
Abstract
Background:
Objective assessment of upper limb physiological features may allow for early detection and proper intervention for lymphedema after breast surgery. However, the development of diagnostic instruments and standard measurement procedures are required.
Methods and Results:
Four instruments (Venustron, Softmeasure, Myoton Pro, and iBDent), tape measurement, and water volumetry were investigated in this study. Inter-limb differences in physiological data were obtained from 40 patients with lymphedema after breast surgery and 38 control subjects. Four instruments and tape measurements were performed at four points. Inter-limb differences between patients with lymphedema and control subjects were determined. All measurements took <20 minutes with minimal pain reported. Inter-limb differences in water volumetry and tape measurements, especially when measured at 5 cm distal to the cubital fossa, were increased in International Society of Lymphology (ISL) stage II cases. All four instruments showed high reproducibility in standard silicon sample measurement. On the other hand, data from human samples were varied, and the utility for assessment of lymphedema was not determined.
Conclusion:
Water volumetry and tape measurement at 5 cm distal to the cubital fossa were useful to assess lymphedema in ISL stage II cases. Four instruments used in this study were feasible in clinical practice. In addition, inconsistent data from human tissue were not due to sensor limitations, rather, acquisition of accurate data from human tissue seemed to be difficult due to anatomical factors. In addition to high-quality sensor, development of system that produce accurate and reproducible results from human tissue is required.
Introduction
Lymphedema is caused by the lymphatic system insufficiency and deranged lymph transport. Both primary (congenital) and secondary lymphedema are characterized by the leakage of plasma proteins into the interstitium, which induces swelling, pain, and various limitations to physical and psychosocial activities.1,2 Upper limb secondary lymphedema is a common side effect after breast surgery with a frequency of 6%–30%. 3 This type of lymphedema develops from a latent to a clinically apparent stage, peaking between 12 and 30 months after surgery. 4 Physical features may progress from reversible to irreversible according to the disease stage. Therefore, adequate prospective surveillance and assessment after surgery can be available not only for disease prevention, but also for the early detection of patients who need an intervention. 5 Various assessment methods and instruments have been reported to assess lymphedema. Bioimpedance spectroscopy was reported to be useful to detect extracellular fluid in stage I, and tape measurement and water volumetry were reported to be useful to assess volume change in stage II of the International Society of Lymphology (ISL) stage.1,6 High-quality, low-cost, and easy-to-use instruments may allow for a detailed and frequent prospective assessment, which may improve prevention, and early detection of patients in the latency period or reversible stage. An adequate intervention for patients in the latency period or reversible stage may prevent permanent disability and reduce direct cost of care. In this study, we determined the upper limb physiological features in patients with lymphedema after breast surgery. In addition, heterogeneous physiological features within the arm require standard assessment procedures to be used for the assessment of lymphedema in clinical practice. In the case of tape measurement, the bilateral assessment of multiple locations before and after swelling has been reported, but a standard assessment method has not been established. Therefore, we performed bilateral upper limb measurements on four points and compared the values with those of nonlymphedema subjects to establish a practical measurement protocol.
Materials and Methods
Bilateral upper limb measurements were performed using four instruments, water volumetry, and tape measurement, from April to December 2017. Forty patients with lymphedema after breast surgery participated in the study. In addition, 19 breast cancer patients without lymphedema before breast surgery and 19 healthy volunteers were also enrolled as control subjects. Lymphedema was staged according to the ISL stage, 1 and graded as stage 0 + I, early II, and late II. Four instruments were used for measuring physiological features: Venustron system (Axim, Kyoto, Japan), Softmeasure (Horiuchi Electronics, Tokyo, Japan), Prototype of iBDent (Koganei Corporation, Tokyo, Japan), and Myoton Pro (Myoton AS, Tallinn, Estonia) (Fig. 1). Physiological measurements using these instruments were performed at the inner base of the thumb, inner part of the wrist, and at the inner 5 cm distal to and 10 cm proximal to the elbow (dots in Fig. 2a–d). Tape measurement was performed using a flexible, nonstretch tape. Circumference measurements were performed at corresponding locations to the instrument measurements: the plane of the thumb and index finger and ulnar styloid process (corresponding to the inner base of thumb), ulnar and radial styloid processes (corresponding to the wrist), and 5 cm distal to and 10 cm proximal to the plane of the olecranon and cubital fossa (Fig. 2a–d). 7 Water volumetry was performed using a water bath, and the water volume overflowing from the water bath to the saucer was measured when the whole upper limb was inserted into the bath (Fig. 2e). These measurements were performed bilaterally and the inter-limb difference were determined.

