
Abstract
Background:
Lymphedema includes primary lymphedema (P-LE) and secondary lymphedema (S-LE), which is a chronic progressive disease. The former group is further classified as congenital and acquired P-LE (AP-LE); its etiology is unclear, and only a few studies on its pathophysiology exist. We hypothesized that an autoimmune disease or self-inflammatory mechanism occurs in lymphatic vessels, leading to obstruction.
Methods and Results:
We enrolled 46 patients with lymphedema who underwent lymphaticovenous anastomosis (LVA) from January to October 2015. Collecting lymph ducts were obtained during LVA. We performed hematoxylin/eosin staining and immunostaining for LYVE-1, IL-1β, IL-6, and TNF-α. There were no substantial histological differences between the two types of lymphedema, whereas some differences in expression of inflammatory cytokines, including interleukin (IL)-1β and tumor necrosis factor (TNF)-α, were observed. Only a few inflammatory cells could be seen around the vessels. Although no significant differences in expression of IL-1β were found between AP-LE and S-LE, TNF-α was more highly expressed in the smooth muscle layer in AP-LE patients than in S-LE patients. There were no significant morphological differences in the collecting ducts of lymphatic vessels between S-LE and P-LE. Nevertheless, higher levels of TNF-α accumulation were found in the thick smooth muscle layer of P-LE patients than in that of S-LE patients.
Conclusion:
TNF-α-related inflammation in collecting ducts of lymphatic vessels is an important characteristic of the pathology of P-LE. TNF-α inhibitors might improve symptoms of AP-LE.
Introduction
Lymphedema is a progressive disease characterized by the dysfunction of lymphatic vessels, as well as the accumulation of extracellular fluid, protein, and waste products from cells in the interstitial space. 1 In many cases, pain and cellulitis in the affected area occur frequently. In severe cases, the tissue hardens, and pitting is absent (stage 3, according to the International Society of Lymphedema). Lymphangiosarcoma occurs in few cases. 2 Lymphedema has a severe chronic impact on quality of life.
There are two types of lymphedema, primary lymphedema (P-LE) and secondary lymphedema (S-LE). S-LE occurs after lymphadenectomy for cancer, radiotherapy for malignancies, injury, and other injuries. P-LE includes congenital and acquired (AP-LE) types. 3 In some congenital P-LE, the responsible gene is known (VERFR-3: Milroy disease 4 ; FOXC2: lymphedema/distichiasis syndrome 5 ; SOX18; hypotrichosis/lymphedema/telangiectasia syndrome). 6 In contrast, the pathophysiology of AP-LE has not been elucidated.
Combined physiotherapy, consisting of lymph drainage, compression therapy, and skin care, is used to treat both types of lymphedema. As surgical treatments, lymphaticovenous anastomosis (LVA) and lymph node transplantation are performed. Nevertheless, there is no evidence-based treatment for AP-LE.
AP-LE often develops in individuals younger than 35. 3 Sometimes it occurs without induction, while in other cases it occurs as a result of inflammation such as cellulitis in the affected limb. There are many AP-LE patients with repeated episodes of inflammation in the affected limb.
We hypothesized that inflammation was involved in the etiology and pathology of AP-LE and that there is some inflammation of lymphatic vessels before lymphatic vessel disturbances. In our hospital, we perform LVA for AP-LE. During surgery, we took specimens of collecting lymphatic vessels and performed histological research.
Materials and Methods
Patients
Nineteen AP-LE patients and 27 S-LE patients as controls were examined. All underwent surgery (LVA) at Yokohama City University Hospital from January to October 2015. All of these operations were performed sequentially within this period. There were no selection criteria for patients for this study. Lymphoscintigraphy revealed edema of the limbs and lymphatic dysfunction in all patients. This study was approved by the ethics committee of our hospital (Research No. B100902029).
Collection of samples
From each patient, one or two samples of collecting lymphatic vessels were taken from the nonanastomosis side during surgery avoiding to disturbing the anastomosis. The specimens were fixed in 4% paraformaldehyde phosphate buffer and embedded in paraffin.
