
Abstract
Background:
The current belief is that the calcium channel blocker (CCB)-induced edema is due to a preferential arterial over venous dilatation leading to increased fluid filtration. We challenged this conviction by measuring the lymphatic removal of interstitial fluid during chronic systemic treatment with the CCB, amlodipine. Lymphatic vessels could potentially be an off-target effect of the drugs and play a role in CCB edema.
Methods and Results:
Sixteen healthy postmenopausal women completed a 12-week double-blinded randomized placebo-controlled crossover trial. Lymphatic function was assessed by near-infrared fluorescence imaging. The lymphatic function during amlodipine treatment compared with placebo did not show any difference in pumping pressure (53.9 ± 13.9 mmHg vs. 54.7 ± 9.4 mmHg, p = 0.829), contraction frequency (0.4 ± 0.2/min vs. 0.4 ± 0.3/min, p = 0.932), refill time (440 ± 438 seconds vs. 442 ± 419 seconds, p = 0.990), or propagation velocity of lymph packets (18 ± 10 mm/s vs. 15 ± 7 mm/s, p = 0.124). However, the subjects who developed edema during CCB treatment had a 20% lower baseline lymphatic pumping pressure (48.9 ± 4.4 mmHg, n = 7) than the subjects not affected by treatment (59.1 ± 1.2 mmHg, n = 9, p = 0.025). Contraction frequency, refill time, and lymph packet velocity showed no differences in baseline values between the two groups.
Conclusion:
Our results suggest that CCB does not directly impair lymphatic function. However, our results show that a reduced lymphatic function predisposes to CCB edema, which may explain why some patients develop edema during treatment.
Introduction
Calcium channel blockers (CCBs) of the dihydropyridine class are part of the first-line treatments for hypertension1,2 and lower limb edema is a common adverse effect. According to numerous clinical studies, edema occurs in 9%–33%3–10 of patients receiving the drugs and 5%–9% discontinue treatment due to this side effect.3,5,9 Higher age and female gender are risk factors for developing edema.9–12
The blood pressure lowering effect of CCBs is caused by reduced calcium influx through L-type calcium channels in the arterial smooth muscle cells. Lower intracellular calcium levels lead to decrease in arterial tone, which reduces peripheral resistance, subsequently lowering blood pressure. The preferential arteriolar over venous dilatation leads to an increase in hydrostatic pressure in the capillaries and thereby a rise in fluid filtration, which is widely accepted as the cause of CCB edema.13–16 As dictated by the Starling force, an estimated 8 L of fluid is daily filtered out of the blood circulation to the interstitial space under normal conditions and returned to blood circulation through the lymphatic vessels.17,18 An increased fluid filtration does not constitute a problem per se as long as the lymphatic vessels are capable of removing the extra fluid load.17,19
Lymphatic fluid transport depends on coordinated intrinsic contractions of the lymphatic vessels, 20 which possess smooth muscle cells in the vessel wall. Valves divide the vessel into functional contractile segments (lymphangions). This series of contracting lymphangions are coined the “lymph pump.” 21
We have previously shown that voltage-gated calcium channels are essential for generating phasic contractions in human lymphatic vessels ex vivo 22 and that therapeutic concentration of CCBs completely inhibits lymphatic contractility. 22 How these findings translate to in vivo is unclear. Reduced lymphatic removal of interstitial fluid could be an off-target effect of CCBs that play a role in the pathogenesis of CCB edema.
We hypothesize that chronic treatment with high-dose amlodipine in postmenopausal women decreases lymphatic function in the lower leg assessed in vivo by near-infrared fluorescence (NIRF) imaging.
Materials and Methods
Study population
The inclusion criteria were postmenopausal women. Exclusion criteria were arterial hypotension, orthostatic hypotension, angina pectoris, previous acute myocardial infarction, previous gastrointestinal bleeding, peripheral edema at inclusion in the trial, currently under treatment with any type of CCB, angiotensin converting enzyme inhibitor, or angiotensin-receptor blocker, and allergy against anything contained in the tablets. Subjects stating unexplainable loss of consciousness during the ast 5 years were also excluded.
