
Abstract
Background:
Bioimpedance spectroscopy (BIS) demonstrates proficiency in early identification of breast cancer treatment-related lymphedema (BCRL) development. Dual-tab electrodes were designed for consistent and easy electrode placement, however, single-tab electrodes positioned to mimic dual-tab placement on the body may make BIS technology more accessible in community hospitals and outpatient settings. The purpose of this study is to evaluate use of single-tab electrodes for BIS measurements and assess whether single-tab electrodes provide consistent BIS measurements in controls and patients with BCRL.
Methods and Results:
Upper limb BIS ratios were obtained using ImpediMed L-Dex® U400 in controls (n = 13; age = 23–75 years; 9 repeated measurements) using dual-tab and single-tab electrodes. BCRL patients (n = 17; Stage = 1.65 ± 0.49; number nodes removed = 16.3 ± 7.7; age = 50.9 ± 10.6 years; age range = 33–77 years) and healthy controls (n = 19) were evaluated to determine if single-tab electrodes provided discriminatory capacity for detecting BCRL. Intraclass correlation coefficients (ICC), linear mixed-effects models, Wilcoxon rank-sum tests, and linear regression with two-sided p-values <0.05 required for significance were applied. Single-tab electrodes were found to be statistically interchangeable with dual-tab electrodes (ICC = 0.966; 95% confidence interval = 0.937–0.982). No evidence of differences in single-tab versus dual-tab measurements were found for L-Dex ratios (p = 0.74) from the linear mixed-effects model. Repeated trials involving reuse of the same electrodes revealed a trend toward increases in L-Dex ratio for both styles of electrodes. Single-tab electrodes were significant (p < 0.0001) for discriminating between BCRL and control subjects.
Conclusion:
Findings expand upon the potential use of BIS in clinic and research settings and suggest that readily available single-tab electrodes provide similar results as dual-tab electrodes for BIS measurements.
Introduction
As survival rates from breast cancer continue to improve, treatment comorbidities such as breast cancer treatment-related lymphedema (BCRL) are becoming increasingly recognized. BCRL results from a compromise in the lymphatic processing capacity relative to the lymphatic load frequently initiated by damage to axillary lymph nodes secondary to sentinel node biopsy or lymph node dissection. A review of 30 prospective breast cancer clinical trials determined a high 21.4% incidence rate of BCRL after breast cancer treatment, 1 highlighting the need to improve our understanding of lymphedema etiology and early biomarkers of lymphatic vulnerability that could be used to guide prophylactic therapies and early intervention.
Surveillance models for early BCRL detection are advocated for in the literature2–6 and are also a component of clinical guidelines proposed by the National Comprehensive Cancer Network and the National Lymphedema Network. BCRL surveillance models commonly recommend obtaining presurgical bilateral arm extracellular fluid or circumferential measurements using a consistent protocol. Repeated measurements are recommended for ongoing longitudinal assessment and encouraged to be repeatable independent of the clinic or clinician.
However, commonly used volumetric and circumferential limb measurements identify relatively late-stage changes in limb volume induced by lymph stasis. Bioimpedance spectroscopy (BIS) is a promising portable technology that could be used more often in most clinics as an alternative or adjunct to limb circumference measurements to detect BCRL onset and progression,3,7–9 given its increased potential for earlier detection and interrater reliability. The commercially available BIS devices, L-Dex® U400 and SOZO (ImpediMed, Mansfield, Australia), are Food and Drug Administration (FDA) approved devices for clinical use and provide surrogate markers of extracellular fluid levels.
When using the L-Dex U400, dual-tab electrodes are applied to the skin and a subsensory alternating current is applied to detect the amount of opposition to current flow in the right and left limbs. Higher levels of extracellular fluid are tightly correlated with lower impedance measures.7,10 By sampling multiple frequencies in the range 5–1000 kHz, 11 the BIS measurement provides information on impedance of extracellular fluid 12 and the device calculates an impedance ratio value (L-Dex ratio) relative to normative values, 13 after correcting for small biases due to hand dominance.7,14,15 Clinicians may use the BIS values to monitor disease progression, where an increase of ≥7.1 in the L-Dex ratio corresponds with potential lymphedema onset.8,14 While BIS continues to be evaluated for its effectiveness,10,16–20 the ease of obtaining a BIS measurement8,14,20,21 and potential for patient self-monitoring22,23 are major, well-accepted advantages of this technology.
