
Abstract
Background:
It is not always possible to detect nonpalpable small lymph nodes (LNs) surrounded by adipose tissue under the wavelength of visible light. A newly developed near-infrared camera with InGaAs element was able to capture photographs using light at >1000-nm wavelength, at which the difference in absorbance between water and lipids is large. This study investigated the ability to detect nonvisible small LNs using light at 1300-nm wavelength.
Methods and Results:
Following retrieval of LNs through axillary LN dissection from 20 patients with breast cancer, residual specimens were simultaneously photographed using light at 970-, 1070-, 1200-, 1300-, 1450-, and 1600-nm wavelengths. A total of 45 specimens were observed pathologically at the selected portions in which the 1300-nm light was absorbed (high absorbance group [HA group], n = 25) and those in which the 970-nm light was absorbed instead (low absorbance group [LA group], n = 20). All specimens categorized in the HA group detected the LNs, whereas none of those categorized in the LA group detected an LN. The sensitivity and specificity in the identification of an LN were 1.0. The LNs detected using this camera were significantly smaller than those detected by surgeons (3.00 ± 2.93 mm vs. 5.90 ± 3.91 mm, p < 0.01).
Discussion:
The light at 1300-nm wavelength was absorbed by axillary LNs. This camera detected LNs that were undetectable by surgeons. This novel technology may be applied to lymphatic microsurgery and contribute to the development of a minimally invasive LN dissection method.
Introduction
Lymph nodes (LNs) are small organs, playing important roles in maintaining homeostasis in humans and progression of cancer. 1 In the surgical treatment of certain types of cancer, LNs are resected and dissected to assess the stage of disease and determine the most appropriate adjuvant therapy.2–5 A sufficient number of LNs is required to provide an accurate pathological staging.6–9 In current surgical practice, LN sampling entails the resection of the adipose tissue, which surrounds the LNs, the lymphatic vessels connected to them, and the surrounding blood vessels. However, this approach causes obstruction of the blood flow and lymphatic flow.
In the previous decade, obstruction of the lymphatic flow after LN dissection was recognized as a therapeutic target for microsurgical reconstruction. Following the development of extremity lymphedema after LN dissection in patients with cancers (e.g., breast or gynecological cancers), autologous LNs were transferred from a healthy portion of the body to the affected limb. This approach aims to reconstruct the function of the lymph fluid transportation.10–15
However, it is not always possible to detect small LNs surrounded by adipose tissue using visible light. To detect sentinel LN or to transfer LN, an enhanced near-infrared camera, colored dye, or radio isotope were used.16–27 However, LNs that are not on the way of enhanced lymphatic route cannot be detected with those methods. Even on the way of enhanced route, nonpalpable small LNs may be ignored.
Recently, a novel near-infrared camera with indium gallium arsenide (InGaAs) element was developed. 28 This device is characterized by high sensitivity in the near-infrared region at >1000-nm wavelength. One of the unique characteristics of light in wavelengths ranging from 1300 to 1600 nm is the difference in absorbance between water and lipids. 28 However, the appearance of each structural component within human soft tissue under these wavelengths is currently undetermined.
We hypothesized that it may be possible to detect nonpalpable small LNs surrounded by adipose tissue using this novel near-infrared camera, without the requirement for contrast medium or damage to the surrounding tissue. The purpose of this study was to investigate the ability of this camera to detect LNs from surrounding adipose tissue using resected specimens. The future perspective of this study was to develop a device for intraoperative assessment to distinguish organs in the adipose tissue.
Patients and Methods
This study was conducted at the Chiba University Hospital (Chiba, Japan). The study protocol was approved by the Institutional Review Board and Ethics Committee (no. 2553). Patients with breast cancer who underwent axillary LN dissection from July 2017 to October 2018 at our institution were included in this study. In addition to patients in whom metastasis of axillary LN was already diagnosed through preoperative needle biopsy, those in whom LN dissection was indicated in response to positive sentinel lymph node biopsy (SLNB) were also included. Patients were included regardless of the use of neoadjuvant chemotherapy.
All patients underwent standard treatments for breast cancer based on the findings of their preoperative examinations.29–31 After LN dissection, LN retrieval from the resected axillary specimen was performed as usually performed in our institution. In brief, LNs were examined immediately by surgeons after surgery before fixation with formaldehyde, using blunt manual dissection, inspection, and palpation techniques. Chemical dissolution of fatty tissue was not used in our institution. After careful gross dissection of the specimen, all detected LNs were fixed in 10% formaldehyde and sent to the clinical pathologist (first examination). The clinical diagnosis was based on the first examination.
