clearance, diminished tissue inflammation, and improved tail anatomy. 19 LTB4, however, has a bimodal function; lower LTB4 levels, such as those seen in the lymphedematous tail at early days, promote lymphatic repair, but higher LTB4 levels work as an antilymphangiogenic agent, in part, by inhibiting Vascular endothelial growth factor receptor 3 and Notch pathways. 19 In line with these results, a recent work has shown that the use of ketoprofen, a strong LTB4 inhibitor, improves cutaneous pathology and skin thickness in human lymphedema, suggesting the potential use of ketoprofen or other anti-inflammatory agents to treat human lymphedema. 20 All these results highlight the importance of LTB4 in the different phases of lymphedema development, but if serum LTB4 levels can work as a biomarker to predict lymphedema development remains to be evaluated.
In this study, we evaluated if serum HA and LTB4 can work as serum biomarkers to predict the development of lymphedema in a mouse model of acquired lymphedema. Our results suggest that the ratio LTB4/HA is a good predictor of lymphedema development with potential in clinical diagnostics.
Materials and Methods
Mice
Eight- to 12-week-old C57BL/6 mice were obtained from The Jackson Laboratory (Bar Harbor, ME). Animals were housed in temperature- and humidity-controlled rooms, maintained on a 12-h light/12-h dark cycle (lights on at 7:00 hours). All animal procedures were performed according to animal protocols approved by the Institutional Animal Care and Use Committee at Universidad Autónoma de Chile.
Mouse model of tail lymphedema
Acquired lymphedema was surgically induced in the tails of C57BL/6 mice by thermal ablation of lymphatic trunks (Lymphedema) under anesthesia by inhalation of isoflurane, as previously described. 21 Briefly, a full-thickness circumferential incision of the skin was made 15 mm distal to the base of the mouse tail. Lymphatic trunks were ablated through controlled limited cautery application. For surgical control, the skin incision alone was performed without lymphatic cautery (Sham). Mice were daily monitored and photographed to record the lymphedema progression. Animals were euthanized at different time points until day 26 after surgery and analyzed as outlined below.
Tail thickness measurement and histological analysis
Tail diameter of the lymphedematous site was measured using multiple caliper tail circumference measurements at the point exactly 5 mm distal to the incision site, and the truncated cone formula was used as previously described.21,22 Lymphedema severity (score) was calculated as the number of days that take lymphedema to resolve/day that clinical signs appear. At the end of the follow-up, mice were euthanized, and their tails were obtained, sliced, fixed in 4% ice-cold paraformaldehyde overnight (Sigma-Aldrich, St. Louis, MO), and decalcified using 3% EDTA (Loba Chemie Pvt Ltd., Mumbai, India) for 3 weeks, under gentle agitation on a shaker. Fixed samples were then washed in phosphate-buffered saline (PBS) and treated with 15% sucrose in PBS for 5 hours, followed by 30% sucrose overnight. Next day, tissues were embedded in Tissue-Tek OCT (Sakura Finetek, Torrance, CA) and stored at −20°C before sectioning. Samples were sectioned at 30 μm with a cryostat and processes for immunofluorescence. Briefly, samples were slightly permeabilized in PBS +0.5% Triton X-100 for 30 minutes, blocked with a mix of 5% donkey serum (Jackson ImmunoResearch) +1% bovine serum albumin +0.05% sodium azide and 0.1% Triton X-100 in PBS, and incubated overnight at room temperature with anti-LYVE1-AlexaFluor 488 conjugated antibody (clone 53-0443; eBioscience, San Diego, CA) at 1:250 dilution in PBS +0.1% Triton X-100. Local macrophage infiltration was evaluated by immunofluorescence of the lymphedema area using a mAb against F4/80 (clone BM8; BioLegend, San Diego, CA) followed by a secondary antibody conjugated with Alexa 488 (cat number: A-21208; Invitrogen). Samples were mounted with VECTASHIELD antifade mounting medium with DAPI (Vector Laboratories) and sealed with nail polish. Images were acquired in an Olympus BX51 epifluorescence Microscope (Olympus, Melville, NY). Percentage area of lymphatic vessels was calculated according to the formula: total area of lymphatic vessels/total tissue surface area × 100, from at least 15 randomly selected fields per treatment from two independent experiments, using ImageJ software version 1.46r (NIH, Bethesda, MD).
Enzyme-linked immunosorbent assay analysis
Serum samples were obtained the day before the surgery (day −1) and the days after the treatment (days 1, 2, and 5). For HA detection, the Hyaluronan Quantikine ELISA Kit (R&D Systems, MN) was used according to the manufacturer's instructions. For LTB4 detection, the Leukotriene B4 Multispecies Competitive ELISA Kit (Thermo Fisher Scientific, Waltham, MA) was used according to the manufacturer's instructions. For IL-6 detection, capture mAb: clone MP5-20F3 and detection mAb: clone MP5-32C11 (BioLegend) were used as previously described. 23 Samples were measured in an Autobio PHOmo microplate reader in a blinded manner.