Informed consent was obtained from all participants and were assessed for eligibility and included by S.M.
Study design
The trial was designed as a randomized double-blinded placebo-controlled crossover trial, wherein each subject underwent two treatment periods of 12 weeks, one period with Amlodipine Actavis and the other period with placebo. Lymphatic function was assessed after each period using NIRF imaging. There was a 4-week washout period between each administration period. The order was randomized to start with either amlodipine or placebo. During the first 8 weeks, the dose was 5 mg (1 capsule) amlodipine or placebo per day. During the last 4 weeks, the dose was increased to 10 mg (2 capsules) (Fig. 1). Amlodipine Actavis and placebo pills were packed in identical empty hard gelatine capsules (CAPSUGEL) to blind the subjects and investigator.
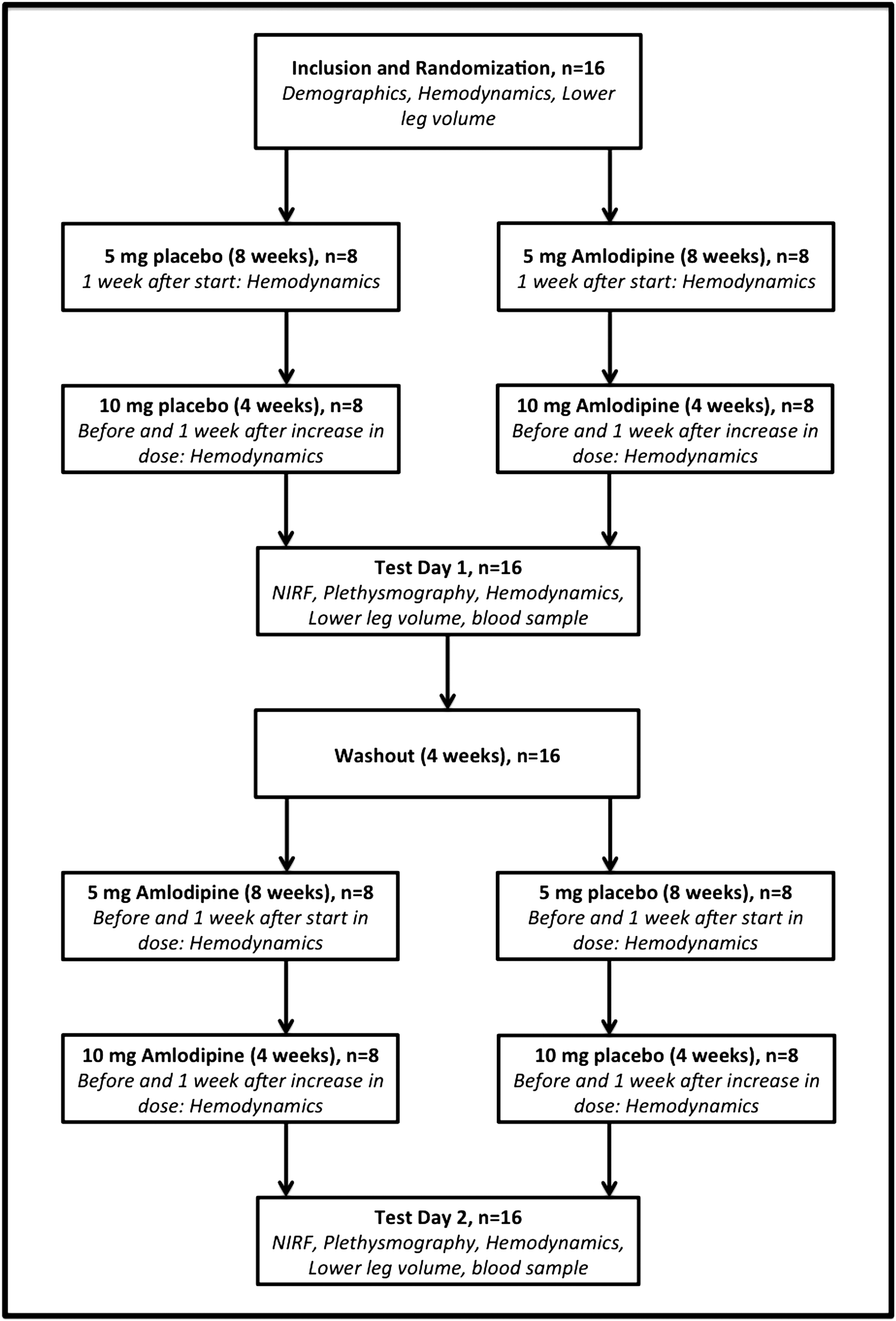
Flowchart of study design. NIRF imaging, near-infrared fluorescence imaging.