The near-infrared camera with an InGaAs element
The remnant specimen after the first examination was examined using a near-infrared camera with an InGaAs element (NIR-P01S; Nikon Corporation, Tokyo, Japan; Fig. 1). A unique characteristic of near-infrared cameras with an InGaAs element is the ability to show long-wavelength light >1000 nm, which cannot be visualized by existing near-infrared cameras. In the region exceeding 1000 nm, the absorbances of water and oil were significantly different. 28 NIR-P01S, the camera used in this study, can capture moving images at 970-, 1070-, 1200-, 1300-, 1450-, and 1600-nm wavelengths. In addition, still images of each wavelength and visible light could be obtained simultaneously (Figs. 2 and 3).*

Appearance of the newly developed InGaAs camera and the design of the camera section.

A resected specimen of axillary LN dissection after LN retrieval in the first examination.
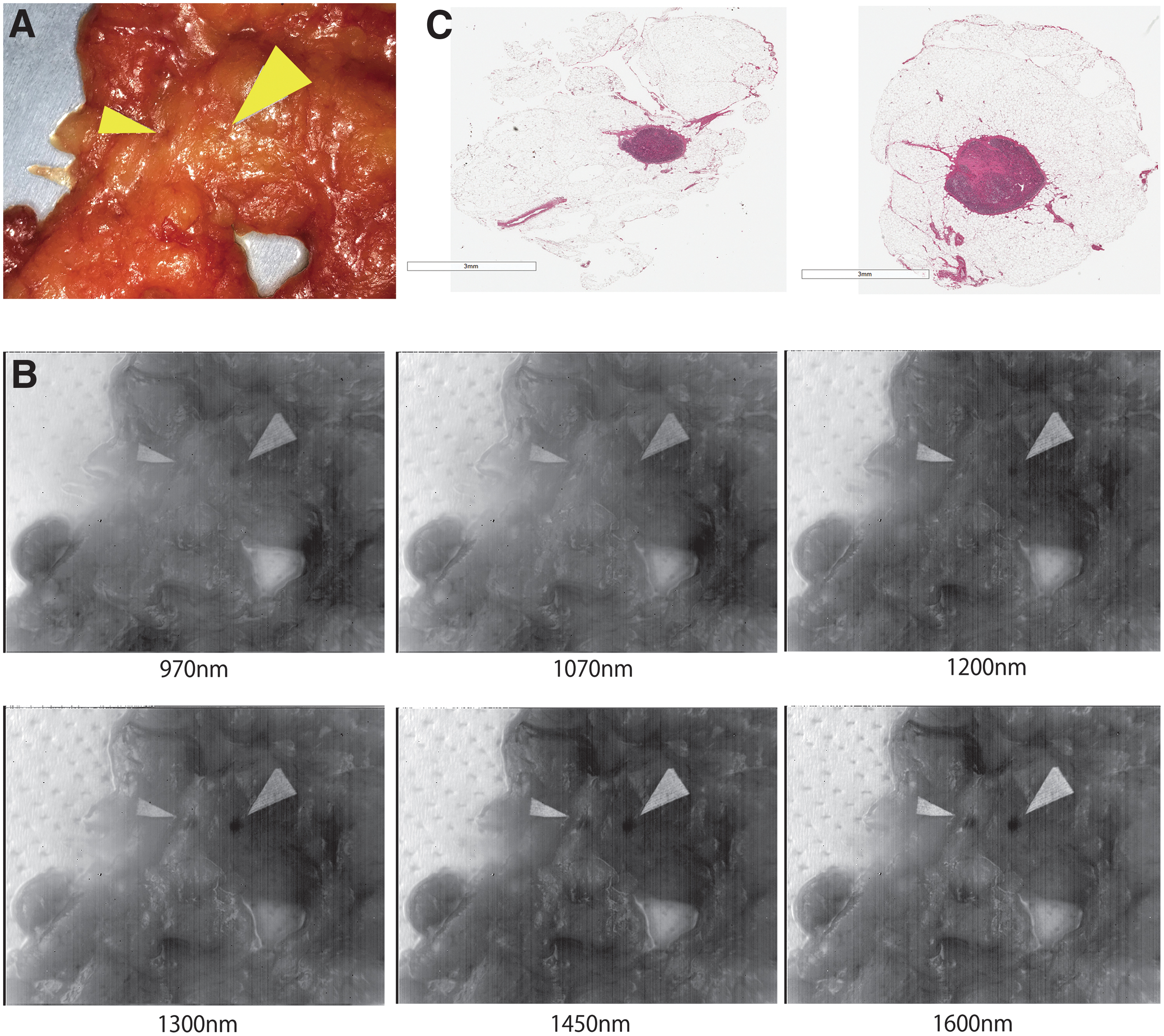
A resected specimen of axillary LN dissection after LN retrieval.