Pathological investigations
Hematoxylin/eosin (HE) staining and immunostaining were performed. This process was ordered from Kyoudou Byouri in Japan. As markers of lymphatic endothelial cells, LYVE-1 and podoplanin were selected: anti-human LYVE-1 mouse monoclonal antibody (MAB20892; R&D System, MN) and anti-human D2-40 mouse monoclonal antibody (SIG-3730; Covance, NJ) were purchased. Alpha-smooth muscle actin (α-SMA) was selected as a marker of the muscle layer of lymphatic vessels. For factors of inflammation and autoimmune disease, IL-1β, IL-6, C1q, C3, C4, IgG, TNF-α, and NF-κB were selected: anti-human IL-1β rabbit polyclonal antibody (sc-7884; Santa Cruz, TX), anti-human IL-6 rabbit polyclonal antibody (109-401-310; Rockland, Inc., PA), anti-human C1q complement rabbit polyclonal antibody (A136; DAKO, Glostrup, Denmark), anti-human C3c complement rabbit polyclonal antibody (F0201; DAKO), anti-human C4c complement rabbit polyclonal antibody (F0169; DAKO), anti-human IgG rabbit polyclonal antibody (F0202; DAKO), anti-human TNF-α rabbit polyclonal antibody (ab66579; Abcam, Cambridge, United Kingdom), anti-human smooth muscle actin mouse monoclonal antibody clone; 1A4 (M0851; DAKO), and anti-human NF-κB rabbit polyclonal antibody (sc-7178; Santa Cruz) were purchased from Kyowa Medical Corporation (Shizuoka City, Shizuoka, Japan).
Paraffin-embedded sections were deparaffinized and antigens were activated with 10 mM citric acid buffer solution at pH 6.0 (NF-κB, IL-1β, D2–40, LYVE-1), with 0.1% trypsin/phosphoric acid buffer solution at pH 7.6 (C1q, C3, C4, IgG). Antigen activation was not performed for α-SMA, interleukin (IL)-6, or tumor necrosis factor (TNF)-α. Subsequently, endogenous enzymes were removed with 3% H2O2/purified water and washed with 0.05 M phosphoric acid buffer solution at pH 7.6. Nonspecific proteins were absorbed with Blocking
Samples were observed with an optical microscope (Biorevo BZ9000; Keyence, Osaka, Japan) and analyzed using BZ-II Analyzer ver. 1.42 (Keyence). We compared the expression intensity of each factor in terms of obstruction of lymphatic vessels, the condition of lymphatic lumens and walls of lymphatic vessels, inflammatory reactions, and immune reactions in AP-LE and S-LE.
We calculated relative expression ratios of IL-β and TNF-α in lymphatic vessel specimens by taking measurements of the dyed area in the cross section of lymphatic vessels (relative lymphatic vessel expression ratio: dyed area/area of each lymphatic vessel) with BZ-II Analyzer ver. 1.42 (Keyence).
Results
Among the AP-LE patients, 18 were female. All S-LE patients were female. The average age of the AP-LE patients was 40.2 ± 4.1 years, while that of the S-LE group was 56.8 ± 2.0 years. Average onset age of AP-LE was 33.1 ± 4.0 years, while that of P-LE was 47.4 ± 2.1 years. Both average age and average onset age of AP-LE patients were significantly younger than those of the S-LE patients. All AP-LE patients were affected in the lower limbs only. Among the S-LE patients, two patients had upper limb involvement, 21 were affected in the lower limbs, and four were affected in both the lower abdomen and lower limbs. In the AP-LE group, there were eight patients with a history of inflammation in the affected part. There were 16 patients with history of inflammation in the S-LE group. The average body mass index was 21.2 ± 0.5 for AP-LE patients and 22.8 ± 0.7 for S-LE patients.