Four instruments used in this study.
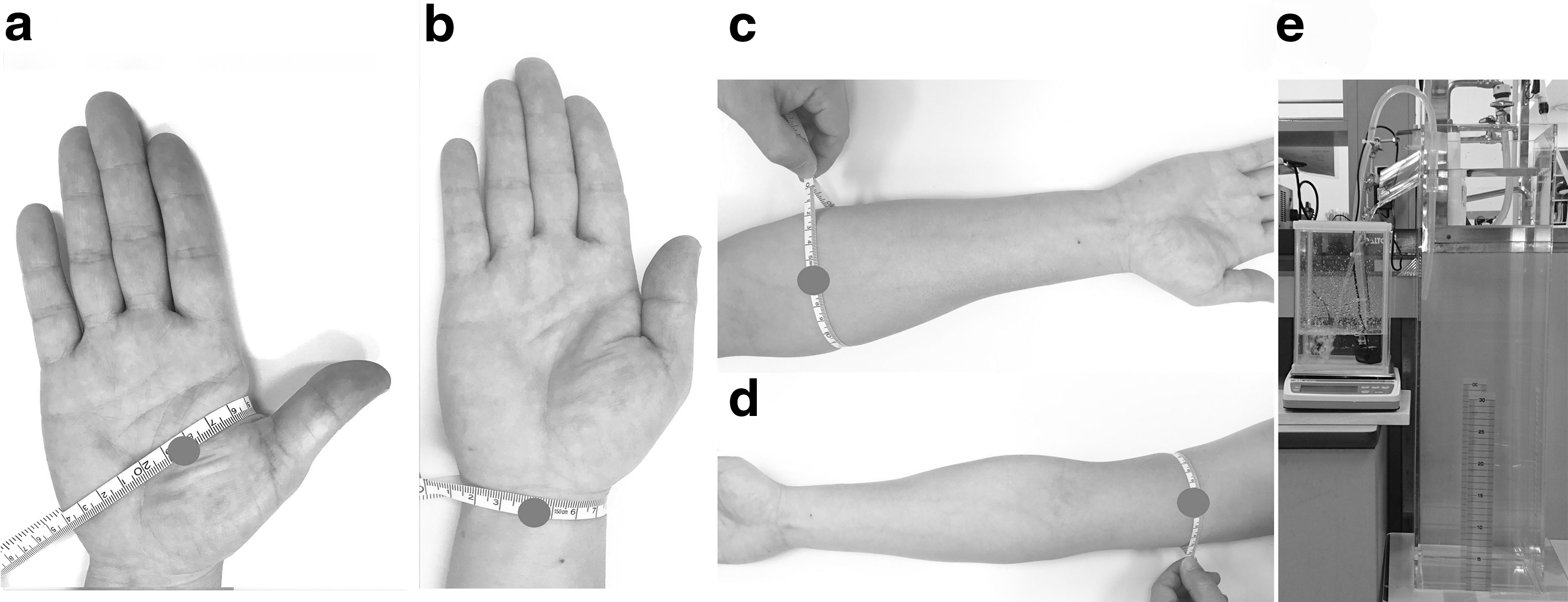
Instrument and tape measurements were performed at the locations shown by the dots and the tape, respectively
Inter-limb difference in physiological measurements were recorded as percentages and calculated as follows: Inter-limb difference in physiological measurements (%) = |(higher value, either in right or left)−(lower value, either in right or left)|/(lower value, either in right or left) × 100.
Inter-limb difference in physiological measurements was compared between patients with lymphedema patients and control subjects to elucidate the utility of these instruments in the assessment of lymphedema. Additionally, ISL stage-dependent changes in these data were also evaluated to elucidate their utility for lymphedema staging. We defined an outlier as any value larger than the third quartile by at least 1.5 times the interquartile range. The frequency of outliers was recorded for each measurement method.