Real-time semiquantitative polymerase chain reaction analysis
For real-time polymerase chain reaction (RT-PCR) analysis, tissues were homogenized in TRIzol reagent according to manufacturer's instructions (Thermo Fisher Scientific). RNA (1 μg) was reverse transcribed using the High Capacity RNA-to-cDNA Kit (Applied Biosystems). Real-time PCR was performed using SYBR Green Real-Time PCR Master Mix (Thermo Fisher Scientific), as described previously, 24 and the expression of each target gene is presented as the fold change relative to the expression of Sham at day 0. Primer sequences used in this study were: LTA4H (forward, 5′-GAGGTCGCGGATACTTGCTC-3′; reverse 5′-CTCCTGTGACTGGACCGTG-3′), 5LO (forward, 5′-TCATTGAGAAGCCAGTGAAGG; reverse 5′-GTTGGGAATCCTGTCTGGTGA-3′), HAS1 (forward, 5′-CTTTCAAGGCACTGGGCGAC-3′,reverse 5′-CACCGCTTCATAGGTCATCC-3′), HAS2 (forward, 5′-TGCAGTTTTGGTGACGACAG-3′, reverse 5′-GCATTGTACAGCCACTCTCG-3′), HAS3 (forward, 5′-GCTGGTGGGCATTATCAAGG-3′, reverse 5′-CCTAGAAGAACTGCCACCCA-3′), IL-6 (forward, 5′-CTGCAAGAGA CTTCCATCCAGTT-3′, reverse 5′-GAAGTAGGGAAGGCCGTGG-3′), IL-1β (forward, 5′-GCAACTGTTCCTGAACTCAACT-3′, reverse 5′-ATCTTTTGGGGTCCGTCAACT-3′), and GAPDH (forward, 5′-GAGGCCGGTGCTGAGTATGT-3′, reverse 5′-GGTGGCAGTGATGGCATGGA-3′).
Statistical analysis
Statistical analysis was performed using GraphPad Prism 6 (GraphPad Software, San Diego, CA) software. Results are expressed as mean ± SD. Data were tested for normal distribution. Two-way repeated measures analysis of variance was used when multiple time points were involved. Two-tailed Student's t test was used for comparison between the two groups. Pearson correlation test was used to find association between parameters. All analyses were considered statistically significant at p < 0.05.
Results
Lymphedema signs appear at day 4 after surgery
To evaluate HA and LTB4 as predictor biomarkers for lymphedema, we performed tail ablation of lymphatic vessel. Mice were divided in two groups. One group (Sham) involved tail skin incision only, whereas the second group (Lymphedema) included lymphatic ablation surgery. Before and after surgery, serum was collected as described in Figure 1A, and lymphatic architecture was evaluated by immunofluorescence analysis. Our results showed that lymphatic ablation surgery leads to progressive tail swelling, which is not observed in the Sham group (Fig. 1B). Lymphedema development had begun to be evident at day 4, giving us the first 2 days postsurgery as a window to evaluate our biomarker candidates for lymphedema. When we analyzed lymphatic architecture, the destruction of dermal lymphatic vessels was observed at day 1 postsurgery in the Lymphedema group (Fig. 2A). As previously described, we observed increased lymphangiogenesis as early as 2 days after surgery in the lymphedematous tail and remains higher until the end of the experiment (Fig. 2A, B). 25 These results showed that tail surgery efficiently affects lymphatic architecture, promoting tail swelling starting at day 4 after treatment.
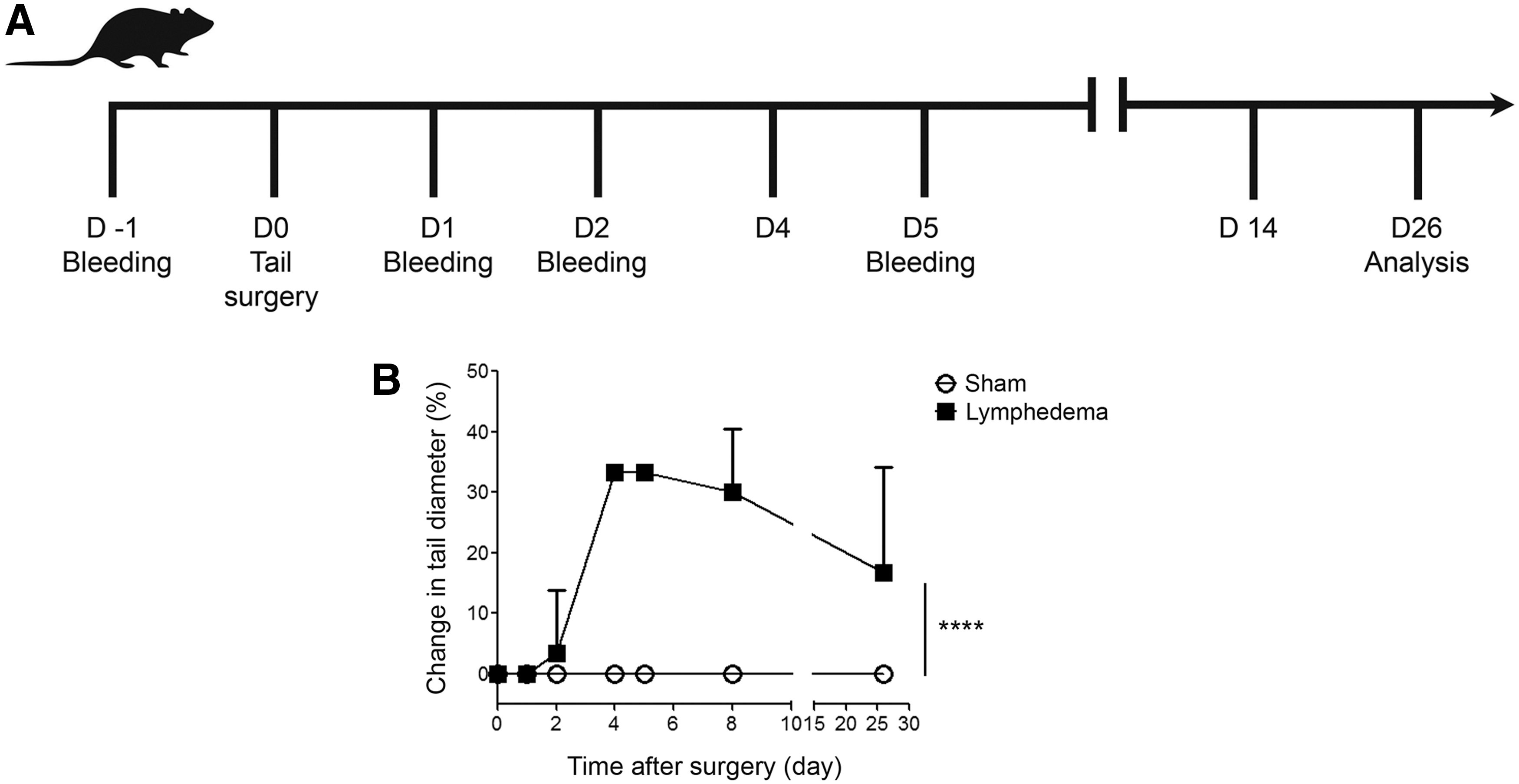
Tail lymphatic ablation leads to swelling starting at day 4 postsurgery.