Other patient background information was as follows. The average pulse rate of AP-LE patients was 72 ± 4 bpm, while that of S-LE patients was 68 ± 2 bpm. No patients smoked in either group. Neither group included patients with diabetes mellitus. We found four patients with hyperlipidemia in the S-LE group, whereas there were no such patients in the AP-LE group. Four patients with hypertension were observed in the S-LE group, whereas there were no such patients in the AP-LE group. Only one patient with chronic heart disease was observed among the S-LE patients, while there were no such patients in the AP-LE (Table 1).
Patient Background and Statistical Analysis
AP-LE, acquired primary lymphedema; S-LE, secondary lymphedema.
Thickened smooth muscles of lymphatic vessels were observed in the specimens of both groups. Ectasia type, contraction type, and sclerosis type with thickened smooth muscle of collecting lymphatic vessels were recognized on HE staining and α-SMA immune staining. Thickness of smooth muscle layer and area of lumen were not significantly different between the AP-LE and S-LE groups (Figs. 1 and 2). Regarding expression of LYVE-1 and podoplanin as markers of lymphatic endothelium, no substantial differences were found between the groups (Fig. 3). These proteins were found positive or weakly positive in the ectasia type, and weakly positive or negative in the contraction and sclerosis types. Regarding inflammatory reactions and factors related to autoimmune disease, there were no significant differences of expression of IL-6, C3, and C4 in the lymphatic vessels between the groups (data not shown). In 6 of 19 patients with AP-LE and 8 of 27 patients with S-LE, deposition of IgG to lymphatic endothelium was observed. One patient with