BIS measurements for the L-Dex U400 are recommended by the manufacturer to be obtained using dual-tab electrodes for a standard placement of electrodes using the manufacturer's identified body landmarks for the hands and feet. However, BIS measurements have not yet been tested using more commonly available single-tab electrodes positioned to mimic the dual-tab electrode placement, which would still preserve the importance of having standardized body landmarks for interpretation of data results. This comparison is fundamental as single-tab electrodes are inexpensive and readily available in most medical centers and outpatient clinics. Investigation of standardized placement of single-tab electrodes for BIS measurements mimicking dual-tab placement could therefore greatly increase the accessibility of this important technology in clinical and research settings, where reimbursement for new devices, associated consumables (i.e., electrodes), and BIS technology software may be limited. The purpose of this study is to (1) evaluate whether single-tab electrodes, when positioned similarly to dual-tab electrodes, provide reproducible and consistent BIS measurements (L-Dex ratios) and (2) determine whether BIS measurements obtained using single-tab electrodes provide discriminatory information in patients with BCRL and age-matched controls, as has already been shown for dual-tab electrodes. 22 We will also outline best practices for standardizing the use of single-tab electrodes when obtaining BIS measurements.
Materials and Methods
Single-tab versus dual-tab electrodes
All participants provided informed, written consent for this Institutional Review Board-approved study and were enrolled as part of the prospective trial Imaging Noninvasively with Functional-MRI for Onset, Response, and Management of Lymphatic Impairment (INFORMLI; ClinicalTrials.gov identifier = NCT02611557). The first goal was to evaluate the repeatability and reproducibility of the BIS measurements using dual-tab and single-tab electrodes. To achieve this, using the L-Dex U400 (ImpediMed, Mansfield, Australia), we obtained 18 upper limb L-Dex ratios for each healthy participant (n = 13; age = 23–75 years) in a single visit. All control volunteers were without medical histories of lymphedema, risk of lymphedema, or other edematous conditions at the time of participation.
Dual-tab electrodes were purchased from ImpediMed ($500 for 60 electrodes) and 3M single-tab electrodes from an online distributor ($5.40 for 60 electrodes). Each L-Dex reading requires three dual-tab electrodes ($24.99/measurement) or five single-tab electrodes ($0.45/measurement). As such, there is an approximate cost difference of $24.50 per participant at the time of this study, a more than a 55-fold reduction in fractional cost by using the single-tab electrodes.
To obtain the BIS measurements using either dual-tab or single-tab electrodes, the electrodes were positioned as recommended by the manufacturer on the wrists and right foot. Three trials of L-Dex ratios were taken consisting of three repeated measures in every trial for both the dual-tab (ImpediMed) electrodes and single-tab (3M Red Dot Electrode #2360) electrodes. The style of electrode (dual-tab vs. single-tab) used first was randomized between participants. Following each electrode trial, we carefully removed the electrodes, placed them on their original plastic sheet to be reused on the same volunteer until all three trials were completed for each style electrode. We then placed the alternative electrode style on the participant. We continued using this alternating pattern until completing all three trials for both electrode styles. This setup was utilized to allow for calculations of (1) repeatability of a single electrode type to be investigated (i.e., consistency of L-Dex ratios between consecutive measurements), (2) reproducibility of a single electrode type to be investigated (i.e., consistency of the same electrode type between nonconsecutive measures), (3) comparison between electrode types to be determined, and (4) comparison between electrodes used for the first trial versus reuse during subsequent second and third trial measurements.
More specifically in terms of electrode placement, the dual-tab electrodes were positioned on the hands and right foot as directed by L-Dex U400 guidelines with the green line to align with identified bony landmarks (e.g., ulnar and radial styloid processes for wrist and medial and lateral malleoli for the ankle). The single-tab electrodes were positioned to replicate the placement of the dual-tab electrode by creating a template (Fig. 1) using the dual-tab electrode as a guide and adding the words “body” and “fingers/toes” to provide an orientation cue when aligning the green line to the body landmarks. Figure 2 illustrates correct and incorrect placement of the dual-tab electrodes and how the paper template offset to one side allows for the single-tab electrodes to be positioned midline on the body. Figure 3 shows the single-tab electrodes using the electrode template positioned, so the L-Dex electrode lead connectors are at an identical distance from each other as they are when using a dual-tab electrode to optimize standardization in BIS measurements regardless of the style electrode used.