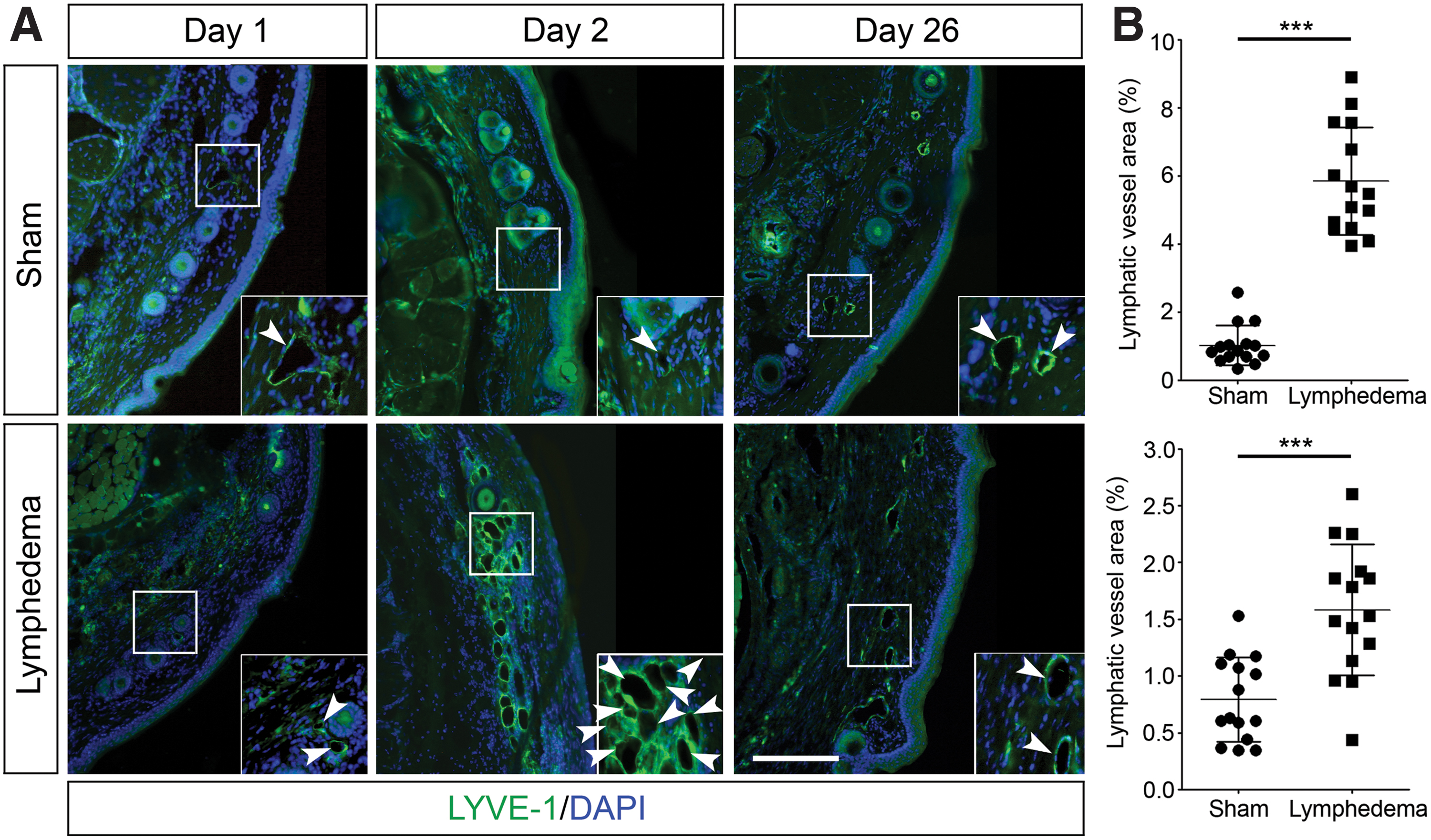
Efficient lymphatic vessel ablation is followed by rapid lymphangiogenesis.