AP-LE showed deposition of C1q in the lymphatic endothelium in the same area as deposition of IgG (Fig. 4). In both groups, IL-1β and TNF-α were strongly expressed in the thickened smooth muscle layer (Fig. 5).
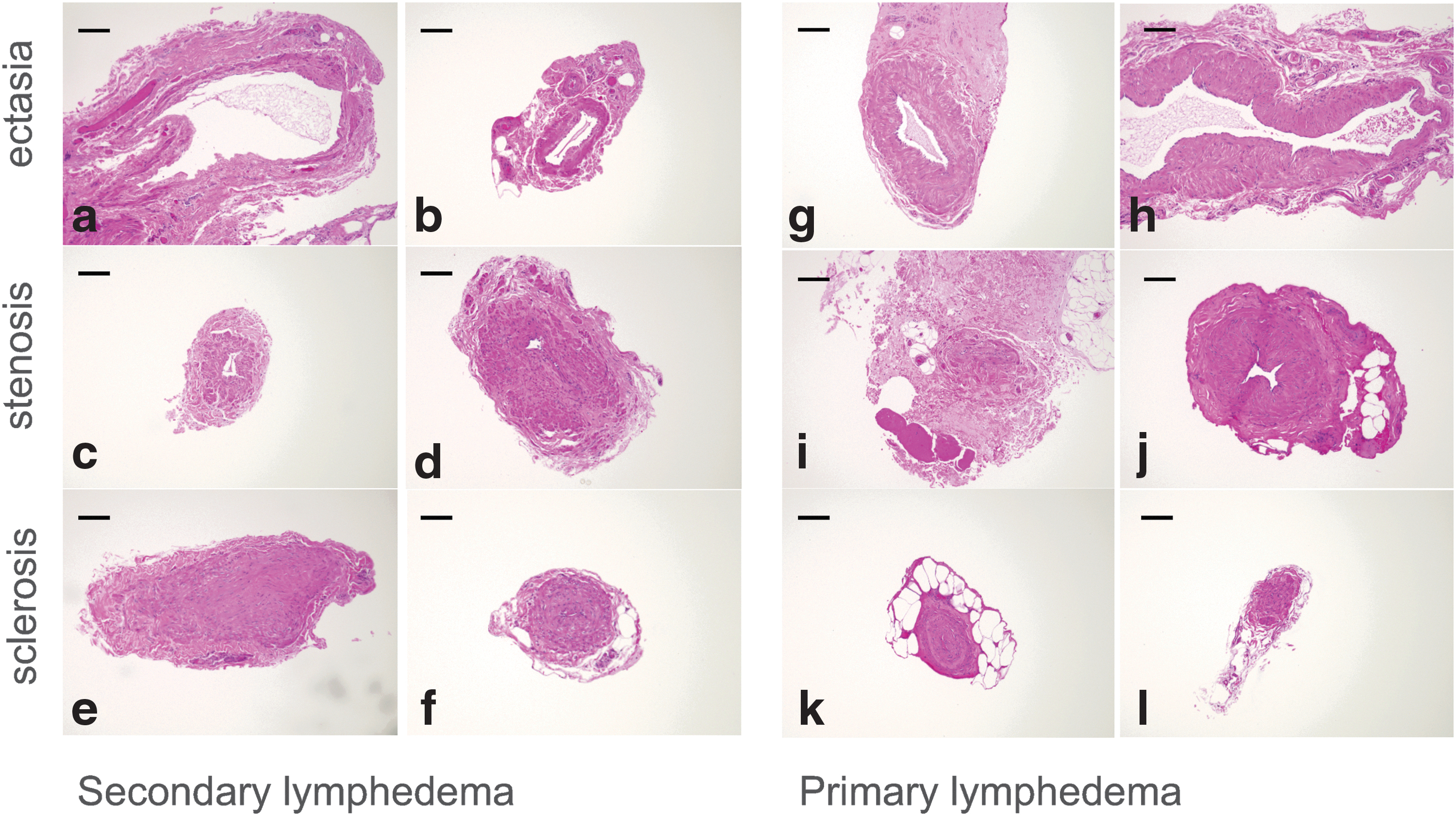
HE staining of lymph ducts from lymphedema patients. The upper row shows the ectasia type of lymph ducts. The middle row shows the stenotic change of collective lymphatics. The thickness of the muscle layer is over 100 μm. The lower row indicates the closed lumen of collective lymph ducts.
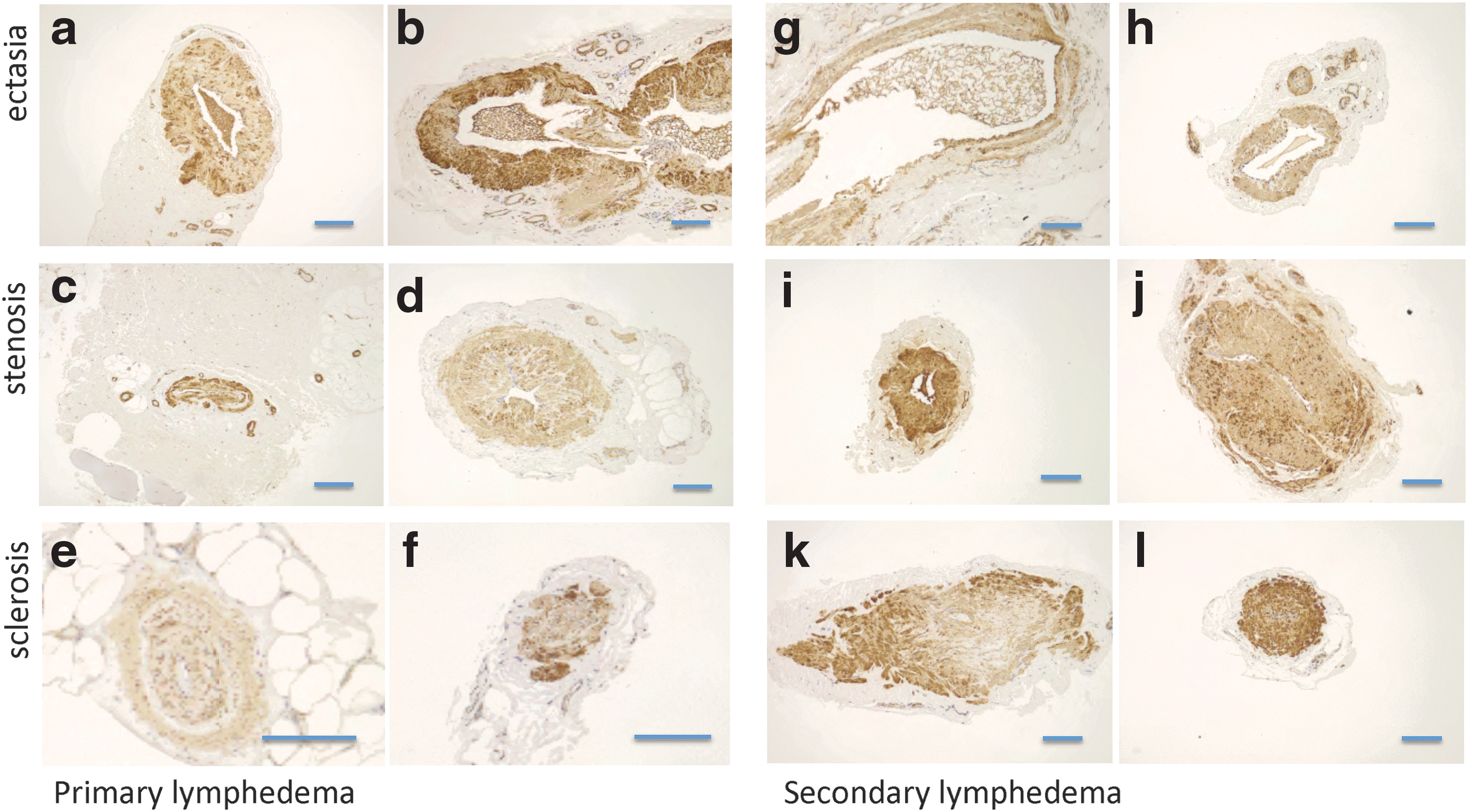
Immunohistochemical staining of α-SMA. The upper row shows ectasia type lymph ducts. Although the smooth muscle layer has been already thickened, the lumens of the lymph ducts were preserved or dilated. The middle row shows stenotic changes of lymphatics from both P-LE and S-LE patients. The ratio of