
Abstract
Background:
Lipedema and Dercum's disease (DD) are incompletely characterized adipose tissue diseases, and objective measures of disease profiles are needed to aid in differential diagnosis. We hypothesized that fluid properties, quantified as tissue water bioimpedance in the upper and lower extremities, differ regionally between these conditions.
Methods and Results:
Women (cumulative n = 156) with lipedema (n = 110), DD (n = 25), or without an adipose disease matched for age and body mass index to early stage lipedema patients (i.e., controls n = 21) were enrolled. Bioimpedance spectroscopy (BIS) was applied to measure impedance values in the arms and legs, indicative of extracellular water levels. Impedance values were recorded for each limb, as well as the leg-to-arm impedance ratio. Regression models were applied to evaluate hypothesized relationships between impedance and clinical indicators of disease (significance criteria: two-sided p < 0.05). Higher extracellular water was indicated (i) in the legs of patients with higher compared with lower stages of lipedema (p = 0.03), (ii) in the leg-to-arm impedance ratio in patients with lipedema compared with patients with DD (p ≤ 0.001), and (iii) in the leg-to-arm impedance ratio in patients with stage 1 lipedema compared with controls (p ≤ 0.01).
Conclusion:
BIS is a noninvasive portable modality to assess tissue water, and this device is available in both specialized and nonspecialized centers. These findings support that regional bioimpedance measures may help to distinguish lipedema from DD, as well as to identify early stages of lipedema.
Introduction
Adipose tissue diseases are often resistant to commonly-prescribed diet and exercise, and the etiology of these diseases is not well understood.1,2 Lymphatic dysfunction has been proposed as a component of the pathophysiology of adipose tissue diseases, namely lipedema and Dercum's disease (DD), based on symptoms of lower extremity edema.2,3 A clear understanding of the topography of edema has not been reported in these populations; however, understanding the spatial distribution of fluid and adipose distribution, and associated tissue water generally, could impact our understanding of disease etiology and assist with differential diagnosis and evaluating treatment outcomes.
More specifically, lipedema is a chronic condition involving excessive and disproportionate adipose tissue deposition in the lower extremities of females. 2 Clinically, external features of lipedema are described in three stages of severity. 4 The legs of patients with lipedema have normal appearing skin over a thick and nodular hypodermis (stage 1), dimpling of the skin and larger masses in the thick nodular adipose tissue (stage 2), and visible large lobules of skin and adipose tissue on the legs that may compromise joint integrity and impair mobility and balance (stage 3, Fig. 1). Symptoms of fatigue, diffuse aches or pain, easy bruising, and muscle weakness can coincide with any stage of lipedema. It remains unclear whether lipedema severity corresponds with changes in tissue composition, namely water retention, and the quantitative extent to which upper and lower extremities are involved. Characterizing these relationships is important for improving our understanding of disease origins, as well as differentiating lipedema from other conditions that share similar external phenotypes as lipedema (e.g., obesity), but have fundamentally discrepant physiological origins and corresponding management strategies.