Instruments used in this study and their feasibility in clinical practice
The Venustron system measures elastic modules based on Hooke's law and Hertz's contact stress theory.8–10 A ϕ5-mm piezoelectric tactile sensor was applied on the measurement point, and elasticity was calculated from the change of resonance frequency (Fig. 1a). Softmeasure is an indentation tester based on the Hertz's contact stress theory, and palpation mechanic; in this case, a ϕ10-mm rigid sphere indenter was applied on the measurement point (Fig. 1b). 11 The iBDent prototype is a tonometer system, which measures the phase difference caused by the deformation of the arm after compression by air (Fig. 1c). 12 Deformation of the arm after air compression at 30 kPa was recorded. Myoton Pro measures several biomechanical and viscoelastic features through the oscillation of measurement point (Fig. 1d). 13 In this study, dynamic stiffness, which characterize the resistance to an external force that deforms its initial shape, was chosen to evaluate the applicability of this instrument in the assessment of lymphedema. At first, the accuracy of these instruments was confirmed using four referenced silicon samples (S1–S4). S1 is the hardest sample, and the stiffness decreases progressively across the S2, S3, and S4 samples. Physiological data were obtained three times from each silicon sample using four instruments to confirm their reliability and reproducibility, and the relative ratio to the averaged physiological data compared with S1 sample was recorded in each measurement. Next, the time to assess physiological features in human tissue was measured, and pain caused by these assessments was also evaluated using the verbal rating scale to estimate the feasibility of use in clinical practice. 14
Informed consent
This study was approved by the National Cancer Center Institutional Review Board (2017-001) and all procedures were in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants, including healthy volunteers. The trial registration is UMIN 000028398.
Results
Clinicopathological features and feasibility of physiological data acquisition
Clinical data of patients with lymphedema after breast surgery and control subjects, including breast cancer patients without lymphedema before surgery and healthy volunteers, are shown in Table 1. All patients with lymphedema were women and 60.9 years old in average. The right and left sides were affected in 17 (42.5%) and 23 (57.5%) cases, respectively. ISL stage was 0 + I in 29 cases (72.5%), early II in 8 cases (20.0%), and late II in 3 cases (7.5%). All 19 breast cancer patients without lymphedema before surgery were female and had an average age of 61.0 years. Among the 19 healthy volunteers, 14 were female and 5 were male. Body height, weight, and body mass index were similar between groups. The assessment time ranged from 3.15 to 12.48 minutes across the four instruments used; most participants felt no pain during measurement (Table 2).
Patient Characteristics
BMI, body mass index; ISL, International Society of Lymphology; SD, standard deviation.
Time to Assess and Verbal Rating Scale Pain Score