Electrode template.
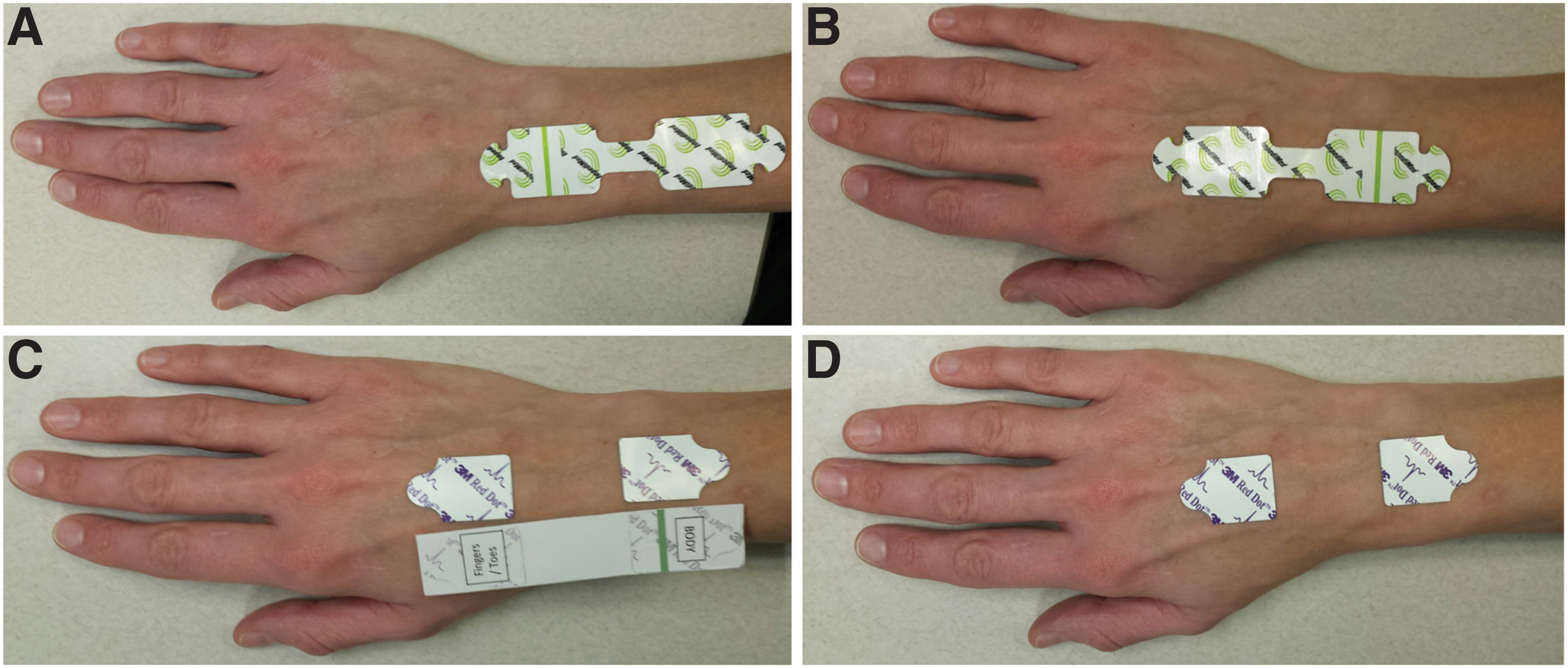
Positioning dual- and single-tab electrodes.