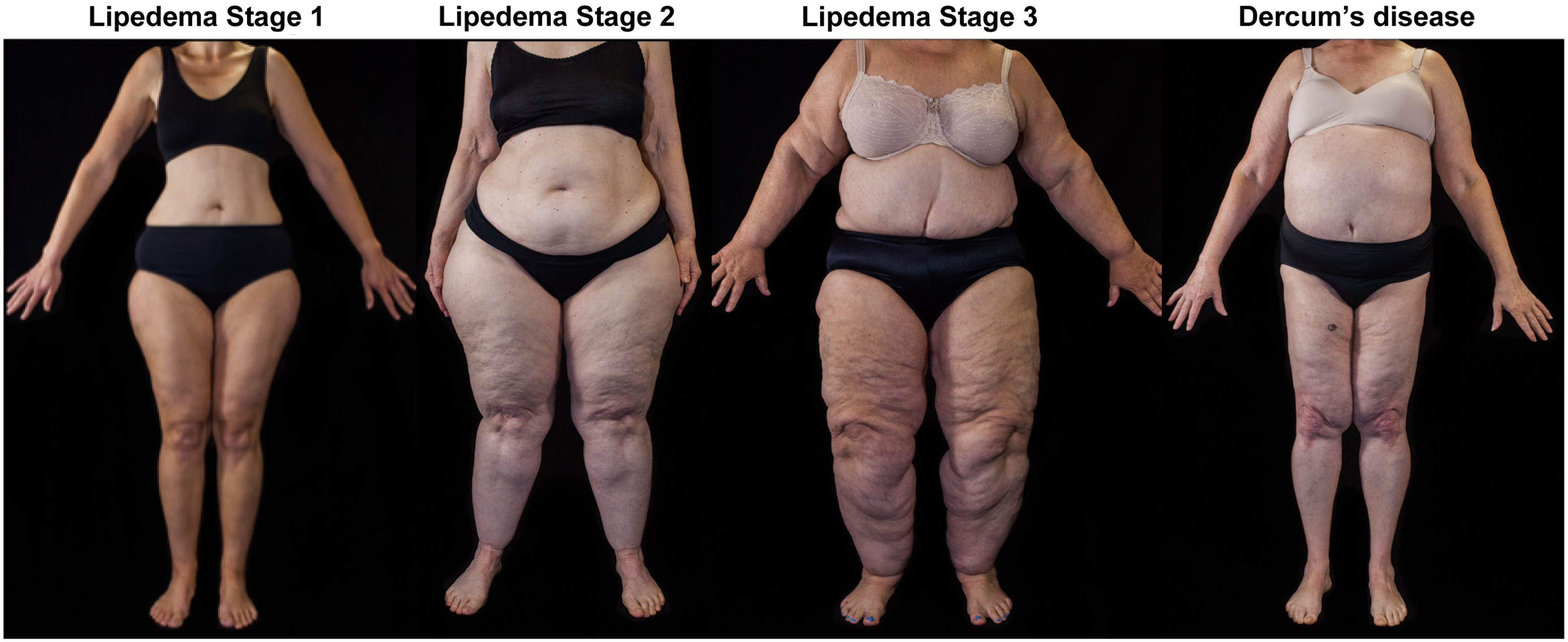
Example photos of patients with lipedema stages 1, 2, or 3 and a patient with DD reveal body shape characteristics of these adipose tissue diseases. Note the disproportionate size of the lower extremities in patients with lipedema, and the swollen appearance of the abdomen in DD. DD, Dercum's disease. Color images are available online.
DD is also an adipose tissue disease that can share many clinical features with lipedema. Subcutaneous adipose tissue has palpable pearl-sized nodules in patients with diffuse DD, similar to early stages of lipedema. 5 However, DD is distinguishable from lipedema based on the location of fat and nodules presenting on the torso in addition to the limbs (e.g., Fig. 1) early in the disease process for DD. In addition, there is generally a higher mean daily pain, prevalence of painful comorbid disorders such as fibromyalgia, and an increased occurrence of metabolic disease in patients with DD. 5 Differentiating these conditions generally requires specialized clinicians aware of these subtle differences, however, it may be difficult for the untrained clinician to identify. The differential diagnosis of lipedema versus DD can be additionally complicated by excess nonlipedema gynoid or android fat (obesity), masking the disproportionate body shape characteristic of lipedema. Understanding how tissue composition is altered in regions of the body affected by DD, and how this differs from patients with lipedema, may provide insight into the etiology and assist with differential diagnosis of adipose tissue diseases especially in nonspecialized centers.
The purpose of this study is to report objective measures of tissue water properties in women who met clinical criteria for lipedema or DD, and women without an adipose tissue disease. We utilized a bioimpedance spectroscopy (BIS) unit to measure tissue water in the upper and lower extremities. We hypothesized that BIS metrics in the legs are elevated in (i) patients with higher compared with lower stages of lipedema, (ii) patients with lipedema compared with DD, and (iii) patients with stage 1 lipedema compared with female controls matched for age and body mass index (BMI) and without an adipose tissue disease.
Materials and Methods
Volunteer recruitment
This study is part of a multicenter collaborative effort to provide objective phenotyping of patients with lipedema and DD. All research activities were approved by the institutional review boards of the University of Arizona and Vanderbilt University Medical Center (VUMC). To recruit an adequate number of patients with these relatively poorly recognized conditions, these devices were brought to the Fat Disorders Resource Society (FDRS) conference attended by patients, physicians, and researchers. The study was conducted off-site at the FDRS conferences in St. Louis, Missouri (2017) and Salt Lake City, Utah (2018), or on-site at VUMC (April 2016–April 2018).