The study subjects were included from June 2016 to April 2017 in four blocks of four subjects and assigned a unique number (1–16). The trial was completed in October 2017. Aarhus University Hospital Pharmacy performed randomization and blinding. The subjects were instructed to take the capsules at the same time each day.
If a subject wished to stop treatment because of edema, lymphatic function was assessed before medication was terminated and the subject remained included in the study.
A 4-hour protocol using NIRF imaging was performed at Aarhus University Hospital on each of the test days.
Blood pressure, pulse, body weight, height, and lower leg volume were measured before randomization and on the 2 days of test (Fig. 1).
Study protocol
NIRF imaging
Lymphatic vessels in the right lower leg were examined using NIRF imaging, a custom-built near-infrared camera setup, as described previously.22,23 In brief, the fluorescent dye indocyanine green (ICG; Diagnostic Green, Germany) was dissolved in sterile water before diluting in isotonic saline to reach a final concentration 0.3 g/L. ICG, (30 μg; 0.1 mL) per injection, was injected in three locations, on the right foot. The injections were placed intradermally with 31G needles (Wiotech, Denmark) behind the medial malleolus and distally in the first and fourth intertarsal space after 15 minutes of acclimatizing to room temperature (23°C–27°C) and resting position in a standard hospital bed to avoid any extrinsic influence on the lymphatic function during testing.
The ICG was excited using a custom-designed 785 nm 450 mW laser (Power Technology, Alexander, AR), with a 780 ± 28 nm band-pass filter, and the emitted fluorescence dye was collected using an electron-multiplier charge-coupled device camera (C9100-13 Hamamatsu, Japan), with a Navitar lens (25 mm f0.95) with two 835 nm ±15 nm (>OD5) band-pass filters.
Image acquisition began 20 minutes after injection to allow for a sufficient dye uptake in the lymphatic vessels. 23 Four NIRF imaging sequences were obtained during the protocol. First, an injection sequence of the right foot was acquired (Supplementary Movie S1). Next, an 8-minute baseline NIRF imaging acquisition sequence of the lower leg was captured in a complete supine and resting position (Supplementary Movie S2). Finally, refill time and pumping pressure were assessed in two separate NIRF imaging sequences.
Human lymphatic function: quantification
Quantification of lymphatic function was determined offline using ImageJ (NIH, Bethesda, MD) and a custom-written LabVIEW program (National Instruments, Austin, TX). The following dynamic parameters were assessed as primary outcomes to describe function: pumping pressure, contraction frequency, refill time, and velocity. All data were analyzed blinded twice by S.M. and B.K., and interobserver variation was calculated.
All measurable vessels in each sequence were used in the assessment of contraction frequency, refill time, and velocity. In each corresponding sequence from the two different test days, regions of interests (ROIs) were plotted in the same measureable vessels for each specific participant (Fig. 2).

Raw data trace from NIRF imaging.
Pumping pressure
Pumping pressure was defined as the maximal pressure the lymphatic vessels can pump against. A Hokanson sphygmomanometer cuff (Marcom Medical, Denmark) was used to occlude lymphatic flow. Before occlusion, the lymphatic vessels in the calf were emptied for lymph fluid by manual massage while blocking the lymph flow with a tourniquet placed above the malleolus. The sphygmomanometer cuff placed around the calf was inflated to 70 mmHg using an accurate (±1 mmHg) cuff system (Hokanson E20 Rapid Cuff Inflator, Hokanson AG101 Air Source, SC10 Cuff; Marcom Medical). The distally placed tourniquet, preventing lymph flow, was detached and the pressure in the cuff was decreased in 5 mmHg steps every fifth minute until lymph passed the cuff, proving that the lymphatic pumping exceeds pressure in the cuff. The pressure was noted and the cuff was deflated.