Slight increase of HA levels at early days postsurgery
We next evaluated the serum levels of HA during the development and progression of lymphedema, focusing on early days to determine its predictor capability. Our results showed that HA levels were similar in both groups before the surgical procedure and remain similar in both groups at day 1 after lymphedema induction (Fig. 3A, B). Interestingly, at day 2 we observed a trend in increase of HA levels in the Lymphedema group compared to the Sham group without reaching significant differences (p = 0.07, Fig. 3C). Once the swelling is obvious at day 5 in the Lymphedema group and the tail diameter is at the maximum, this trend is lost (Fig. 3D). These results suggest that serum HA by itself is not a good biomarker capable of predicting acquired lymphedema development.
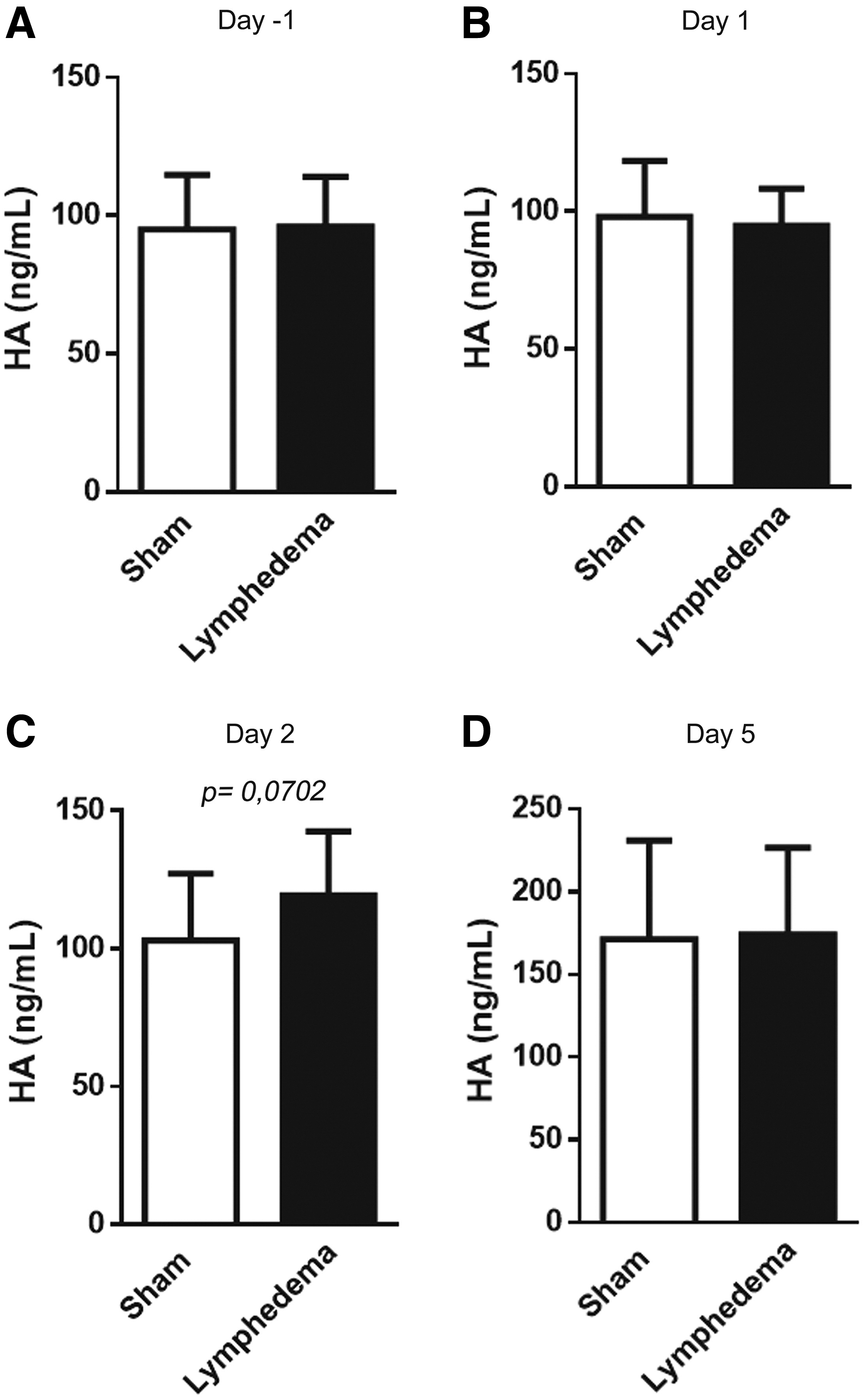
HA serum levels at early days postsurgery. HA levels were measured before surgery
LTB4 levels are significatively reduced at early days before the development of lymphedema signs
We next evaluated the serum levels of LTB4 at early days postsurgery. We observed a significative reduction of serum LTB4 in the Lymphedema group as early as 1 day postsurgery (p = 0.046, Fig. 4B). This difference begins to be less evident at day 2 (Fig. 4C) and is lost at day 5 postsurgery (Fig. 4D). These results suggest that serum levels of LTB4 can be a good biomarker candidate to predict the development of acquired lymphedema.