Survey and physical examination
Volunteers were enrolled after providing informed written consent. All participants were evaluated by physical examination in a private area for objective clinical criteria of lipedema and DD. Participants were evaluated by a board-certified endocrinologist (K.L.H.) with >13 years of experience treating patients with lipedema and DD to determine the presence of disease; using identical criteria, subjects enrolled at VUMC were evaluated by a certified physical therapist (P.M.C.D.) with subspecialty certification and training by the Lymphedema Association of North America, and 12 years of experience treating patients with lymphedema and lipedema. Participants determined to have lipedema or DD were required to meet all primary criteria and at least two secondary disease criteria for each condition (Table 1). Disease criteria determined during physical examination included disparity between the abdomen and limbs noted as android or gynoid body habitus, confirmed by anthropometric measurements. Tissue on the arms, abdomen, flanks/hips, lower back, and legs was examined by palpation, and nodules the size of a pea and larger lipomas were noted as was stage of lipedema if appropriate. Fat deposits under the knee, on the medial knee, medial elbow, hips, wrist cuff, ankle cuff, medial and lateral malleoli, and adjacent to the Achilles tendon were noted and assessed for nodularity. Pitting and nonpitting edema was assessed on the lower legs by pressure using the fingers, and Stemmer's sign was used to assess edema of the hands and feet. 6 The presence of bruising, pain on palpation, spider veins, varicose veins, and corona phlebectatica was noted and recorded. Hypermobility of joints was assessed using the Beighton score. 7 Medical histories were reviewed for evidence of abnormal bruising, pain in the legs, family history of lipedema or DD, fatigue, and additional secondary criteria (Table 1).
Disease Criteria
Clinical criteria were adopted from Herbst et al. 2
Biophysical examination
A biophysical examination was performed (Fig. 2) that comprised height, weight, and BIS. Participants were required to lay supine for ∼10 minutes after which BIS (L-Dex U400; ImpediMed, Ltd., Pinkenba, Australia) was applied to measure impedance of each arm and leg. The L-Dex U400 requires placement of electrodes at standardized locations on the wrists and feet (Supplementary Methods), with attachment of lead wires as industry directed to obtain bioimpedance measurements in the four limbs.

Volunteers received a physical examination and bedside BIS measurement.
Data analyses
Height and weight were converted to metric units and BMI was calculated (kg/m2). BIS data were analyzed using manufacturer software following the Cole–Cole analysis. 8 For each limb, impedance values acquired with multiple transmit frequencies in the range of 5–1000 kHz were used to extrapolate impedance values at 0 kHz and at the limit of an infinite frequency (R0 and R∞ respectively, in units of Ω). 9 Higher levels of extracellular water are inversely correlated with R0 impedance, and higher levels of total limb water are inversely correlated with R∞ impedance.10,11 An additional BIS metric was computed as R0 or R∞ in the leg normalized by that in the arm (leg/arm impedance ratio) on the same side (right or left). This metric is similar to the affected/unaffected limb impedance ratio reported in patients with unilateral lymphedema, by which lower impedance ratios indicate greater tissue water content in the affected limb. 12 Therefore, the metrics that were recorded and preserved for hypothesis testing were BIS values: R0 in the legs, arms, and leg/arm ratio; R∞ in the legs, arms, and leg/arm ratio.
Statistical analyses and data reporting
Descriptive statistics, including means, standard deviations, and ranges of continuous parameters (e.g., age, BMI, and BIS metrics), were calculated. Frequencies were calculated for categorical variables (e.g., disease status of lipedema stage or lipedema, DD, or control). A Student's t-test was used to confirm that patients with stage 1 lipedema were matched to controls for age and BMI.