The measurements made on silicon samples confirmed the high validity and reproducibility of these instruments (Fig. 3). All instruments produced reproducible results with low standard deviations. Venustron and Softmeasure successfully differentiated all referenced samples according to stiffness. Furthermore, data from these two instruments were in accordance. Myoton Pro successfully differentiated the S1, S2, and S3 samples according to stiffness, but failed to identify S4. iBDent successfully differentiated all samples according to stiffness, and less deformation was seen in stiffer samples. These results confirmed the quality of the sensors and that Myoton Pro may not be useful in the measurement of very soft materials.
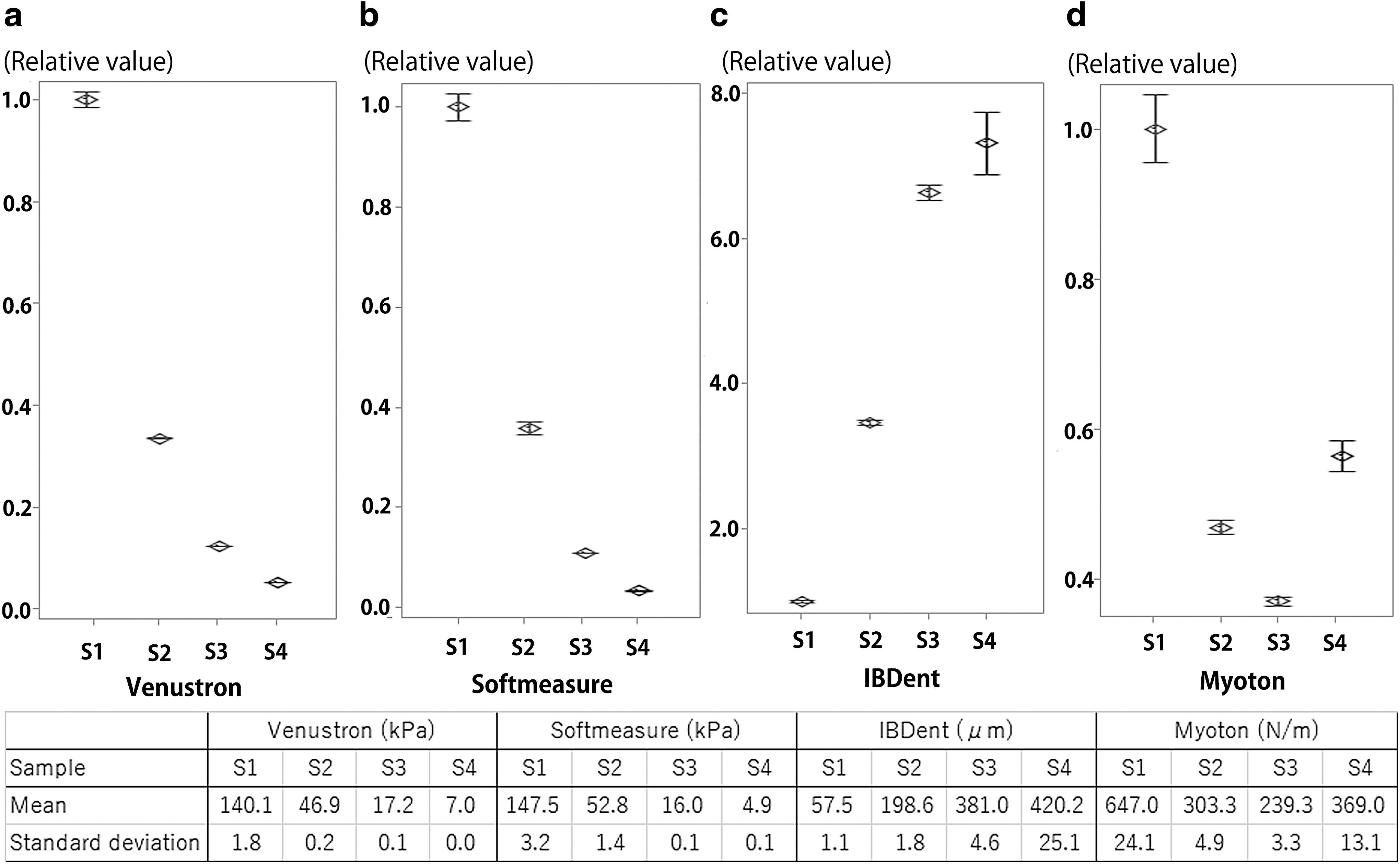
Silicon sample measurement using four instruments. Data accuracy of instruments was confirmed using four referenced silicon samples (S1–S4). S1 is the hardest sample, and the stiffness decreases progressively across the S2, S3, and S4 samples. Physiological data were obtained three times from each silicon sample using four instruments to confirm their reliability and reproducibility. In addition, relative ratio to the averaged physiological data compared with S1 sample was recorded in each measurement.
Physiological features of upper limbs with and without lymphedema
In water volumetry, inter-limb difference was similar among healthy volunteers, breast cancer patients without lymphedema before breast surgery, and patients with lymphedema (Fig. 4a). Additionally, cases of outliers were seen only in patients with lymphedema (Table 3). Although the inter-limb difference was similar between control subjects (healthy volunteers+patients with breast cancer before surgery) and stage 0 + I patients, this difference increased from early stage II to late stage II patients (Fig. 4b). Therefore, water volumetry can be used for the assessment of lymphedema after stage II but not in patients at stage 0 + I.

Water volumetry and tape measurement inter-limb differences.
The Frequency of Outlier Data
Inter-limb differences in tape measurements were plotted regardless of the location measured, and there was no difference among healthy volunteers, patients with breast cancer before surgery, and patients with lymphedema (Fig. 4c). There were also no differences between control subjects and stage 0 + I patients. However, the inter-limb difference increased from early stage II to late stage II patients (Fig. 4d). Separating data from each of the four locations revealed that the inter-limb difference at 5 cm distal to the elbow showed an increase in early and late ISL stage II patients (Fig. 5).

Inter-limb differences in tape measurement in the four locations. Measurements at 5 cm distal to the elbow showed an increase in patients in early and late stage II.
Water volumetry and tape measurement produced no outliers in control subjects, while the measurements in patients with lymphedema produced a few outliers. All four instruments produced outliers both in control subjects and in patients with lymphedema. Complete outlier information is shown in Table 3.