Reduced levels of LTB4 at day 1 postsurgery. LTB4 levels were measured before surgery
Increased hyaluronan synthases and reduced leukotriene A4 hydrolase in the lymphedema tissue
Next, we evaluated mRNA levels of several HA and LTB4 biosynthetic enzymes in the lymphedema tissue at early days postsurgery. Three hyaluronan synthases have been described so far in mammals, HAS1, HAS2, and HAS3. 26 While we were unable to detect HAS1 in the lymph edematous tail, we observed increased HAS2 and HAS3 mRNA levels at days 2 and 5 postsurgery (Fig. 5A, B), suggesting that HA levels are also increased in the lymphedema tissue at early time points. Regarding LTB4 synthesis, two key proteins involved in its biosynthesis, Arachidonate 5-lipoxygenase (5-LO), which catabolizes the oxygenation of arachidonic acid, and leukotriene A4 hydrolase (LTA4H), which converts Leukotriene A4 into LTB4, were evaluated in the lymphedema tissue. Although no significant differences were observed in the levels of 5-LO postsurgery (Fig. 5C), we found reduced LTA4H mRNA levels at days 1 and 2 postsurgery (Fig. 5D), suggesting a reduction of LTB4 levels in the lymphedema tissue at early days postsurgery.
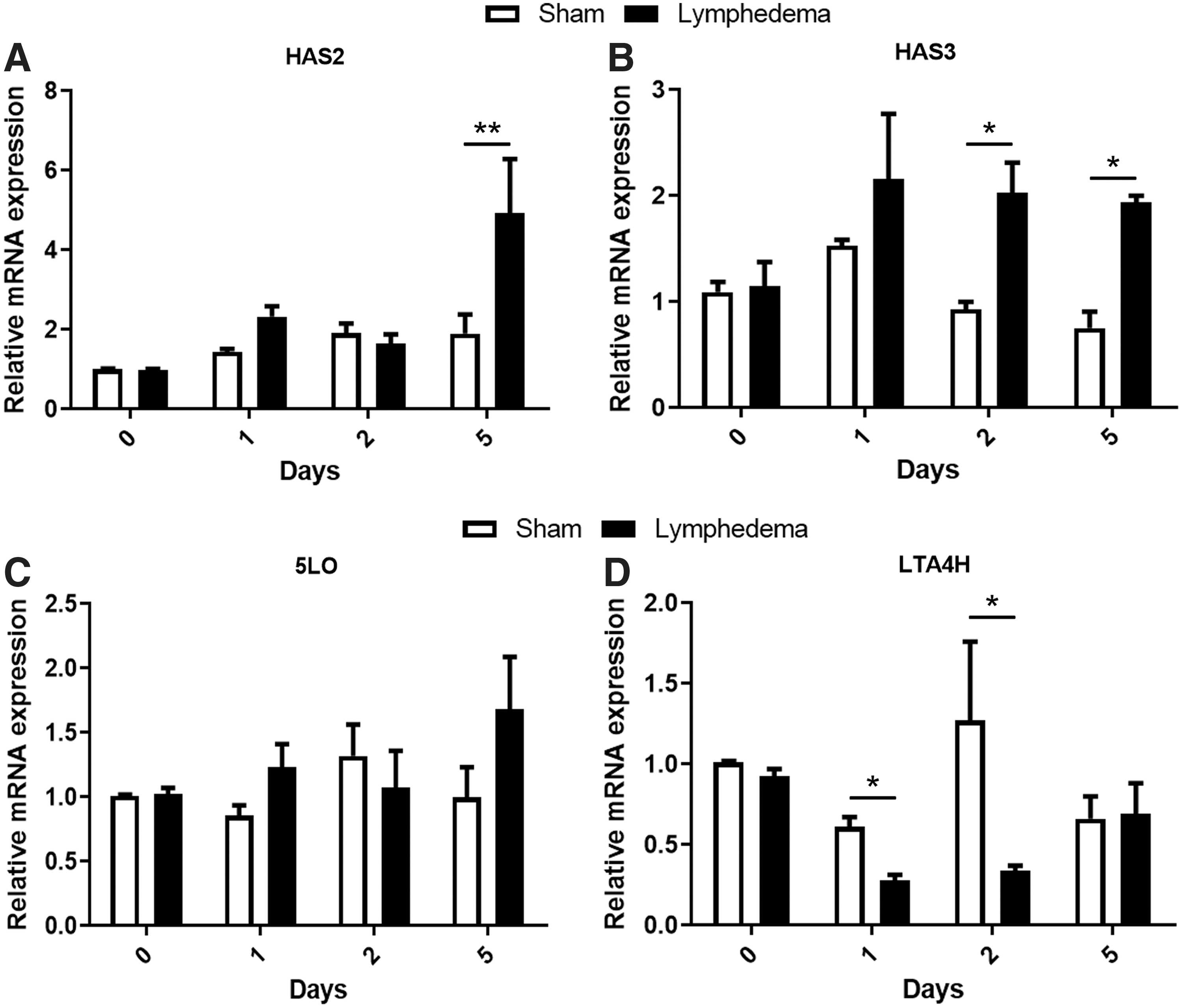
Altered mRNA levels of HA and LTB4 biosynthetic enzymes in the lymphedema tissue at early days postsurgery. mRNA levels of HAS2
Increased local and systemic inflammation at early days postsurgery
Because lymphedema development involves an aberrant immune response, we decided to evaluate local and systemic inflammation at early days postsurgery, by analyzing inflammatory cytokines IL-6 and IL-1β levels in the serum and in the lymphedematous tissue, and also evaluating macrophage infiltration into the damaged tissue, to correlate inflammation with changes in HA and LTB4 levels. Although we were unable to detect IL-1β in serum from Sham or Lymphedema treated mice (data not shown), we observed dramatic increase of IL-6 in the serum of the Lymphedema group at days 1 and 2 postsurgery (Fig. 6A). At a local level, we observed increase of both IL-6 and IL-1β mRNA levels in the lymphedematous tissue as early as 1-day postsurgery, followed by a gradual reduction at late time points (Fig. 6B). We also analyzed local macrophage infiltration into the lymphedematous tissue by analyzing F4/80 positive cells by immunofluorescence. Our results showed rapid macrophage infiltration throughout the dermis and close to the lymphatic vessels at day 1 postsurgery (not shown), reaching a peak at day 2 postsurgery (Fig. 6C). All these results showed increased local and systemic inflammation at early days postsurgery and suggest that changes in HA or LTB4 levels in the serum or in the lymphedematous tissue could contribute to this increased immune response.