To select the place at which still images were captured, we focused on the findings of two different wavelengths at which the degree of absorbance between water and oil was apparently different (i.e., 970 and 1300 nm). The camera was used to identify the location in which the 970- or 1300-nm light was absorbed. At the place including the identified location, still images of each specimen were simultaneously captured using light at 970-, 1070-, 1200-, 1300-, 1450-, and 1600-nm wavelengths.
In cases in which the 970- and 1300-nm light was absorbed in the selected area, the difference in color of the area was compared between the 970- and 1300-nm images to objectively determine the absorbance. To decide the objective value of the color, L*a*b* coordinate scale was used. In the L*a*b* coordinate scale, high values of the L* component indicated high lightness (the darkest black is at L* = 0, whereas the brightest white is at L* = 100). The value of the L* component of the L*a*b* color coordinate scale at the selected point was measured using the Adobe Photoshop software (CS6; Adobe Systems, San Jose, CA). The difference between the wavelengths was compared statistically.
The selected portion at which light at 970 nm, 1300 nm, or both was absorbed was resected from the specimen with a minimal amount of adipose tissue, fixed in 10% formaldehyde, and observed pathologically (second examination). All specimens assessed in the second examination were categorized into two groups according to their absorbance of light at 1300-nm wavelength. Specimens that absorbed the light at 1300-nm wavelength or at 1300- and 970-nm wavelength were categorized into the high absorbance group (HA group; study group). Specimens that absorbed the light at 970-nm wavelength and did not absorb the light at 1300-nm light were categorized into the low absorbance group (LA group; control group).
In the second examination, the presence or absence of LNs in hematoxylin and eosin staining was recorded, and the ratio of LN identification was compared between the groups. In specimens in which an LN was detected, the maximum diameter of the LN was measured as the size of the LN and the presence or absence of metastasis was recorded. The size of the LN in the second examination was compared with that of the first examination. In specimens in which metastasis was observed, it was investigated whether the presence of the metastasis would affect clinical diagnosis and treatment policy if the LN had been detected in the first examination. In specimens in which an LN was not detected, the structures observed in the specimen, excluding the adipose tissue, were recorded.
Statistical analysis
Statistical analyses among the groups were performed using the JMP statistical software (version 13; SAS Institute, Inc., Cary, NC). A chi-square test was used to compare the ratio of LN identification between the groups. A paired t-test was used to compare the objective difference in color between the groups. An unpaired t-test was used to compare the size of the LN between the first and second examinations. A value of p < 0.05 was considered statistically significant. The data are presented as mean ± standard deviation.
Results
The basic characteristics of the patients are given in Table 1. The mean age of the 20 patients included in this study was 60.2 ± 12.3 years, and the mean body mass index was 22.9 ± 4.6. Of those, seven patients underwent neoadjuvant chemotherapy. The remaining 13 patients did not undergo neoadjuvant chemotherapy, and 4 among 13 patients underwent axillary LN dissection after a positive intraoperative SLNB. In the first examination, an average of 14.1 ± 4.1 LNs were sent for pathological investigation, and LN metastasis was observed in nine cases. The first examination was performed for clinical use. In the first examination, a number of LNs were gathered onto a slide, and each LN was not sliced in their maximum diameter. The number of LNs that were elliptical and coated by a fibrous capsule was 143/250, and their average size was 5.90 ± 3.91 mm.
Basic Characteristics of the Study Patients
ALND, axillary lymph node dissection; BMI, body mass index; LN, lymph node; SLNB, sentinel lymph node biopsy.