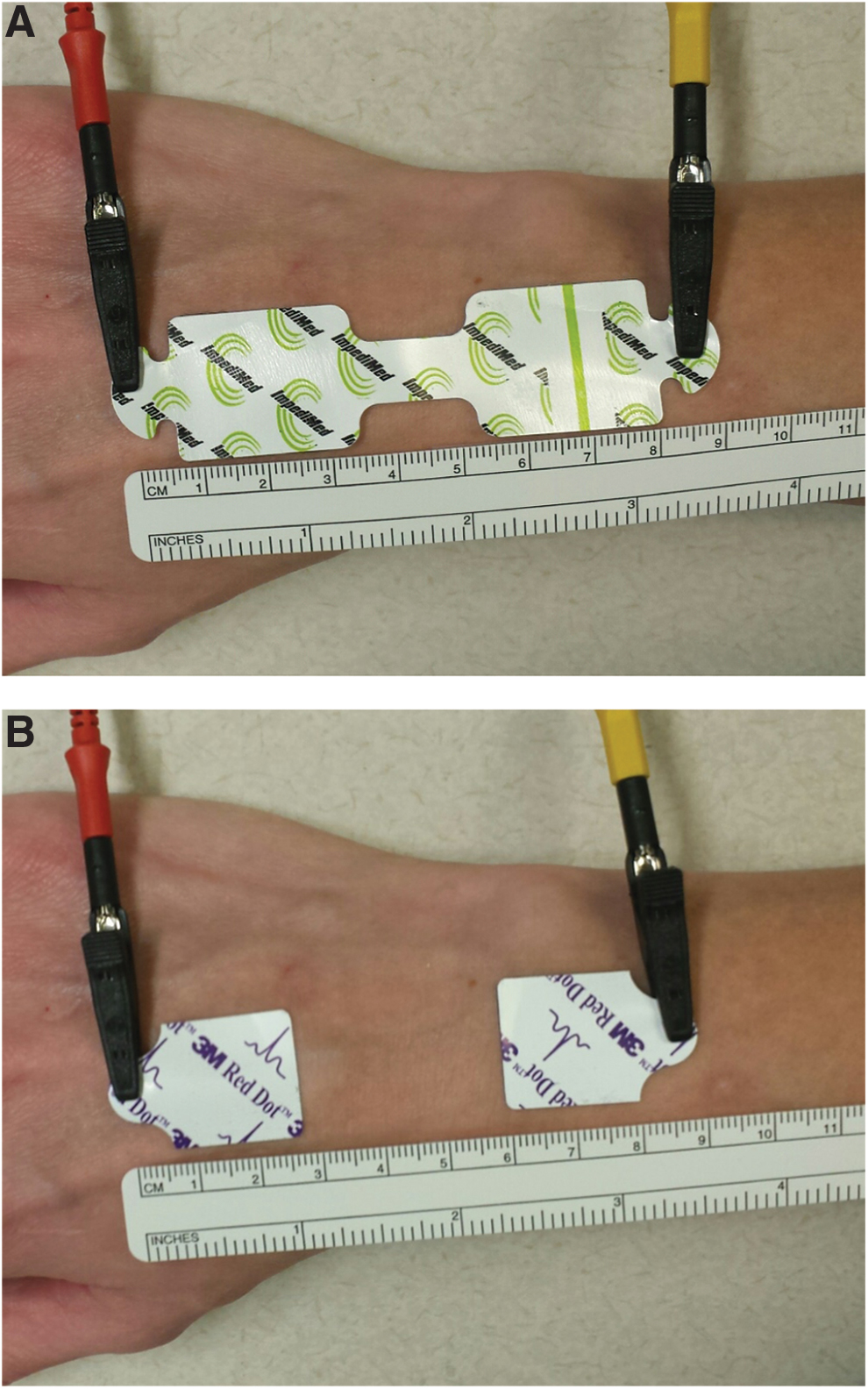
Distance of L-Dex® leads using dual- and single-tab electrodes.
Patients with BCRL versus age-matched controls
We acquired upper limb BIS measurements from patients with known BCRL (n = 17; Stage = 1–2; number nodes removed = 16 ± 8; age = 50.9 ± 10.6 years; age range = 33–77 years; body mass index [BMI] = 28.5 ± 4.9) and age-matched controls (n = 19; age = 48.2 ± 11.3 years; age range = 38–73 years; BMI = 25.9 ± 6.0). For this experiment, all volunteers were matched for biological sex (i.e., female), and we obtained a single L-Dex ratio using single-tab electrodes using the aforementioned electrode placement guidelines.