Contraction frequency
A rise in intensity combined with/or a visual verification of a lymph package moving through a ROI was defined as a contraction. In the LabVIEW program, the raw signals of the contractions in the ROIs were seen as positive spikes. The contractions were also depicted in a differentiated plot (signal/time), where a contraction was seen as a transient complex of a positive deflection followed by a negative deflection. The frequency was determined by counting the number of negative deflections over the obtained 8-minute sequence (Fig. 2).
Refill time
As already described, under pumping pressure the lymphatic vessels of the calf were emptied by manual massage. After removing lymph from the vessels, the tourniquet placed above the malleolus to block lymph flow was detached and refilling of vessels was allowed. The average time required to refill 5 cm of vessels in three consecutive measurements was defined as refill time.
Packet velocity
The propagation velocity of lymph packets after contractions was measured in 5–10 cm straight vessels with a ROI placed at each end of the vessels. Only packets moving through both ROIs without any delay were included in the calculations. Velocity was determined by taking the time required for the lymph packets to move from one ROI to the other and divide it by the distance between the two ROIs.
Secondary outcomes
Lower leg volume
Water displacement was used to estimate lower leg volume. A custom-built container was filled with 25 cm of 30°C water after which the participant placed the right foot and lower leg in the container. The displaced water, equivalent to the lower leg volume, emptied through a hole on the side of the container and was weighed with a scale. The lower leg volume was determined as the average of three repeated measurements. 10
Hemodynamics
Blood pressure and pulse were measured in seated subjects on the left arm with a manual sphygmomanometer, and the average of three measurements was noted. Blood pressure and pulse were measured 2 days before start of intake of capsules, 1 week after taking the capsules, before increase of doses, 1 week after increase of dose, and on the 2 days of test, in total 10 times (Fig. 1).
Measurement of amlodipine concentration in plasma
A 4 mL blood sample was taken two times, on either test day. All freshly drawn blood samples were centrifuged at 2000 × g for 10 minutes and the resulting plasma fractions were transferred to new tubes and then stored at −20°C until analysis in the research biobank at the Department of Forensic Medicine at Aarhus University Hospital. All analyses were performed at the same time after the last test of the study. Quantification of amlodipine in human plasma samples was based on methodologies previously developed and validated in our laboratory. 24
Deuterium-labeled amlodipine (Amlodipine-d4, Toronto Research Chemicals) was used as internal standard and a 7-point calibration was performed in separate blank plasma samples spiked with defined amounts of amlodipine reference material (Amlodipine besylate, Cat. No. A5605; Sigma Aldrich) in the range of 0.1–100 μg/L. Amlodipine extraction was analyzed by ultra-high performance liquid chromatography mass spectrometry essentially as previously described. 24
Capillary filtrations rate
In the original design as described in clinicaltrialsregister.eu we aimed to measure the capillary filtration rate. Owing to technical difficulties, the method was excluded.
Ethical approval
The clinical drug trial, Lymphatic dysfunction as a cause of calcium channel blocker edema in postmenopausal women, was approved by The Central Denmark Region Committees on Health Research Ethics (1-10-72-203-15), Danish Health and Medicine Agency, and the Danish Data Protection Agency. The study is registered in clinicaltrialsregister.eu (EudraCT No.: 2015-001761-11).
The study subjects participated voluntarily and after a written informed consent was signed. The study was conducted in accordance to the Helsinki declaration and monitored by the Good Clinical Practice unit in Region Midt, Denmark.
Statistics
NIRF imaging was analyzed as already explained. Data storage was done in Microsoft Excel, whereas GraphPad Prism and Stata/SE 15.1 were used for all statistical analyses and graphical presentation of the data. All data were tested for normality and presented as mean ± standard deviation (SD) and for significance with paired and unpaired Student's t-test (data with two samples). Significance level was set to 0.05 in all tests.