The statistical objectives were to evaluate whether BIS metrics differ with disease status for patients with (i) different stages of lipedema, (ii) lipedema compared with DD, and (iii) stage 1 lipedema compared with controls. To test the first group comparison between patients with different stages of lipedema, a multivariable linear regression model was applied using leg R0 as the dependent variable and age, BMI, side of measurement (left or right), and disease status (lipedema stages 1, 2, or 3) as independent variables. Separate models were evaluated with identical independent variables and alternative dependent variables: arm R0, leg/arm R0 ratio, leg R∞, arm R∞, and leg/arm R∞ ratio. To test the second group comparison between patients with lipedema and patients with DD, we used the same dependent variables as already outlined, and independent variables were age, BMI, side of measurement (left or right), and disease status (lipedema or DD). To test the third group comparison between patients with lipedema stage 1 and controls, we used the same dependent variables as already outlined, and independent variables were age, BMI, side of measurement (left or right), and disease status (lipedema or control).
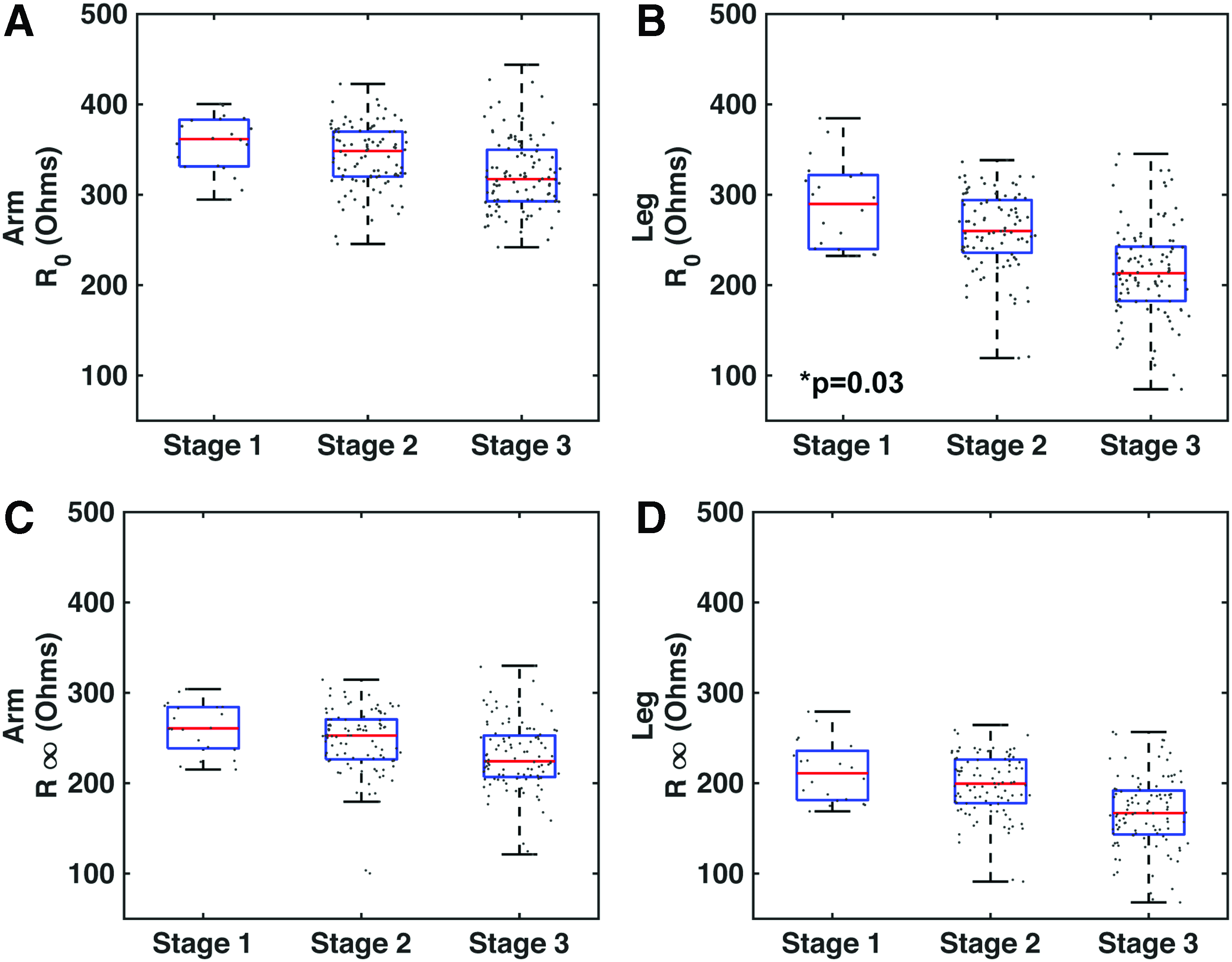
The number of observations, F-statistic, R-squared, and p-value for each model are reported along with coefficients and p-values for the independent variables. Boxplots depict the group median (red bar), upper and lower quartiles (upper and lower blue lines), and whiskers extend to twice the interquartile range. Individual data points are overlaid and randomly distributed on the horizontal axis for completeness and visualization purposes.