Compared with water volumetry and tape measurement, larger inter-limb differences were observed in the four instruments. Even in healthy volunteers, inter-limb differences of over 50% were observed in instrument measurements (Fig. 6); standard deviations were also larger. Venustron, Softmeasure, and Myoton Pro failed to show differences among patients with lymphedema, breast cancer patients without lymphedema before breast surgery, and healthy volunteers (Fig. 6a, b, d). When measuring patients with lymphedema, inter-limb differences did not correspond to ILS staging in any measurement point (Supplementary Figs. S1, S2, S3). Inter-limb differences measured by iBDent were not found among patients with lymphedema, breast cancer patients without lymphedema before breast surgery, and healthy volunteers (Fig. 6c). Increases in inter-limb difference according to ILS staging were found in the wrist and inner base of the thumb (Supplementary Fig. S4). However, large standard deviations were found for this measurement.
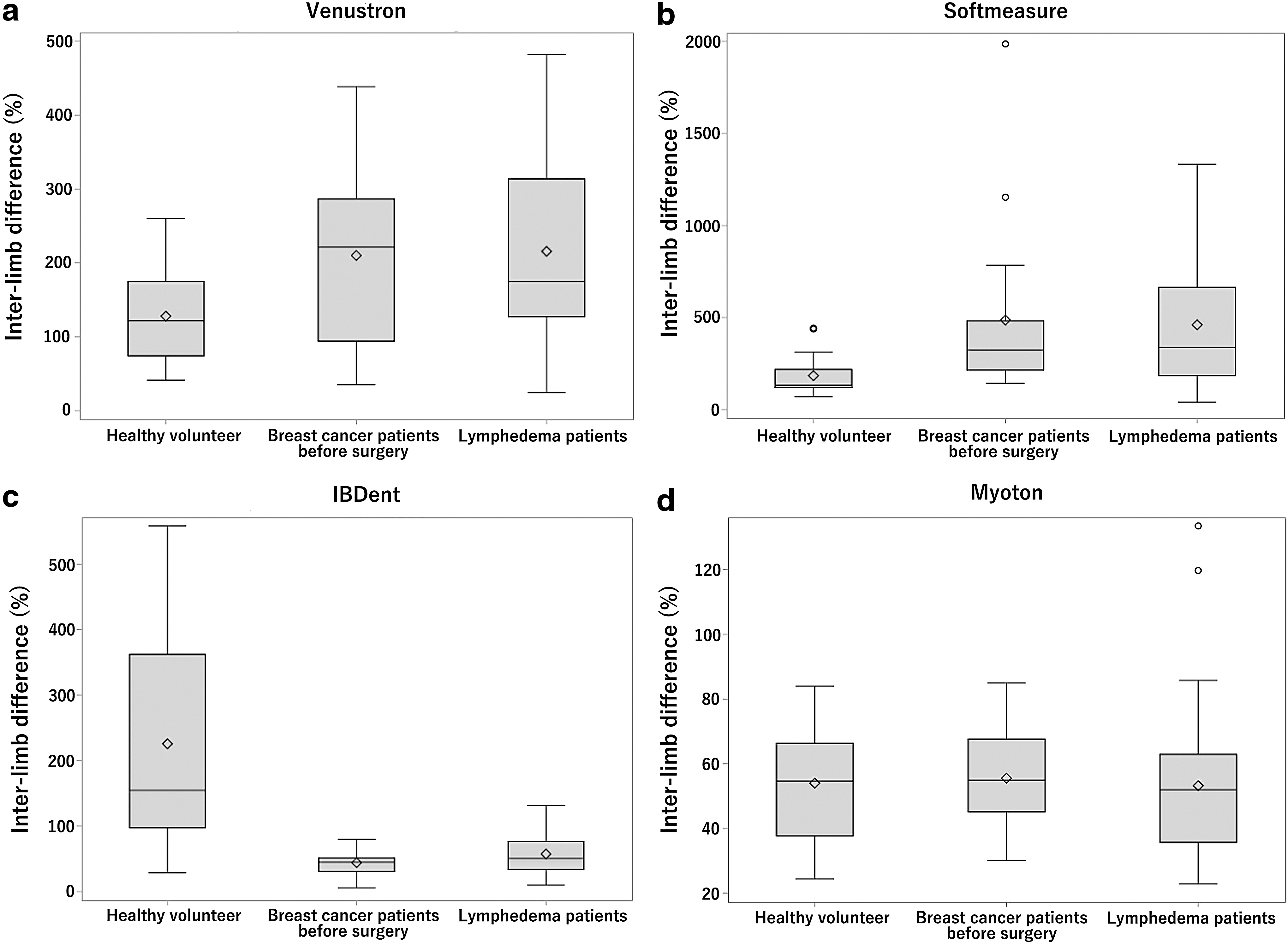
Inter-limb differences in instrument measurements. Data from the four locations measured were included in this figure. All instruments failed to show differences among patients with lymphedema, patients with breast cancer before surgery, and healthy volunteers
Conclusion
In this study, we aimed to standardize the methods and location of secondary lymphedema assessment after breast surgery. Water volumetry and tape measurement have been reported as the standard tools for the assessment of lymphedema, and water volumetry may be a reference test for measuring lymphedema in the upper extremities. In this study, we confirmed their utility, especially in patients classified as ISL stage II. 6 Tape measurement data showed significant variability across the different locations. These results suggested the need for standardization of the location of tape measurements. ISL consensus document 2016 described the utility of water volumetry and tape measurement. Tape measurement is simple and low cost with wide availability. On the other hand, there was little study about the measuring point available for accurate assessment of lymphedema. Our results suggest that 5 cm distal to the elbow is an appropriate location to detect patients with an ISL early and late stage II, which can be used for more simple and accurate data for the assessment of lymphedema. Our study revealed the importance of measuring point in tape measurement. On the other hand, this measurement variation across different locations can be influenced by clinical characteristics, such as body mass index, presence of taxane chemotherapy, and age. Therefore, further studies are required to establish the optimal location for the tape measurement. Water volumetry and tape measurement were found to produce reliable data without outliers in healthy subjects and reliability was confirmed as reported previously. On the other hand, these methods lack the ability to differentiate patients in ISL stage I; therefore, other modalities are required to detect early stage lymphedema.