Interobserver agreements were tested using the intraclass correlation (ICC) coefficient calculated with a two-way mixed model for absolute difference between two measurements. 25 The ICC coefficient is presented with 95% confidence intervals.
Based on a mean pumping pressure found in our NIRF imaging validation study 23 of 56.5 mmHg and a SD of 9 mmHg, a total of 16 study subjects were needed for this two-treatment cross-over study with a probability of >83% for detection of a treatment difference at a two-sided 0.05 significance level, if the true difference between treatments is 10 mmHg. All data were analyzed before unblinding of data. The trial is reported according to the CONSORT 2010 guidelines for reporting a randomized clinical trial.
Results
Study population
The 16 postmenopausal women included in the study had a mean age of 56.5 ± 6.9 years. None of the subjects were excluded during the trial or lost to follow-up. The demographical and clinical characteristics of study subjects are described in Table 1. The blood pressure in the subjects was at randomization 128 ± 14 mmHg/80 ± 9 mmHg and average mean arterial pressure was significantly lowered after treatment with 5 mg amlodipine and further lowered after 10 mg amlodipine (Table 2). Heart rate was unaffected throughout the trial (71 ± 11/min vs. 71 ± 9/min, p = 0.936). The mean plasma concentration of amlodipine was 18 ng/mL (range: 9–29 ng/mL) after 3 months of treatment and similar to plasma concentrations found in previous studies (6–24 ng/mL).26–28
Demographics and Clinical Characteristics
Data are presented as means ± standard deviation.
BMI, body mass index; BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Clinical Characteristics and Changes to Amlodipine Treatment
Data are presented as means ± standard deviation.
Seven of the 16 women developed clinical edema during amlodipine treatment and had edema with pitting at the time of testing with an average increase of lower leg volume from 1.64 ± 0.21 L during intake of placebo to 1.72 ± 0.22 L under amlodipine treatment (p = 0.012). In comparison, the group of patients who did not develop edema during the trial had almost no change in lower leg volume from 1.53 ± 0.39 L under placebo to 1.56 ± 0.34 L during amlodipine treatment (p = 0.579) (Table 2; Fig. 2c). There were no differences in age (57 ± 2 years vs. 55 ± 3 years, p = 0.557) or body mass index (25.9 ± 1.6 vs. 25.8 ± 2.0, p = 0.970) between the women not developing edema during amlodipine treatment and with those who did.
NIRF imaging
Dynamic parameters: amlodipine versus placebo
Pumping pressure in the lower leg lymphatic vessels was similar in the subjects during amlodipine treatment, 53.9 ± 13.9 mmHg, and placebo intake, 54.7 ± 9.4 mmHg (p = 0.829; Fig. 3a). Contraction frequency was comparable during amlodipine treatment, 0.4 ± 0.2/min, compared with during placebo, 0.4 ± 0.3/min (p = 0.932; Fig. 3b). There was no change in refill time for the amlodipine period, 440 ± 438 seconds, compared with the placebo period, 442 ± 19 seconds (p = 0.990; Fig. 3c). The velocity by which the lymph was propelled forward after each contraction (packet velocity) was not different between the amlodipine period, 18 ± 10 mm/s, and the placebo period, 15 ± 7 mm/s (p = 0.124; Fig. 3d). The continuous movement of lymph was measured over an average distance of 61 ± 10 mm. The average number of vessels analyzed per subject was 3.4 ± 1.2 and was not different between the 2 days of test (p > 0.999).

Dynamic parameters estimated with NIRF imaging comparing amlodipine with placebo.
To clarify whether CCB treatment had any influence on lymphatic function during placebo after crossover in the group receiving CCB in the first period, we compared the placebo results after separating the study population in the two groups according to when they received placebo. The results showed no significant difference between the two groups, suggesting that CCBs did not have any influence on placebo data.