In total, 45 specimens were obtained from the remnants of 20 axillary LN dissections obtained from 20 patients. In 17 specimens, the light at 1300-nm wavelength was absorbed, whereas that of 970-nm wavelength was not absorbed. In eight specimens, both 1300- and 970-nm wavelengths were absorbed. In total, 25 specimens were categorized into the HA group (n = 25). Specimens in which the light at 970-nm wavelength was absorbed and specimens in which the light at 1300-nm wavelength was not absorbed were categorized into the LA group (n = 20). The presence or absence of LN was investigated pathologically, and differences between the groups were compared.
The absorbance at each wavelength of the specimens in the HA and LA groups is given in Tables 2 and 3, respectively. In all 25 specimens of the HA group, the absorbance of light at 1450 and 1600 nm was also high (Table 2 and Fig. 1). In contrast, in the 20 specimens of the LA group, light at these wavelengths was not absorbed (Table 3 and Fig. 2).
Absorbance at Each Wavelength and Findings of Lymph Nodes in the Specimens Categorized into the High Absorbance of Light at the 1300-nm Wavelength Group
HA, high absorbance.
Absorbance at Each Wavelength and Findings of Lymph Nodes in the Specimens Categorized into the Low Absorbance of Light at 1300-nm Wavelength Group
Components observed in the pathological specimen other than the adipose tissue and connective tissue.
LA, low absorbance.
In 17 specimens of the HA group, light at lower wavelengths (i.e., 970–1200 nm) was not absorbed. In the remaining eight specimens of the HA group, light at these wavelengths was absorbed. Even in these eight specimens, the value of the L* component in the light at 970-nm wavelength was significantly lower than that of the light at 1300-nm wavelength (48.3 ± 4.2 vs. 29.5 ± 6.9, respectively; p < 0.0001). In all specimens, the lightness was higher in 970-nm light than in the 1300-nm light with a difference of ≥10 for the value of the L* component. In all specimens, higher absorbance was observed at the 1300-nm wavelength than at the 970-nm wavelength (Fig. 3).
According to the pathological findings, one or more LNs were detected in all 25 specimens categorized into the HA group. In contrast, there were no LNs detected in the 20 specimens categorized into the LA group. A statistically significant difference was observed between the groups (p < 0.01) (Table 4). Both the sensitivity and specificity were 1.0. Moreover, the positive and negative predictive values were 1.0.
Correlation Between the Groups Categorized Depending on Their Absorbance at 1300-nm Wavelength and the Presence of a Lymph Node
HA group, high absorbance of light at the 1300-nm wavelength group; LA group, low absorbance of light at 1300-nm wavelength group.
In the HA group in the second examination, one specimen included three LNs, whereas another specimen included two LNs. In these specimens, the size of the largest LN was recorded as the LN size of the specimen. The other 23 specimens included one LN per specimen. In two of them, the size of the LN could not be measured because it was unintentionally cut and did not maintain an oval shape. In second examination, the average size of the LN in 23 specimens in which LN size could be recorded was 3.00 ± 2.93 mm (range: 0.58–15.11 mm, only one LN >5 mm). Although the size of the LNs in the first examination was not measured in their maximum split surface, the size of LNs detected in second examination were significantly smaller than those observed in the first examination (p < 0.01).
Metastasis was observed in 5 of the 28 LNs detected in the second examination. In three of those, there were metastases in the other LNs in the first examination and the TNM staging system was not changed even if the result of the second examination was added to the result of the clinical pathology. However, in two of the specimens, metastasis was observed only in the second examination. If this LN had been promptly detected in the first examination, the adjuvant therapeutic approach for this patient may have been influenced.
LNs were not observed in any of the 20 specimens categorized into the LA group. Regarding the presence of components other than the adipose tissue/connective tissue, blood vessels, muscle, and blood clot were observed in two, two, and three specimens, respectively (Table 3).
Discussion
This was the first study to investigate the absorbance of light by axillary LNs at >1000-nm wavelength using a newly developed near-infrared imaging device with InGaAs element. Light at 1300- to 1600-nm wavelengths was highly absorbed by axillary LNs, unlike in the other components included in the surrounding adipose tissue. It was possible to detect LNs, which were nonpalpable and indistinguishable from the surrounding adipose tissue under visible light. In this study, the accuracy of LN detection was 1.0. Use of the InGaAs camera enabled surgeons to detect significantly smaller LNs in resected tissue than those identified through classical methods.