Statistical considerations
To evaluate the primary objective of whether single-tab and dual-tab electrodes provide similar information, two electrode types (dual-tab ImpediMed and single-tab 3M) were considered. For each electrode, we performed measurements as described above and presented all values and also summarized these 39 values by averaging the three measurements in each trial for each subject (13 subjects with three trials each). The intraclass correlation coefficient (ICC) for agreement was calculated using the 39 pairs of measurements. The mean of nine measurements (i.e., three trials with three measurements each trial) for each participant for each electrode type were presented graphically as a scatter plot and the Pearson's correlation (r) and associated two-sided p-value calculated. In addition, a linear mixed-effects model was applied to the raw measurements to determine if there were any differences between trials (e.g., first, second, or third) for each electrode type and between the electrode types for each trial. To test the secondary objective of whether the BIS measured from the single-tab electrode could discriminate between healthy and BCRL subjects, univariate analysis using a Wilcoxon rank-sum test was applied, as well as a linear regression with age as a covariate. In all tests, a two-sided p-value less than 0.05 was considered for statistical significance. Statistical analysis was performed by a statistician (L.D.) using the R statistical software (version 3.2.2; 2015-08-14) including packages: “ggplot2”, “irr” and “nlme.”
Results
Single-tab versus dual-tab electrodes
Individual L-Dex ratio measurements for each healthy control using single-tab and dual-tab electrodes are displayed together with a schematic of the experimental approach in Figure 4A and B. For both electrode styles, 39 summarized values (13 subjects with 3 mean trial values each) were used to calculate the ICC. The calculated ICC was 0.966 with 95% confidence interval (CI) = 0.937–0.982, indicating a high agreement between the two styles of electrodes when obtaining the L-Dex ratios.
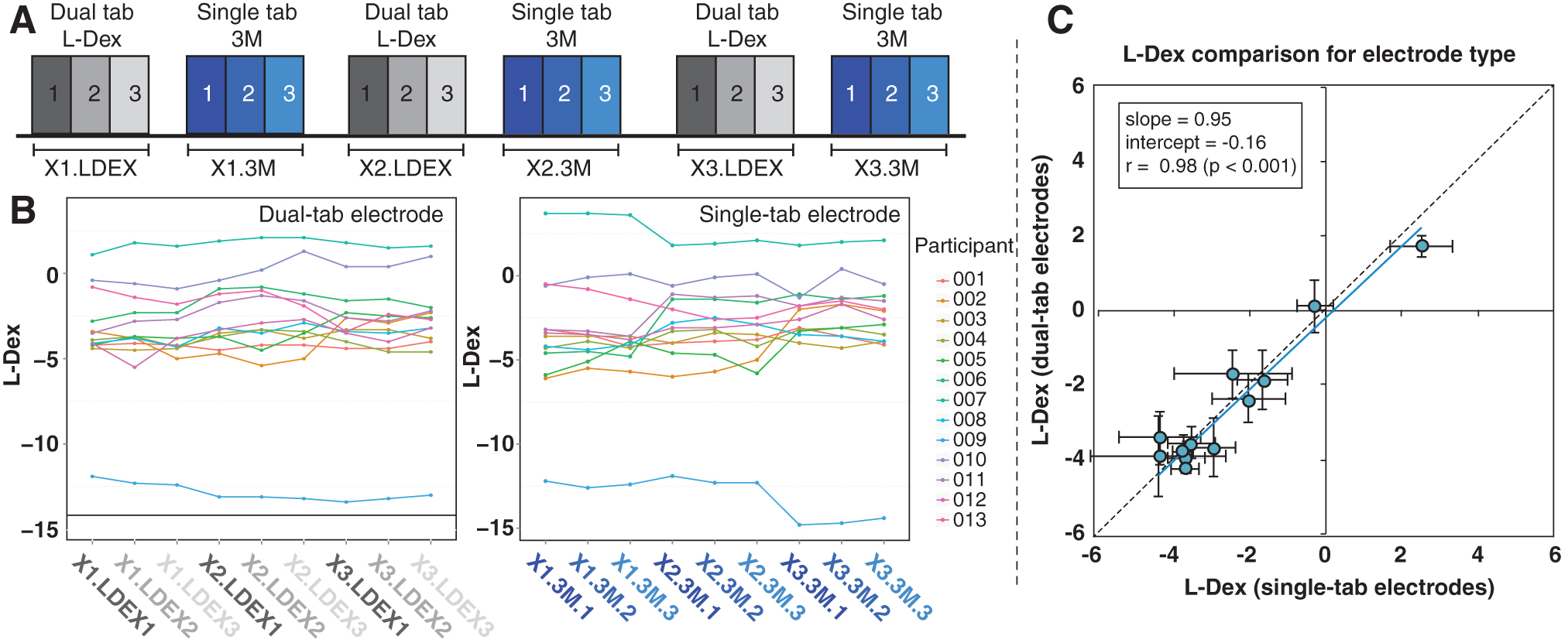
Single-tab versus dual-tab electrodes.