Dynamic parameters: edema versus no edema
To further examine the mechanism of CCB edema, we divided the cohort into two groups (edema with treatment versus no edema with treatment) and compared the placebo values between the groups as well as the change in parameters after treatment with amlodipine. Placebo pumping pressure in the lower leg lymphatics was lower in the subjects (n = 7) developing edema during amlodipine treatment, 48.9 ± 4.4 mmHg, than that in the subjects not developing edema during treatment with amlodipine (n = 9), 59.1 ± 1.2 mmHg (p = 0.025; Fig. 4a). The change in pumping pressure from baseline (−2.9 ± 17.4 mmHg vs. 0.8 ± 12.05 mmHg) was not different (p = 0.623) with amlodipine treatments. Baseline (placebo) contraction frequency was comparable between the group with edema 0.4 ± 0.1/min and those without edema 0.5 ± 0.1/min (p = 0.418; Fig. 4b). This was also the case during amlodipine treatment, where the edema subjects had similar (p = 0.525) change in contraction frequency (0.06 ± 0.3/min vs. −0.04 ± 0.3/min). There was no difference in baseline (placebo) refill time in the subjects with edema, 551 ± 161 seconds, compared with the subjects without edema 356 ± 139 seconds (p = 0.375; Fig. 4c). The same was seen during amlodipine treatment, where the subjects with edema had no difference (p = 0.414) in change in refill time compared with the nonedematous subjects (92 ± 546 seconds vs. −74 ± 214 seconds). The baseline velocity by which the lymph was propelled forward after each contraction was not different between the subjects developing edema, 13 ± 2 mm/s, and nonedematous subjects, 17 ± 3 mm/s (p = 0.282; Fig. 4d). No difference in the change in velocity during amlodipine treatment (p = 0.661) was found between the two groups (3.5 ± 8.5 mm/s vs. 2.0 ± 5.1 mm/s).
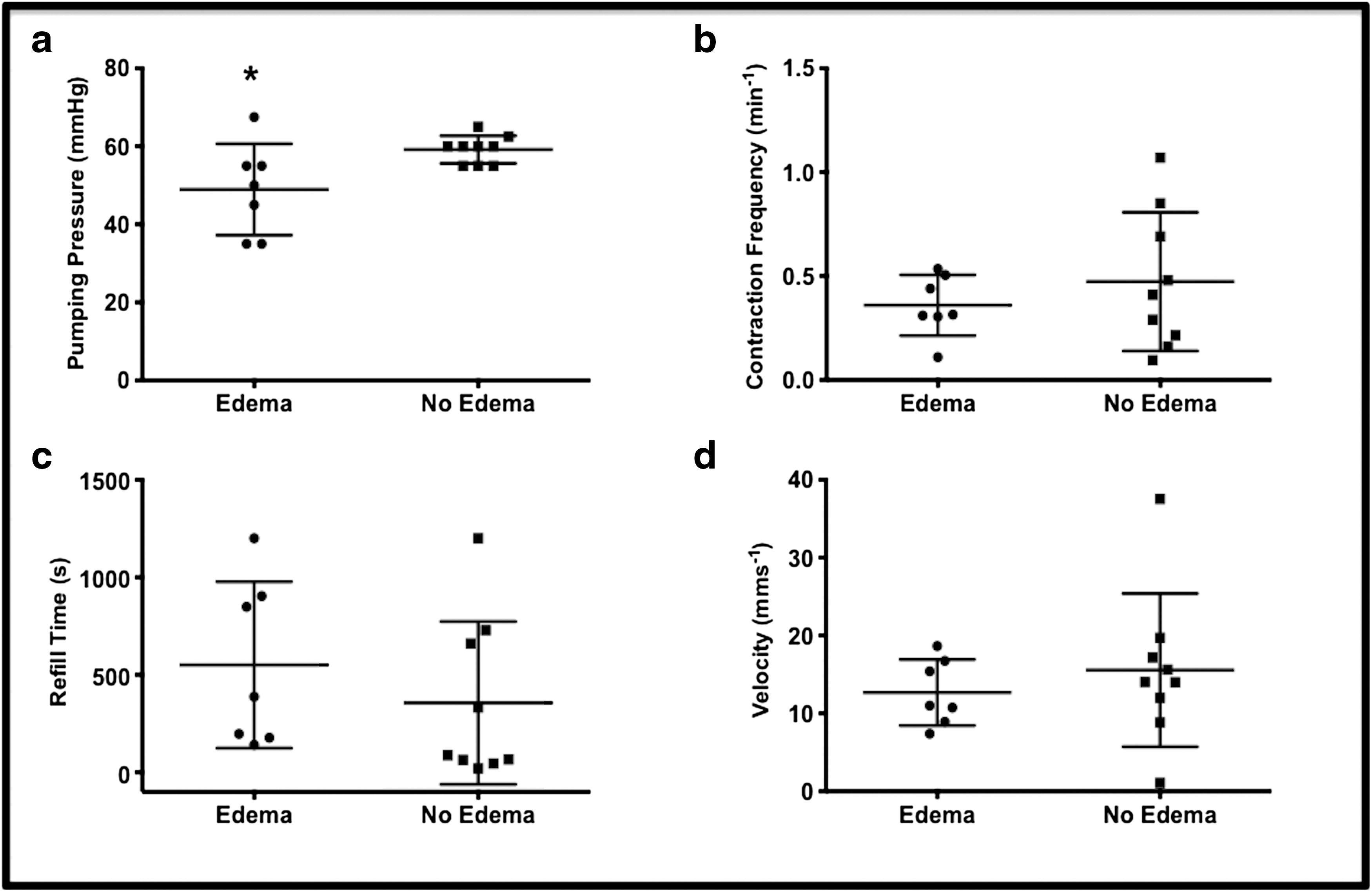