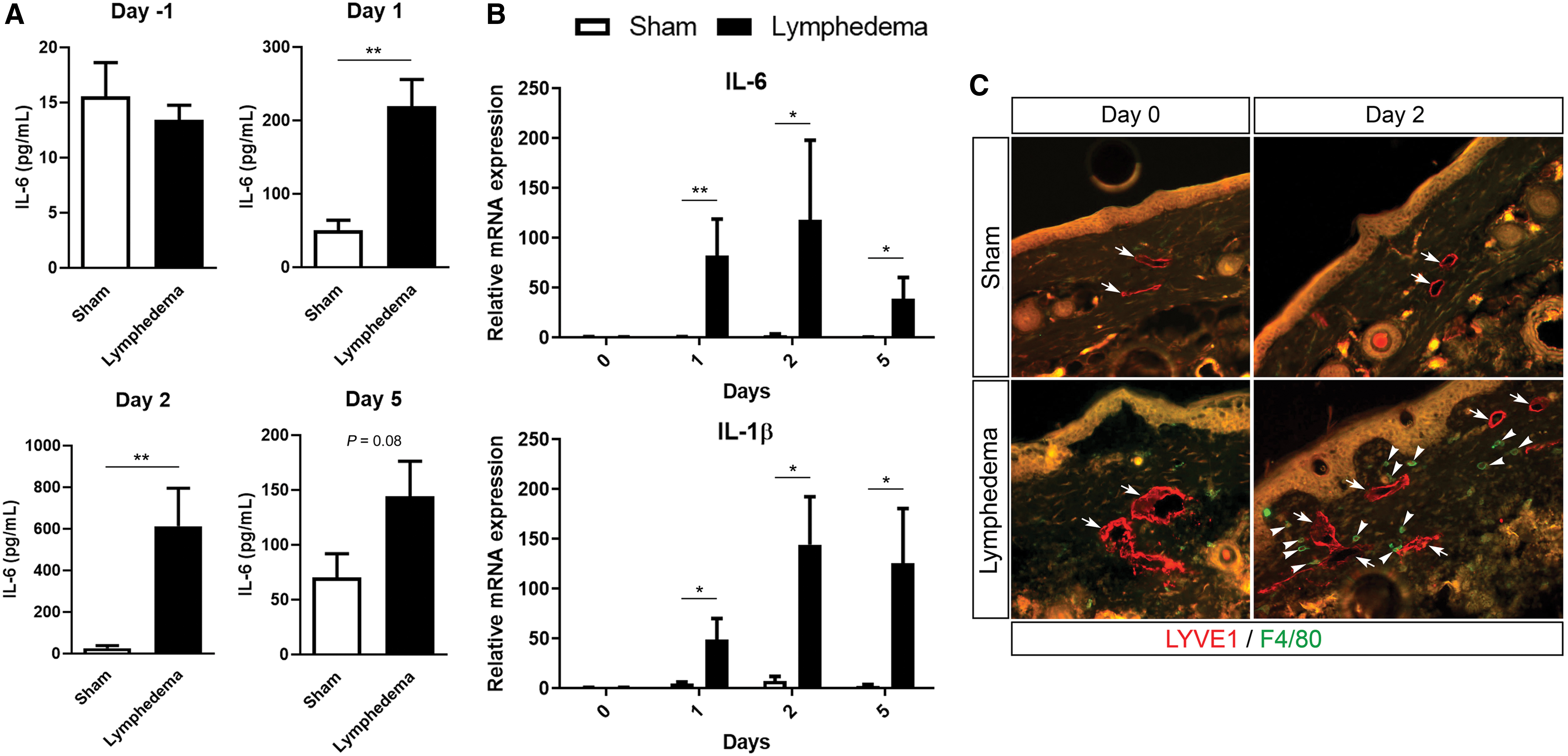
Augmented local and systemic inflammation at early days postsurgery.
Ratio LTB4/HA as biomarker to predict the development of acquired lymphedema
Because our results showed a trend of increase of serum HA levels and a significative reduction of serum LTB4 at early days in the Lymphedema group compared to the Sham group, we decided to evaluate the ratio LTB4/HA as a predictor of the development of acquired lymphedema. Our results showed a reduction of the ratio LTB4/HA in the Lymphedema group at day 1 postsurgery (Fig. 7B), reaching the strongest significance at day 2 postsurgery (p = 0.033, Fig. 7C). This difference is lost at day 5 postsurgery, concomitant with the appearance of swelling in the Lymphedema group (Fig. 7D). LTB4/HA ratio remains similar between both groups at late time points (not shown). These results suggest that serum ratio of LTB4/HA is the strongest predictor of acquired lymphedema development in mice.