The new instruments investigated in this study might offer another option to detect lymphedema at an early stage. However, we faced some limitations while conducting this study. The instruments showed frequent outliers, even in healthy subjects. Furthermore, large standard deviations were also seen. Therefore, we failed to find clinical utility for these instruments in this study. The measured physiological data were not associated with tape measurement findings at the same locations. We do not think that the technical limitations of these sensors were the cause of these results, since reproducible and accurate data were obtained from silicon samples. Some of the four instruments investigated in this study have also been reported to be useful for the assessment of lymphedema or other conditions, and data acquisition training may improve accuracy.9–13,15,16 However, instruments requiring extensive training will have a limited clinical application, and inconsistent interobserver findings will prevent the establishment of standardized measurement methods. Indeed, we felt some difficulty in measuring some participants, especially elderly subjects, since data acquisition requires that the subjects remain immobile. For adequate measurement, the sensors used in this study had to contact the skin vertically. This fact made data acquisition more difficult in participants who had difficulty in maintaining the same position. In addition, harder structures such as bone or tendon lie just underneath the skin tissue. Sensors may also assess such structures without the examiner being aware.
Taken together, the development of instruments, which can effectively assess lymphedema requires a way of confirming vertical position and the differentiation of harder tissue, as well as high-quality sensors. Our results of short assessment time and little pain revealed good feasibilities of these instruments in this study. In addition, these instruments are handy and low cost. We believe development of combination system with these sensors, vertical position sensor, and hard tissue differentiate sensor, enable more concordant assessment of lymphedema. Such a system may allow for more frequent assessment using handy instruments, and can elucidate unknown information such as daily fluctuation of lymphedema. With increasing survival, improved quality of life is increasingly important for patients with breast cancer. 17 Various kinds of sensors that measure physical properties can contribute to improve the quality of life of patients with breast cancer through the assessment of lymphedema. Systems that ensure accurate data collection from human tissue are required to address the heterogeneous physiology.
We confirmed the usefulness of water volumetry and tape measurement to differentiate patients in ISL stage II. Furthermore, tape measurement showed a high variation across the different measurement locations in patients with lymphedema. The plane 5 cm distal to the cubital fossa can be used as a standard location for tape measurement. In addition to the development of high-quality sensors, systems that ensure accurate human tissue measurement are required for the assessment of patients with lymphedema.
Footnotes
Acknowledgments
This work was supported by Murata Corporation (Kyoto, Japan). A.N. and K.Y. were full-time employees of Murata Corporation.
Disclaimer
There are no constraints from the sponsors on results or conclusions in this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.