smooth muscle layer in diameter is much higher than that of the lumen of the lymphatics. The lower row shows the closed lumens of collective lymph ducts. Almost all sections were occupied with smooth muscle. The smooth muscle layers of the lymphatic vessels were stained with horseradish peroxidase as a secondary antibody. From

Immunohistochemical staining of LYVE-1 and podoplanin. The first, second, and third rows show ectasia-, sclerosis-, stenosis-type lymphatic vessels, respectively. There was no substantial difference between the two groups regarding expression of LYVE-1 or podoplanin.
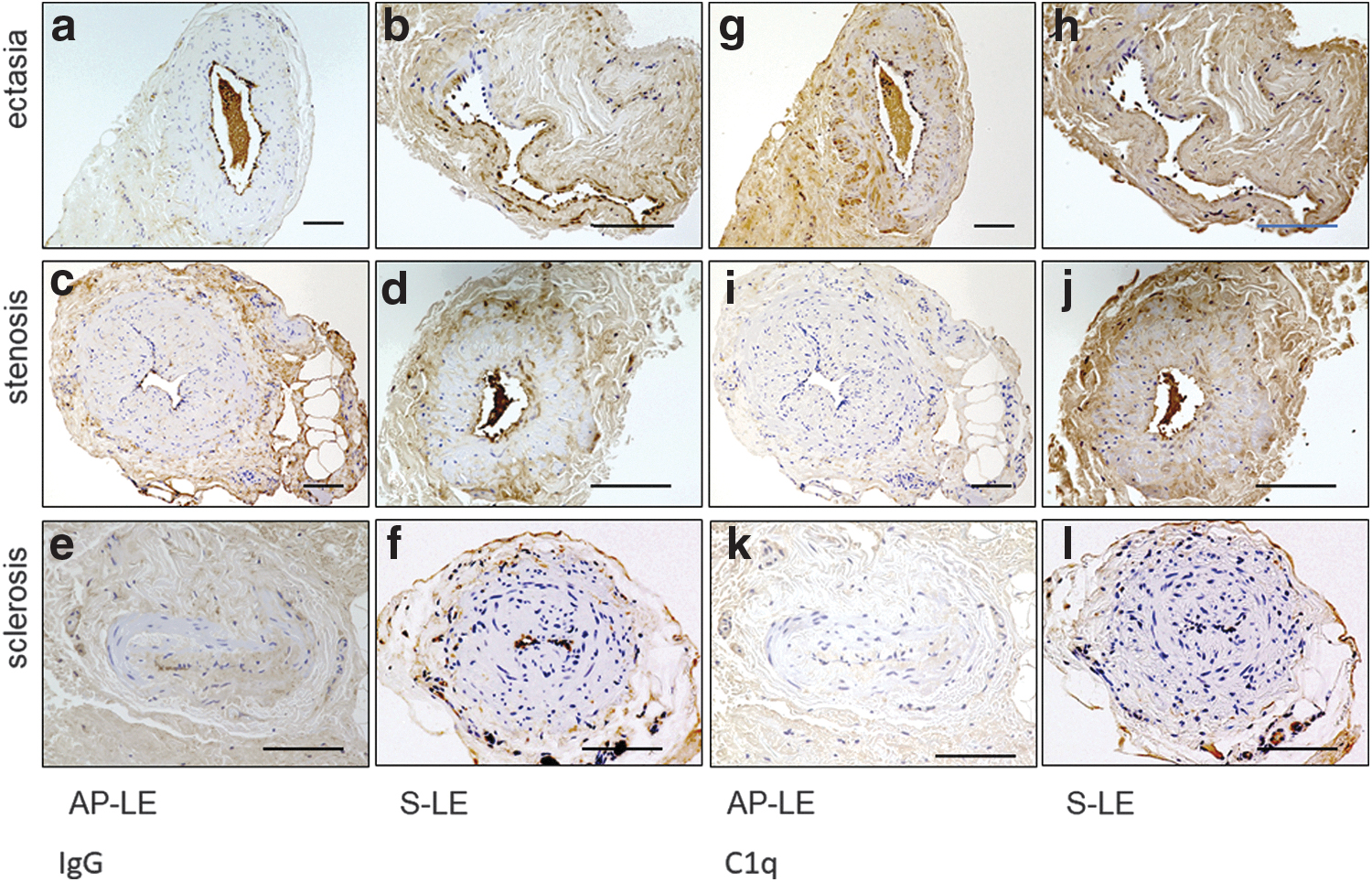
Immunohistochemical staining of IgG and C1q. The first, second, and third rows show ectasia-, sclerosis-, stenosis-type lymphatic vessels, respectively. There was no substantial difference between the two groups regarding expression of IgG and C1q.