The linear mixed-effects model results using all the individual measurements demonstrated no evidence of significant difference between the single-tab and dual-tab electrodes when acquiring the L-Dex ratios. For the first trial (i.e., the first use of the electrode), the mean difference between the BIS measurements using the different electrode styles was estimated to be 0.04 with 95% CI = −0.22 to 0.30 (p = 0.74). There was little evidence of difference between the two electrode types for the second and third trials either (p = 0.51 and 0.31, respectively). A plot of the dual-tab versus single-tab L-Dex ratios is shown in Figure 4C, which yielded a Pearson's r = 0.98 and associated two-sided p < 0.001. One volunteer met outlier criteria and is not included in this plot, however, the inclusion of this outlier did not affect the significance of the correlation (remained p < 0.001).
When evaluating the effect of subsequent trials on L-Dex ratios, which involved reusing the same single- and dual-tab electrodes for repeated measurements on a single subject, a change in the ratio from the initial trial was observed, consistent with the conclusion that both style electrodes should only be used once as recommended by the manufacturer. For single-tab electrodes, the mean of the second trial was higher than the first trial, although not statistically significant (difference = 0.37, p = 0.26) and the mean of the third trial was also higher than the first trial (difference = 0.63, p = 0.06). A similar trend was also noted with the dual-tab electrodes. The agreement shown in the high ICC and the results from the linear mixed-effects model are consistent with the single-tab electrodes providing interchangeable measurements as the dual-tab electrodes.
Patients with BCRL versus age-matched controls
We next measured the L-Dex ratio using the single-tab electrode (one single measurement for each subject) in patients with BCRL (n = 17) and age- and sex-matched controls (n = 19). There was a significant difference in the BIS measurement between the patients (median = 12.30) and controls (median = 1.00) with p < 0.001 (Wilcoxon rank-sum test). Using linear regression adjusting for age, the mean L-Dex ratio was estimated to be 17.79 higher in the patients than in the controls. This difference is statistically significant with 95% CI = 9.69–25.90 (p < 0.0001). Figure 5A displays the age of patients and controls, and Figure 5B shows the L-Dex ratios for both groups. Table 1 summarizes the descriptive statistics by group. Significant discrimination between patients with known BCRL compared to age-matched healthy control volunteers was observed in the measured BIS ratios using single-tab electrodes, which corroborates the findings of studies showing the capability of BIS readings discerning lymphedema in patients with unilateral BCRL compared with healthy controls. 14 These findings are consistent with single-tab electrodes being discriminatory for BCRL when placed using the outlined manner.

Descriptive statistics by group.
Descriptive Statistics of Participant Ages and Bioimpedance Values (L-Dex Ratios)
Discussion
Our primary objective was to evaluate the consistency of the upper limb BIS measurement obtained using single-tab electrodes compared with dual-tab electrodes and to determine if there is any difference in the L-Dex ratio when using either style electrode. Our findings reveal consistency in BIS measurements using either of the electrode styles when the single-tab electrode placement is consistent with that of the dual-tab electrodes. We also found no significant L-Dex ratio difference when using single- versus dual-tab electrodes. These findings are relevant in that not only do they provide an alternative cost-effective option for obtaining consistent BIS measurements using a standardized electrode placement method but also permit interclinical communication of L-Dex ratios for long-term monitoring of BCRL in patients regardless of the electrode style used so long as the single-tab electrodes are positioned similar to the dual-tab electrodes. In this study, we created a simple electrode template replicating the dual-tab electrode that made accurate positioning of the single-tab electrodes controlled and efficient.