Dynamic parameters estimated with NIRF imaging comparing amlodipine related edematous subjects (black circle, n = 7) and nonedematous (black square, n = 9) subjects.
Interobserver reliability
We found an interobserver ICC coefficient of 0.99 in pumping pressure estimation, and for contraction frequency ICC coefficient was of 0.98. The calculations for these two parameters consisted of 16 pairs of observations. The calculations for velocity measurement consisted of only 12 pairs of observations with an ICC coefficient of 0.69.
Discussion
In this randomized double-blinded clinical trial, we demonstrate that a reduced lymphatic function predisposes to CCB edema, as demonstrated by the 20% reduced lymphatic pumping pressure in the group of patients who developed edema during treatment compared with the group of patients who did not develop edema. Our data do not support our hypothesis that CCBs have a direct effect on the lymphatic vessels.
CCB edema
CCB edema occurs more often in women and is reported in a comprehensive meta-analysis from 2011 to be up to 11% in patients treated with a CCB. 5
It has long been widely accepted that the pathophysiology behind this common side effect is caused by a preferential precapillary over postcapillary dilatation, leading to increased fluid filtration.13–16 In any patient with edema, the lymphatic load (filtration of fluid) exceeds the maximal lymphatic transport capacity. This does not automatically equate to a lymphatic dysfunction or defect. But our study gives the insight to why patients react differently to the same exposure, where some develop edema while others go free. Our results indicate that the patients who develop edema during CCB treatment have a lower threshold for developing edema in general, shown by the lower maximal lymphatic transport capacity during placebo treatment.