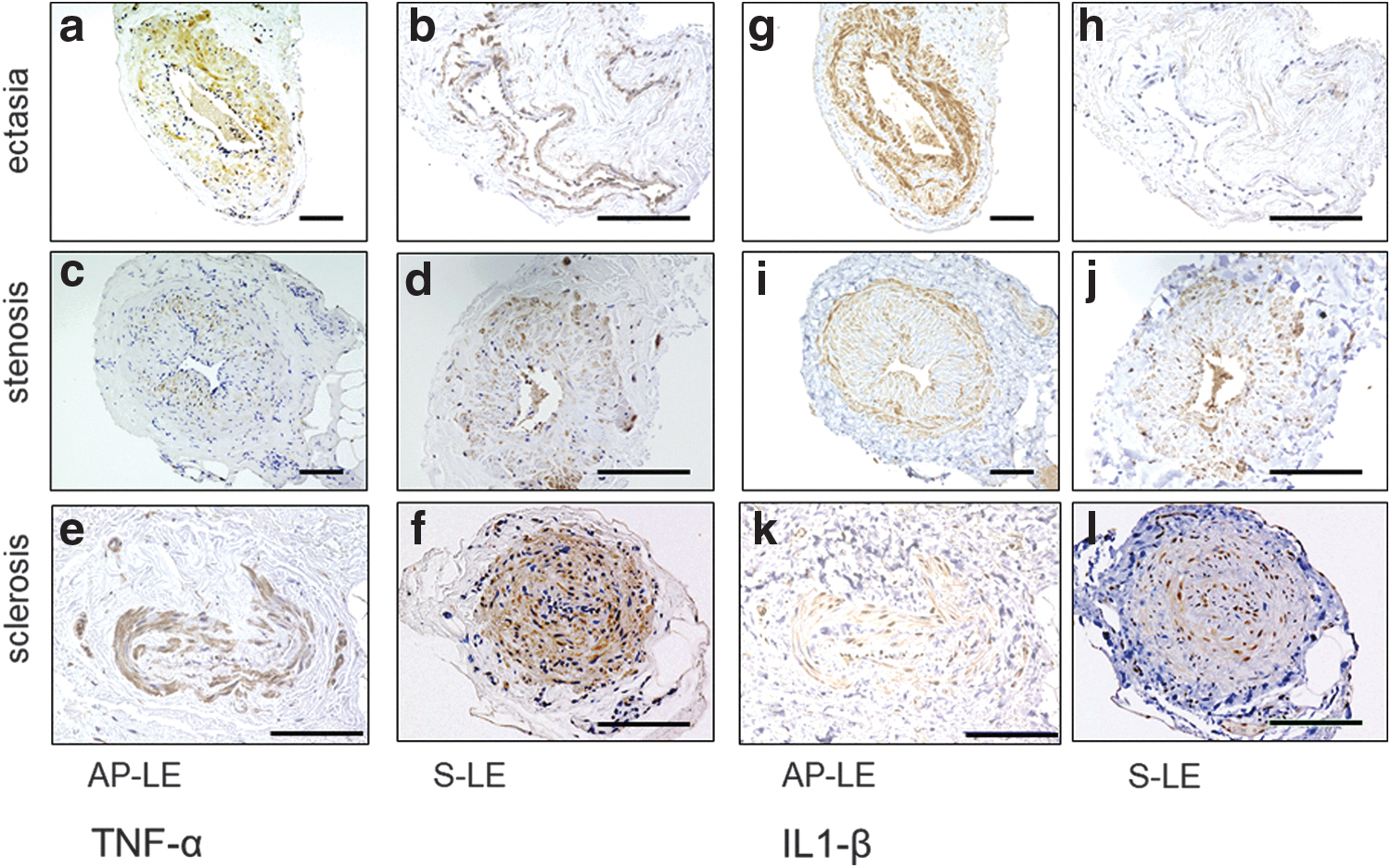
Immunohistochemical staining of TNF-α and IL-1β. TNF-α and IL-1β were highly expressed in the smooth muscle layers in the specimens of both AP-LE and S-LE patients. These cytokines were expressed in all stages of lymphedema.
As damage to lymph vessels progresses, the lumen of lymphatics changes as follows: normal to dilated, dilated to stenotic, and stenotic to occluded.7,8 The thickness of the lymphatics also changes from normal to thinner, thinner to thickened. In both groups, we excluded patients with contraction and sclerosis types who appeared to have end-stage lymphatic vessels. We made comparisons regarding expression of IL-1β and TNF-α in the patients with dilated lymphatics that seemed to be in the progression stage.
There were eight AP-LE patients and six S-LE patients with dilated lymphatics. Regarding patient background, there were no significant differences between the groups (Table 2). We compared IL-1β and TNF-α expression ratios in the lymphatic vessels. There was no significantly deference between the groups with respect to IL-1β (p = 0.061, Fig. 6). In contrast, TNF-α deposited more strongly in the AP-LE group than in the S-LE group (p = 0.0017, Fig. 6).