Our secondary objective was to evaluate if BIS measurements using single-tab electrodes could distinguish between lymphatic limbs versus healthy controls as already determined with use of dual-tab electrodes. This finding was supported as well. As researchers continue to investigate the potential of BIS in secondary lymphedema surveillance and its quantitative sensitivity for evaluating therapeutic responses, these findings motivate the use of single-tab electrodes to obtain L-Dex ratios, while maintaining an important standardized method to acquire these measurements. By investigating the option of using more readily available and cost-effective single-tab electrodes in place of dual-tab electrodes, this potentially expands the opportunity for more clinics and research settings to utilize BIS measurements on an ongoing basis to monitor for lymphedema progression, especially in a health care setting that is being reimbursed more strictly.
Cost considerations
Single-tab electrodes are readily available in hospitals and most outpatient clinics for use in common medical tests, such as EKGs and are less expensive than dual-tab electrodes, with a potential cost savings of 55-fold at current prices. Although some clinicians may be able to receive reimbursement for the test and would benefit from the convenience of a dual-tab electrode with no additional positioning of a template, the cost difference is substantial and these findings for the first time highlight the reproducibility and interchangeable use between the two electrode styles.
A dual-tab template as we described is necessary to help with correct and consistent placement of the single-tab electrodes. For this reason, dual-tab electrodes are the easiest to position since no template is needed for placement. However, a template is simple to produce and can be copied as a paper version for one-time use on patients. We found positioning single-tab electrodes as efficient as dual-tabs where the template also provided an additional orientation cue to ensure correct electrode placement by indicating “toes and fingers” or “body” locations. If attention is only on positioning the green line between malleoli or wrist condyles and attention was not also placed on the correct orientation of the dual-tab electrode in relationship to the green line as instructed by the manufacturer, then the electrode would be improperly positioned on the body and potentially provide a different L-Dex ratio. Since it matters where the electrodes are placed on the limbs 11 even if the distance between the electrode leads is the same, consistency in placement is most essential. The dual-tab electrodes, when positioned properly, allow for a level of standardization of electrode placement only needing to use one body landmark to position essentially two electrodes. The findings of this study reveal that single-tab electrodes are highly consistent and interchangeable with dual-tab electrodes, assuming that the placement on the body replicates that of the dual-tab electrode.
Limitations
The findings of this study should also be considered in light of several potential limitations. First, we evaluated only a single type of single-tab and dual-tab electrode. The high degree of correlation between these measurements and the similarity in electrode composition between manufacturers suggests that these findings are likely generalizable to other single-tab electrode variants; however, the data presented here cannot support that assertion unequivocally. However, as 3M single-tab electrodes are widely available and inexpensive, the results of this study should have relevance to most clinics seeking to interchange dual-tab and single-tab electrodes. Second, as with all clinical studies, there was some heterogeneity in the patient population in terms of BCRL stage and number of lymph nodes removed. We did not find any trend for the electrode type being preferentially useful for any one BCRL stage; however, larger studies with a wider range of patients are necessary to investigate this possibility.
Concluding remarks
The purpose of this study was to evaluate use of single-tab electrodes for BIS measurements and to assess whether single-tab electrodes, when positioned similarly to dual-tab electrodes, provided reproducible and consistent BIS measurements as well as offer discriminatory information in age-matched controls and patients with BCRL. We observed no significant differences between these two electrode types and high discriminatory capacity of single-tab electrodes for distinguishing BCRL versus control volunteers. These results suggest that single-tab electrodes may be a cost effective and widely available alternative to dual-tab electrodes in both clinical and research studies of patients with lymphedema.
Footnotes
Acknowledgments
The authors thank the National Institute of Nursing Research (NINR) within the National Institute of Health (1R01NR015079) and the Lipedema Foundation Award 12 for funding our research which resulted in this article. We are grateful to our subjects for their time and support. We also thank our clinical coordinator Allison O. Scott for assistance with subject recruitment.
Author Disclosure Statement
P.M.C.D. is a consultant for PureTech Health. M.J.D. receives research related support from Philips North America and is the CEO of Biosight, LLC which provides health care technology consulting services. No competing financial interests exist with the other authors.
Funding Information
NIH/NINR: 1R01NR015079 and Lipedema Foundation Award 12.