We have previously demonstrated that the smooth muscle cells in human lymphatic vessels express Cav1.2 and that clinically relevant concentrations of CCB nifedipine ex vivo CCB abolish lymphatic pumping. 22 In the same study, we exposed a small group (n = 6) of young healthy male volunteers to a short treatment course (12 days) of high-dose nifedipine (final dose 90 mg) without finding any inhibitory effect of the drug on the lymphatic vessel function, change in foot volume, blood pressure, or pulse. 22 On the contrary, we found an increased contraction frequency and refill time, which we interpreted as a compensatory response to increased fluid filtration. Elderly, however, respond differently to CCBs and, in particular, elderly women are prone to develop edema in contrast to young individuals.5,10,12,29 The duration of treatment is also of importance since CCBs require up to 3 months to exert their full effect.13,29 The results from our pilot study with the young males, treated with high-dose nifedipine for 12 days, can, therefore, not be extrapolated to a clinically relevant setting. 22
Functional data
In this study, we treated elderly women for 3 months with a high dose of amlodipine. Our treatment was effective since blood pressure drop was seen in 15 of 16 subjects, edema in 7 of 16 subjects, foot volume increased in 13 of 16 subjects, and plasma amlodipine was comparable with other studies (Table 2).26–28 Our results showed that blood pressure drop was equal in the edematous women and the nonedematous women, indicating a vasodilatory response similar to CCB treatment. In conclusion, our attempt to create a setting to study the effect on the lymphatic vasculature of CCB treatment was successful. Despite this, we found no alteration of lymphatic function of CCB treatment. Subgroup analysis of the subjects with and without edema did not show any affect on lymphatic vessels either. Our data thus do not support our hypothesis and ex vivo data that CCBs impair lymphatic pumping. The major contributor to edema must thus be assumed to be increased fluid filtration, in accordance with the common conception of the pathophysiology of CCB edema, although this was not measured in this study. One would expect that increased fluid filtration would lead to a compensatory increase in lymphatic pumping, which was what we found previously in young healthy subjects. 22
Interestingly, we saw no compensatory increase in contraction frequency or refill time in this study. 22 This difference, in the elderly, suggests that the compensatory capacity of the lymphatic vessels toward an increased fluid filtration may be challenged. To try to elucidate why some subjects developed edema, we compared the lymphatic function during placebo treatment between those who developed edema and those who did not. We here found that those who developed edema had a lower pumping pressure, whereas all other parameters were similar. Mean pumping pressure has been shown to decline after age 60 years, especially in women.30,31
The explanation for the reduced baseline function in the subgroup of subjects with edema as well as why pumping decreases with age, especially in women, is interesting to speculate upon and could overlap. Venous insufficiency might be part of the explanation of this since both age and gender are a risk factor 32 and it has been shown that lymphatic function is reduced in patients with venous insufficiency. 33 However, none of the healthy subjects was diagnosed with venous hypertension before or during the study. Subjectively no problems were described regarding chronic venous insufficiency. Objectively no spider or varicose veins was observed at inclusion. But we cannot rule out that some of the postmenopausal subjects had asymptomatic venous reflux, because ancillary testing was not conducted.
Hormonal changes might also play a role since estrogen is known to influence endothelial nitric oxide production,34,35 which is a strong modulator of lymphatic pumping.36–38
Finally, inborn genetic predisposition for edema formation is a theory still widely discussed and further studies need to be conducted. 39
Limitation
Two main limitations must be mentioned: first, although the plasma concentration of CCB reached therapeutical levels in the study during treatment, the interstitial fluid concentrations of the drug are not known; second, even though none of the participants had venous hypertension or documented venous insufficiency, we cannot rule out asymptomatic venous reflux, because ancillary testing was not conducted.
Clinical importance
In the state-of-the-art review by Mortimer and Rockson, 19 they conclude that all chronic edema indicate a lymphatic inadequacy or failure of lymph drainage and that more than one physiological factor contributes to chronic edema. We believe that this study highlights this. The increased fluid filtration by the CCB does not constitute a problem as long as the lymphatic drainage is adequate, but reduced lymphatic function increases the risk of edema. The lack of compensatory increase in contraction frequency and reduced pumping pressure could explain why the elderly more frequently develop edema during CCB treatment. Although we did not find a direct inhibitory effect of CCBs on the lymphatic vessels, treatment might indirectly be detrimental due to chronically increased fluid load. But this probably requires longer follow-up than the 3-month study period in this study.
Conclusions
In this study, we are the first to demonstrate that reduced lymphatic function predisposes to developing peripheral edema during CCB treatment. Long-term treatment with CCBs might aggravate this. The development of CCB edema should make the clinician aware that the patient has a poor functional lymphatic reserve capacity. Our results do not suggest that CCBs have a direct inhibitory effect on the lymphatic vasculature.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.