Relative expression ratio of TNF-α and IL-1β. Expression levels of TNF-α and IL-1β in specimens from AP-LE patients were higher than those of S-LE patients. The difference between AP-LE and S-LE was statistically significant for TNF-α expression, while the difference for IL-1β was not. Error bar: standard deviation.
Patient Background and Statistical Analysis, Whose Collecting Lymphatic Vessels Were Dilated
BMI, body mass index.
NF-κB was positive in lymphatic endothelial cells in seven patients with AP-LE and one patient with S-LE.
Discussion and Conclusions
We found that TNF-α in the smooth muscles of lymphatic vessels was expressed in higher amounts in AP-LE than in S-LE patients. There is a possibility that high expression of TNF-α is related to onset or progression of disease in some AP-LE patients. Because NF-κB was expressed in lymphatic endothelial cells, TNF-α may be produced in the smooth muscle cells of lymphatic vessels acting as lymphatic endothelial cells. This finding suggests that the TNF-α pathway is activated in AP-LE patients.
IL-1β and TNF-α, both inflammatory cytokines, were strongly expressed in the thickened smooth muscle layers, suggesting inflammation in local areas of collecting lymphatic vessels. Moreover, it appears that these cytokines were more strongly expressed in the ectasia type than in the contraction or sclerosis types. By contrast, there were few inflammatory cells surrounding lymphatic vessels in the specimens; therefore, we assumed that lymphatic smooth muscle cells produced these cytokines, and inflammatory cytokines were involved in the progression of lymphedema. However, there are few studies that have shown the secretion of TNF-α from smooth muscle cells. In addition, we could not collect TNF-α mRNA from specimens because of the small number of samples.
The systolic blood pressure of the S-LE was higher than that of the AP-LE group. The reason may be related to the higher average age of the S-LE group. However, we believe that the influence of systolic blood pressure to the difference between the two groups is not particularly significant.
Marker proteins of lymphatic endothelium were low in both groups. This may be caused by damage of lymphatic vessels. 7
Deposition of IgG and C1q in the lymphatic endothelium was observed in some patients in both S-LE and AP-LE groups. This may suggest some immune responses in the lymphatic endothelium, whether or not there is pathological significance.
In both groups, we found thickened smooth muscle of collecting lymphatic vessels. Ectasia, contraction, and sclerosis types with thickened smooth muscle of collecting lymphatic vessels were recognized. We believe that as lymphedema progressed, these pathological changes progressed.7,8 While lymphedema progresses, functions of lymphatic smooth muscle cells are important; when lymphedema worsens, lymphatic smooth muscles become thicker. 8
It was reported that combined therapy reduces gene expression of inflammatory cytokines. 9 However, there have been few reports regarding expression of inflammatory cytokines on the local side of lymphatic vessels or relationship between cytokines and lymphedema.
It was also reported that the expression of tumor necrosis factor receptor depends on lymphoproliferative disorders, 10 and a similar phenomenon may occur in AP-LE and S-LE. In this study, we could not determine whether high expression of TNF-α was the cause of lymphedema or not. Whether or not we examine the expression of mRNA for TNF-α in the smooth muscle layer, it would be difficult to answer to this question. Moreover, there is no appropriate animal model of AP-LE.
There are case reports of lymphedema associated with rheumatoid arthritis or lymphedema associated with psoriatic arthritis being treated successfully with TNF-α inhibitors.11–13 If we had administered TNF-α inhibitors to AP-LE patients, it could have improved symptoms of AP-LE, possibly clarifying the pathophysiology of AP-LE. Ulinastatin, which downregulates TNF-α, has been effectively administered to pulmonary fibrosis patients. 14 A similar effect may be expected in some lymphedema patients.
Footnotes
Acknowledgments
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by Grant-in-Aid for Science Research (C) (project no. 1717K11544).