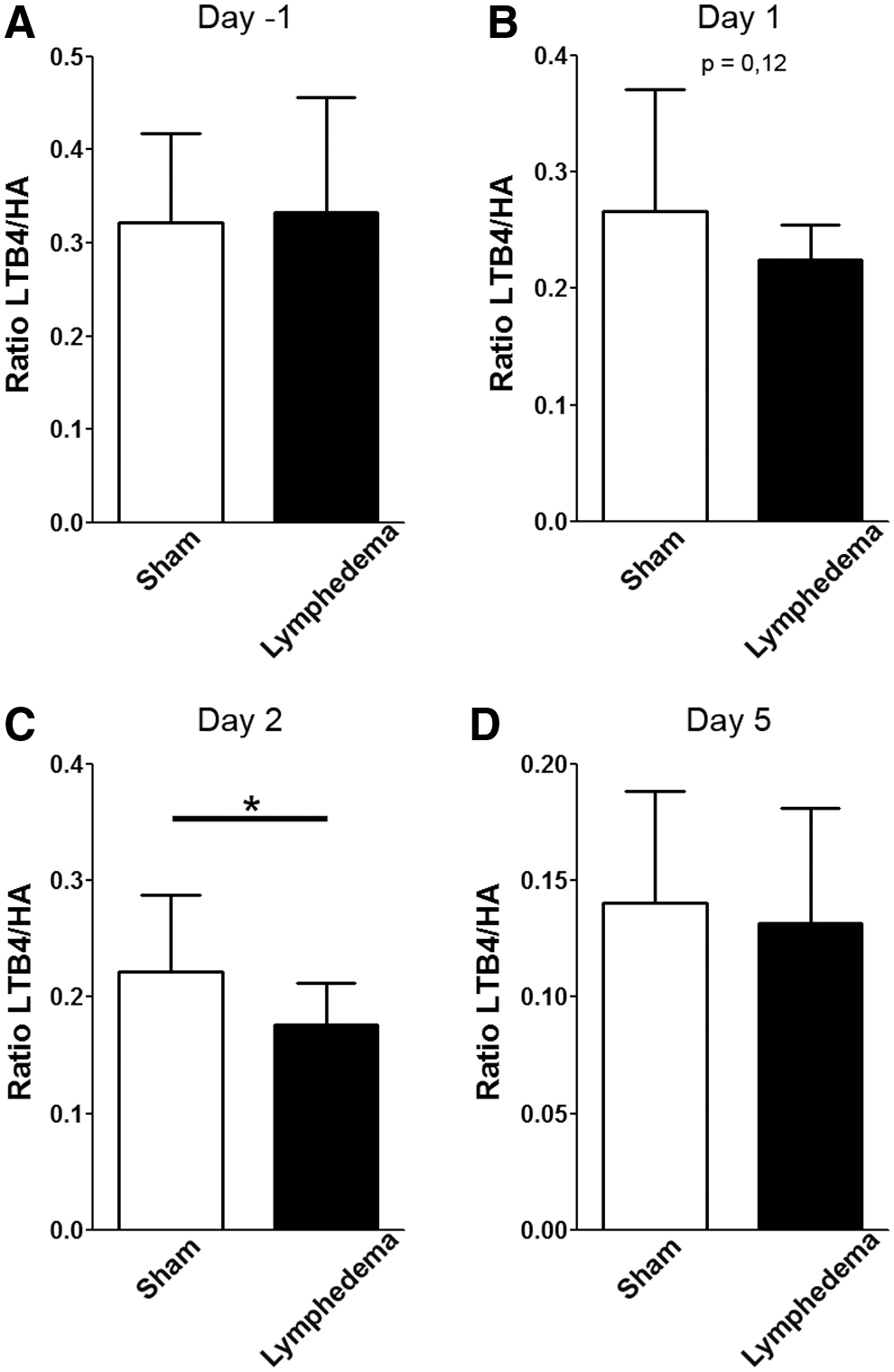
LTB4/HA ratio is a good biomarker to predict the development of acquired lymphedema. LTB4/HA ratio was calculated before surgery
Inverse association between LTB4/HA versus acquired lymphedema severity
Since the ratio LTB4/HA can predict the development of acquired lymphedema, we next evaluated if there is any correlation between LTB4/HA and lymphedema severity. Therefore, we calculated the ratio of LTB4/HA during the progression of lymphedema as the number of days that take lymphedema to resolve/day that clinical signs appear. Our results showed an inverse correlation; a reduction in the LTB4/HA ratio correlates with a greater severity of acquired lymphedema in our mouse model of tail lymphedema (Fig. 8). This result suggests that LTB4/HA ratio is not only able to predict the development of acquired lymphedema but also can give us information about how it will be the severity of lymphedema, with potential in clinical diagnostics.

Association between LTB4/HA ratio and lymphedema severity. A significant negative correlation between LTB4/HA ratio and lymphedema severity (Pearson correlation r: −0.5771) was observed. p < 0.01.
Conclusion
HA and LTB4 molecules have been previously associated with the development of acquired lymphedema.14,15,19 In this study, we provided evidence that the ratio LTB4/HA can be used as serum biomarker to predict the development of acquired lymphedema. We found a trend of increase of serum HA together with a significative reduction of LTB4 serum levels at early days before any clinical manifestation of acquired lymphedema. Interestingly, LTB4/HA ratio was not only the strongest predictor of the development of acquired lymphedema but also was able to predict lymphedema severity, suggesting that the ratio LTB4/HA can work as a reliable biomarker to predict acquired lymphedema development in our mouse model of tail lymphedema, with clear future potential in clinical diagnostics.