Results
Volunteer characteristics
All volunteers were female, consistent with lipedema affecting primarily females. Volunteers with lipedema (n = 110) were lipedema stage 1 (n = 10), stage 2 (n = 48), and stage 3 (n = 52), and had other characteristics: age = 51.3 ± 10.9 years; BMI = 37.5 ± 10.0 kg/m2; race = 95% white, 5% black. Characteristics of volunteers with DD (n = 25) were age = 56.9 ± 8.6 years; BMI = 37.6 ± 8.2 kg/m2; race = 92% white, and 4% American Indian or Alaskan Native, and 4% declined to comment. Characteristics for control volunteers without an adipose tissue disease (n = 21) were age = 45.7 ± 11.1 years; BMI = 28.4 ± 4.1 kg/m2; race = 100% white. Controls were of identical biological sex and not significantly different in terms of age (p = 0.10) and BMI (p = 0.06) to patients with stage 1 lipedema. Age and BMI were incorporated as covariates in regression models to account for any differences in distribution of these characteristics. A summary of the volunteer characteristics is provided in Table 2.
Characteristics of Study Cohorts and Bioimpedance Spectroscopy Measurements
Values represent mean ± standard deviation [minimum, maximum].
All lipedema indicates patients with stages 1, 2, and 3 lipedema.
BMI, body mass index; R0 and R∞ (Ώ), impedance values inversely related to extracellular and total tissue water volume, respectively.
Tissue water in patients with different stages of lipedema
BIS results are summarized in Table 2. Comparing BIS metrics in patients with different stages of lipedema, decreasing trends of R0 (i.e., increasing extracellular water) and R∞ (i.e., increasing total limb water) were observed in the arms and legs of patients with higher stages of lipedema (Fig. 3). Leg R0 has a significant relationship with lipedema stage (p = 0.03), accounting for significant covariates of age (p = 0.009) and BMI (p < 0.001; Supplementary Table S1).
Bioimpedance
Tissue water in patients with lipedema compared with patients with DD
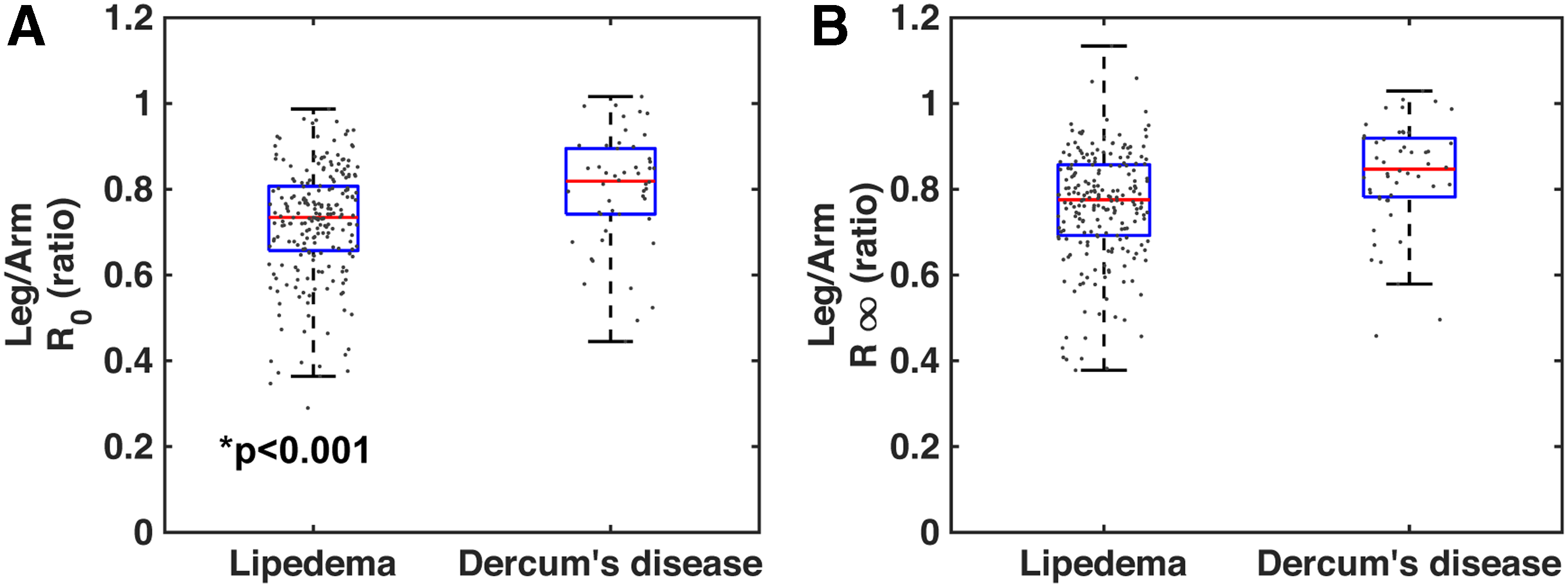