Metastasis was observed in 5 of the 28 LNs detected in this study. In two specimens, there was no metastasis observed in the first examination performed according to current medical practice. Although a sufficient number of LNs is required in a dissection specimen to provide accurate pathological staging for a variety of carcinomas, there is currently no standard method for the retrieval of LNs.2–9 In breast cancer, it has been reported that a minimum of 10 LNs are required in axillary LN dissection specimens for accurate pathological staging. However, the administration of neoadjuvant chemotherapy results in a reduced number of LNs retrieved in the axillary dissection specimens.5–7,32 Use of a fat dissolution liquid has been proposed to increase the number of LN detected in the resected specimen after LN dissection. However, the usefulness of this liquid for the detection of small, nonpalpable LNs remains to be determined. 33 At present, it is difficult to detect small LNs without the use of methods that damage the surrounding tissue and the lymphatic system.
As given in this study, the clinical application of this newly developed near-infrared camera resulted in an increased number of retrieved LNs. In addition, the establishment of unified criteria for the retrieval of LNs based on objective evaluation may reduce measurement bias among researchers. Moreover, an objective evaluation such as the difference in color may be useful to establish an imaging system for the recognition of LNs in future research.
There are numerous potential clinical applications of this newly developed camera in treating lymphatic systems. In the present surgical treatment—except for palpable large LNs—sampling of LNs requires resection of the adipose tissue, which surrounds them, the lymphatic vessels connected to them, and the surrounding blood vessels. This approach causes obstruction of the blood flow and lymphatic flow. Even patients who undergo only SLNB (i.e., no axillary LN dissection) develop upper extremity lymphedema at a certain rate.34–37 In contrast, a sufficient number of LNs is desired to reduce the false-negative rate of SLNB after downstaging of the axilla using neoadjuvant chemotherapy.36,37 The intraoperative detection of a target LN after chemotherapy is challenging. Therefore, the use of clips has been proposed to reduce the false-negative rate of SLNB.38–42 The clips are placed as a mark in the metastatic LN before the initiation of chemotherapy, and the clipped tissue including the LN is removed after chemotherapy. The in vivo use of this camera for clinical purposes may assist surgeons in distinguishing small LNs, which are nonpalpable and nonvisible under visible light intraoperatively without using an isotope, contrast medium, or dye. Consequently, this approach may lead to LN sampling with minimal damage to the surrounding tissue.
This technology may be applied to lymphatic microsurgeries, aiming to improve extremity lymphedema. Although vascularized LN transfer has been clinically applied for over a decade, there is no way of viewing small LNs during flap harvesting and accurately counting the number of LNs included in the flap.10–15 Although the results of animal model and clinical studies have shown that an increased number of LNs in the flap is associated with a more rapid transportation of lymphatic fluid and larger volume reduction of the limb, there is no way of accurately counting the number of LNs included in the flap.43,44 The in vivo use of this camera may permit the accurate counting of the number of LNs included in the flap intraoperatively.
Primary surgical prevention techniques for extremity lymphedema have been reported.45–47 Thus, a possible future surgical treatment to prevent lymphedema may involve minimally invasive LN sampling and simultaneous reconstruction of lymphatic flow, as necessary. 4 Use of the InGaAs camera in vivo will visualize the small LNs and determine the necessity of simultaneous lymphatic flow reconstruction.
This study showed that small, nonpalpable LNs surrounded by adipose tissue may be detected using the newly developed InGaAs camera. However, this method is characterized by limitations. First, although all LNs absorbed light at 1300- to 1600-nm wavelength, the optimal wavelength to distinguish LN from the surrounding fat was not determined in this study. Of note, a proportion of LNs weakly absorbed light at lower wavelength (i.e., 970–1200 nm). Moreover, there was no tendency observed depending on the presence or absence of metastasis in the specimens analyzed in this study. Future studies are warranted to determine the optimal conditions for the clear detection of LNs. Moreover, the differences between LNs with and without metastasis should be investigated using larger numbers of specimens. Second, the exact size and depth at which LNs may be detected through this approach remain to be determined. Future studies are warranted to determine these parameters for the detection of nonvisible LNs.
Conclusion
Light at 1300-, 1450-, and 1600-nm wavelengths was absorbed by axillary LNs, unlike in the surrounding adipose tissue and other components. Using the newly developed InGaAs camera, it was possible to detect LNs, which were nonpalpable and indistinguishable from the surrounding adipose tissue under visible light.
Footnotes
Acknowledgment
The authors acknowledge the excellent technical assistance of M. Shimozawa for the histological analyses.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.