Secondary lymphedema, triggered by an acquired damage to the lymphatic vasculature, remains a growing health problem, and great efforts have been focused on preventing or diminishing the risk of developing secondary lymphedema, especially in cancer-related lymphedema.27,28 Despite the importance of finding new biomarkers capable of predicting lymphedema development, biomarker development for lymphedema detection is still a novel research area. 29 A very recent study has shown an association of pro-inflammatory cytokines and matrix metalloproteinases with the risk and course of lymphedema and fibrosis in patients with head and neck cancer. 30 Although the work did not focus on the early stages of lymphedema development, this study showed that pro-inflammatory cytokines contribute to the development of secondary lymphedema, highlighting the importance of immune cell response in the development of this condition. 30 Interestingly, in our study, we have identified the ratio LTB4/HA as a good biomarker to predict lymphedema development. In line with the previous study, both molecules can regulate immune responses. HA can interact through both Toll-like receptor (TLR) 4 and TLR2, as well as CD44, receptors that are expressed by several immune cells such as macrophages, dendritic cells, and T cells, to stimulate inflammatory genes in inflammatory cells.31,32 Specifically, HA can play different roles depending on its molecular weight. 33 Thus, higher molecular weight HA fragments, found under homeostatic conditions, have been shown to be anti-inflammatory, but lower molecular weight HA fragments that occur during many pathological conditions can stimulate the expression of pro-inflammatory cytokines, triggering inflammation.33,34 It is important to point that the Hyaluronan Quantikine ELISA Kit from R&D used in this study is unable to detect the very low molecular weight HA fragments in the serum, 35 which we can predict are the most abundant in the inflammatory environment triggered by the tail surgery, so we can speculate that using a different enzyme-linked immunosorbent assay (ELISA) kit that detects lower molecular weight HA fragments, the trend of increase of HA in the Lymphedema group will be more significative. Moreover, what is the role of the different molecular weight HA fragments in lymphedema development and how HA fragments modulate immune response during acquired lymphedema remain to be evaluated.
In contrast, LTB4 has been implicated in immune cell trafficking, natural killer and B cell activation, and promotion of pro-inflammatory cytokine production. 36 LTB4 is mainly produced by activated leukocytes, specially neutrophils, playing an important role in the fight against infections.37,38 Neutrophils, the most abundant type of white blood cells, are the first immune cells recruited to sites of bacterial infection or wounds. 39 Neutrophil infiltration is also important during the development of acquired lymphedema. 40 Interestingly, increased levels of LTB4 are found in the lymphedematous tissue at early days postsurgery, which could be explained, in part, by the extensive neutrophil infiltration in this model.19,40 Thus, we can speculate that the reduced levels of serum LTB4 at early days postsurgery found in our study could be, in part, explained by the rapid neutrophil infiltration into the lymphedematous tissue. More studies are needed to specifically evaluate the source and function of LTB4 over immune cell response during acquired lymphedema.
Alterations in HA and LTB4 levels have been observed in different preclinical and clinical studies. For example, increased serum HA serum levels have been reported in bronchoalveolar lavage fluid of persistent asthmatic patients, correlating this increase with disease severity.41,42 Similarly, elevated serum HA has been observed in rheumatoid arthritis, hand osteoarthritis, and chronic obstructive pulmonary patients, correlating serum HA levels with disease activity.43–45 Regarding LTB4, although it has been mainly considered as a pro-inflammatory lipid, early evidence has shown reduced LTB4 release by neutrophils in atopic dermatitis patients. 46 More recently, LTB4 has been shown to repress IL-1β release by macrophages in vitro and in vivo.47,48 These results were further supported by a study showing increased IL-1β production by Alox5−/− that lacks LTB4, as well as other leukotrienes. 49 This anti-inflammatory property of LTB4 seems to be, in part, mediated by its interaction with the anti-inflammatory nuclear transcription factor peroxisome proliferator-activated receptor-α. 49 All these evidences showed that altered HA and LTB4 serum levels can be observed in different clinical conditions and suggest that these molecules could work as predictive biomarkers of disease development.
Some limitations of our work should be considered. First, the tail model of acquired lymphedema likely does not exactly replicate human pathology. Second, the LTB4/HA reduction occurs in a precise moment and is not maintained during the entire phase before lymphedema development. However, we consider that this study provides enough evidence to explore the potential use of HA and LTB4 serum levels as biomarkers in human clinical studies.
In summary, our observations indicate that serum ratio of LTB4/HA can work as a novel biomarker to predict the development and the severity of acquired lymphedema. Because of the importance of these molecules in modulating immune responses, our results highlight the role of inflammatory responses in the development of lymphedema. The use of HA and LTB4 as biomarkers could facilitate the identification of patients with high risk to develop lymphedema. Further clinical studies are needed to validate these biomarkers as predictors of acquired lymphedema in patients.
Footnotes
Acknowledgments
The authors thank their funding sources that made it possible to support their research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the following grants: Proyecto Genera-Autónoma No. UA 17-04 and FONDECYT de inicio No. 11160592, CONICYT (N.E.) and Proyecto Redes Internacionales (REDI170651) (A.A.H.).