Comparing BIS metrics in patients with lipedema and patients with DD, reduced BIS values were observed in the legs of patients with lipedema (R0 = 241.7 ± 53.8 Ω, R∞ = 185.2 ± 40.2 Ω) compared with those in patients with DD (R0 = 263.0 ± 56.6 Ω, R∞ = 199.2 ± 45.1 Ω). Leg R0 has a significant relationship with disease status (lipedema vs. DD; p < 0.001), accounting for significant covariates of age (p = 0.009) and BMI (p < 0.001; Supplementary Table S2). Leg R∞ has a significant relationship with disease status (p = 0.003), accounting for covariates of age (p = 0.49) and BMI (p < 0.001). Leg/arm R0 has a significant relationship with disease status (p < 0.001), accounting for significant covariates of age (p = 0.003) and BMI (p < 0.001; Fig. 4).
Bioimpedance
Tissue water in patients with early stage lipedema compared with controls
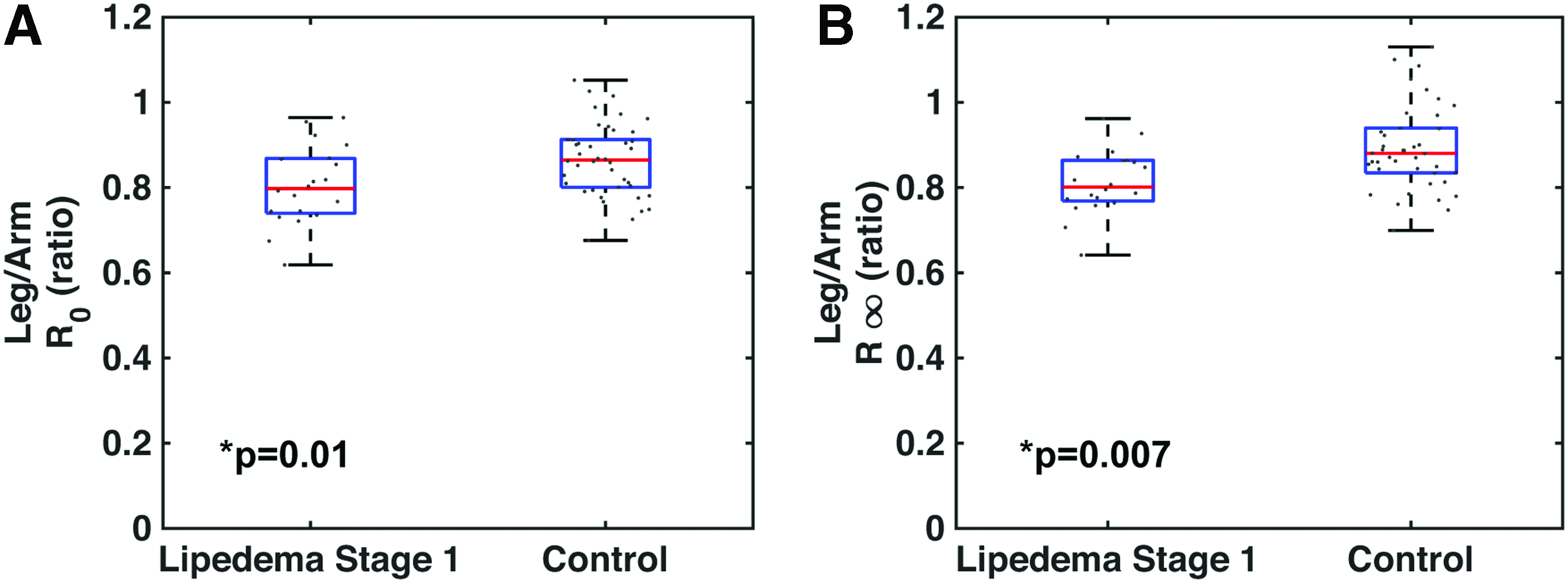
Comparing BIS metrics between patients with stage 1 lipedema and controls without an adipose tissue disease matched for age and BMI, reduced BIS values were observed in the legs of patients with stage 1 lipedema (R0 = 287.9 ± 48.3 Ω, R∞ = 212.6 ± 33.2 Ω) compared with those in controls (R0 = 294.8 ± 32.8 Ω, R∞ = 218.1 ± 25.4 Ω). BIS values in the arms were higher in patients with stage 1 lipedema (R0 = 357.0 ± 30.6 Ω, R∞ = 261.3 ± 27.7 Ω) than those in controls (R0 = 341.8 ± 32.6 Ω, R∞ = 244.0 ± 28.7 Ω). Thus, the combined trend leg/arm R0 has a significant relationship with disease status of stage 1 lipedema versus control (p = 0.01; Supplementary Table S3). Similarly, leg/arm R∞ has a significant relationship with disease status (p = 0.007; Fig. 5).
Bioimpedance
Discussion
Lipedema and DD remain incompletely characterized adipose tissue diseases where objective diagnostic criteria between the diseases would be clinically advantageous especially in the setting of lipedema with truncal obesity. We identified women who met clinical criteria for lipedema or DD, or who were without an adipose tissue disease, and objectively measured tissue composition utilizing a bedside bioimpedance device. BIS tools have been applied broadly to study fluid balance in conditions of kidney dysfunction, 13 weight loss, 14 dehydration, 15 inflammation, 16 antiviral treatment, 17 obesity,18,19 and most notably lymphedema.20–27 In this study, bioimpedance reveals increased extracellular water primarily in the legs of patients with lipedema, and affects the arms and legs differently in patients with lipedema compared with patients with DD, and early stage lipedema compared with females without an adipose tissue disease. Next, we interpret the indications of significant findings and discuss the clinical relevance of this study.
Extracellular water increases with stage of lipedema
Our findings of decreased impedance value R0 indicate higher extracellular water content in the legs of patients with more severe lipedema (higher stage). This is generally consistent with clinical findings of pitting and nonpitting lymphedema associated with lipedema, often termed lipolymphedema.2,28
One additional interpretation of lower BIS values may be that the extracellular fluid has decreased resistance, or is more conductive, and differentially affected by lipedema stage. The conductance of extracellular fluid is determined by the ion concentration (i.e., higher ion concentration reduces resistance), sodium being the most concentrated. 29 The presence of greater tissue sodium content in the legs of patients with lipedema was recently observed by noninvasive sodium magnetic resonance imaging. 30 This raises the possibility that higher tissue sodium content could drive lower impedance in legs affected by lipedema, and is a relevant component of tissue composition to study further in patients with lipedema.
DD affects upper and lower body tissue water
Patients with lipedema have lower impedance values in the legs than patients with DD, indicating higher extracellular and total tissue water volume in the legs of patients with lipedema. The leg/arm impedance ratios were closer to unity in DD and lower in lipedema, suggesting both upper and lower body water retention in DD. It is interesting to note that painful subcutaneous lipomas (defined as >1 cm diameter) are often found in the abdomen, back, and extremities of patients with DD. 5 Enlarged lymphatic vessels of the legs and extraneous lymphoid tissue are reported in a case study of a patient with DD, 31 which may affect water retention, although the etiology of altered tissue composition associated with lipedema and DD remains an active area of investigation.
Tissue water distribution in patients with early stage lipedema
It is estimated that 80% of lipedema patients experience arm involvement. 32 In our cohort, arm impedance is greater in stage 1 lipedema than that in controls. This trend likely indicates higher fat content in the arms, whereas in the legs, impedance is lower indicating higher water content. Together, the leg/arm impedance ratio is significantly lower in patients with stage 1 lipedema than that in controls. Further characterizing how lipedema effects the body systemically, especially early in disease onset, is merited. Precise measurements through imaging, tissue biopsy, and blood biomarkers may be appropriate to acquire in the upper and lower extremities of patients with early stage lipedema to improve our understanding of the etiology and topography of disease.
Areas of potential clinical impact
This study addresses two potential clinical unmet needs for patients with adipose tissue diseases. First, early diagnosis of lipedema at or around stage 1 is particularly difficult due to lack of awareness of lipedema as a medical condition, and the subtle changes in external appearance of legs affected by early lipedema. Consequently, lipedema diagnosis is frequently delayed or overlooked unless lipedema stages 2 or 3 develop. 33 Lipedema patients report a mean age at diagnosis of 44 years, 34 although symptoms typically onset 20 years earlier after menarche or pregnancy. 32 This cross-sectional study of patients with lipedema is a step toward providing objective criteria of disease stage and differential diagnosis. BIS metrics in lipedema compared with those in controls show regional differences in tissue composition in the arms and legs that may inform ways to achieve early diagnosis. Determining the sensitivity and specificity of BIS for early stage lipedema will likely require more subjects and is an ongoing area of investigation.
Second, misdiagnosis of adipose tissue diseases is a fundamental issue, as patients are receiving treatments that are not optimized to reduce resistant adipose deposition and associated water retention. Common treatments for obesity such as exercise and restricted caloric intake, 1 and gastric bypass surgery,35,36 are effective for the obese tissue but less effective for adipose tissue deposition due to lipedema or DD. Evidence of elevated tissue water in both diseases, but in specific areas, suggests that alternative treatment options should be investigated. For instance, conservative treatment through the application of complete decongestive therapy (utilizing compression, manual lymphatic drainage therapy, and targeted exercise) may be effective in management of edema, joint instability and pain or aches in the limbs; whereas deeper massage techniques37–39 are being investigated for their effect on reducing adipose tissue volume and fibrosis. Surgical removal by liposuction will likely play a role in treatment of lipedema 40 until its etiology is identified and targeted. Pharmaceutical treatments may also be effective in reducing persistent fat 41 or adipose deposition due to lymphatic impairment. 42 The successful implementation of treatments for lipedema and DD will require adequate tools to identify potential patient candidates and measure the tissue's response to therapy. BIS devices have potential to objectively track changes in tissue composition in response to these emerging therapies for patients with adipose tissue diseases.
Limitations
Volunteers represent those who have the resources to travel and take leave from work, and this study was not able to control for socioeconomic status or employment status. We were not able to control for treatment status, including liposuction that may alter intra- and extracellular water relationships. 43 Although BIS measurements may aid in objective evaluation of adipose tissue diseases, measurement ranges overlap between study cohorts. Therefore, clinical criteria used in this study must also be met to determine an individual's differential diagnosis in the clinic. Longitudinal monitoring would be necessary to determine an individual's progression of lower extremity water levels and lipedema stage, which deserves further investigation.
Conclusion
Patients with adipose tissue diseases of lipedema and DD suffer from insufficient medical attention due to lack of awareness and diagnostic tools for aiding clinical decision making. We report objective values of tissue water bioimpedance in the upper and lower extremities of 156 women who met clinical criteria for lipedema or DD or who were without an adipose tissue disease. BIS findings indicate higher tissue water levels (i) in the legs of patients with higher compared with lower stages of lipedema, (ii) in lipedema than in DD patients, and (iii) in stage 1 lipedema patients than in matched control participants. This relatively inexpensive and portable device can be applied in both specialized and nonspecialized centers to potentially assist with differential diagnosis for these conditions. Bioimpedance may have relevance for further understanding the etiology of adipose tissue diseases and quickly evaluating the impact of emerging therapies on tissue composition.