
Abstract
Background:
Previous animal studies have shown that intragastric administration of water can accelerate mesenteric lymph flow. Similarly, human studies have shown that abdominal breathing can induce thoracic lymph drainage. In these studies, lymph flow was measured by hemodilution and a corresponding reduction in blood anti-diuretic hormone (ADH) levels, the latter being linked to urine osmolarity. Hence, we questioned if induction of lymph flow through water administration and supine positioning could be measured by monitoring urine osmolarity.
Methods and Results:
Volunteers were given 250 mL of distilled water and then made to rest for either 10 or 30 minutes in a supine position. Blood samples were taken pre and postrest to monitor changes in plasma ADH, total protein, plasma albumin, red blood cell, and hemoglobin concentrations. Urine was collected to monitor [Na+], [Cl−], and osmolarity. Intake of 250 mL distilled water with 10-minute rest caused a significant reduction in plasma ADH concentration, with decreases in urine [Na+], [Cl−], and osmolarity. We found a linear relationship between the ratio of plasma ADH concentrations after/before rest (between 1.1 and 3.0 pg·mL) and the ratio of urine osmolarity after/before rest (between 180 and 601 mOsm·L).
Conclusions:
Intake of 250 mL distilled water with 10-minute rest in a supine position caused hemodilution and a reduction in urine osmolarity consistent with thoracic lymph drainage. Urine osmolarity is a simple, safe clinical measure for monitoring lymph flow that could be used to evaluate the technique of lymph edema therapists.
Introduction
In a previous study, we described a simple and accurate method for evaluating lymph flow through the thoracic duct in human participants by measuring abdominal respiration-mediated hemodilution and its related reduction in anti-diuretic hormone (ADH) concentration in the blood. 1 The work followed on from animal studies by our group that used an in vivo Sonazoid-based, contrast-enhanced, ultrasound-guided method to show manual massage of the cisterna chyli in rabbits produces a significant increase of lymph flow through the thoracic duct, resulting in significant reductions in the blood concentration of total protein (TP), plasma albumin (Alb), red blood cells (RBCs), and hemoglobin (Hb). 2 Our group also demonstrated that intragastric administration of distilled water can produce significant increases in mesenteric lymph flow, enhanced transport of water-soluble substances into the lymph, and increased flux of albumin through the mesenteric lymph vessels in an animal model. 3 This is likely because of the increased movement of Alb into the interstitial tissues from the jejunal microcirculation; this was confirmed by the finding that intravenously injected Evans blue dye was rapidly transported into the rabbit mesenteric lymph vessels and cisterna chyli. 3 We suggested that increased flux of albumin from the jejunal microcirculation could play a key role in the transport of consumed water into the mesenteric lymph vessels, at odds with the classical concept that water-soluble small molecules travel to the liver through the portal vein.
Based on these findings, we aimed to investigate the effects of water intake on lymph flow through thoracic duct in human participants. We aimed to achieve this through monitoring hemodilution before and after water intake and rest, specifically measuring changes in the blood concentrations of TP, Alb, RBCs, and Hb. We measured changes in the concentrations of sodium ions (Na+) and chloride ions (Cl−), and osmolarity in the urine after 30-minute rest in a supine position, with or without 250 mL distilled water intake.
Our secondary aim was to describe the relationship between changes in the plasma concentration of ADH and changes in urine osmolarity in human participants over the course of our regimen. We expected that changes in plasma concentration of ADH would be proportional to changes in urine osmolarity over the course of the experiment, as a linear relationship between plasma ADH concentrations, ranging from 0.5 to 3.0 pg·mL and urine osmolarity ranging from 0 to ∼450 mOsm·L, is well-described in human beings. 4 The ultimate goal of this study was to establish a nonharmful method of testing urine to estimate lymph flow through the thoracic duct in human participants. A potential application for this method is evaluating the manual technique of a lymph edema therapist.
Materials and Methods
Participants
This study was a single-blinded, randomized, and controlled human trial. A total of 20 healthy volunteers (40.8 ± 3.1 years old, 11 women and 9 men) participated in the study. The ethical committee for human studies at the Shinshu University School of Medicine approved this study (document no. 4348) on May 17, 2019, and all participants gave written and oral informed consent. All study data and procedures were managed in accordance with the concepts outlined in the Declaration of Helsinki. The study was also registered with the University Hospital Medical Information Network in Japan (UMIN-ID R000042133, registered June 6, 2019). All experiments were performed in the morning between 9:00 and 12:00 hours to control for effects of circadian rhythm on the human autonomic nervous system. The temperature and humidity of the experimental room were kept at 22°C and between 40% and 50%, respectively, using air conditioners.
Experimental protocol
Figure 1 shows a detailed experimental protocol for the study. The participants were divided at random into three groups: a control group, a water-intake group with 30-minute rest (group 1), and a water-intake group with 10-minute rest (group 2). All participants micturated immediately before starting the experiment to empty all urine from their bladders. Participants in groups 1 and 2 drank 250 mL of distilled water 10 minutes after miction, whereas participants in the control group did not drink. After 30 minutes sitting following miction, all participants had blood and urine samples taken (first sampling). Participants then rested in a supine position on a bed. The participants from the control group and group 1 rested for 30 minutes, after which blood and urine samples were taken (second sampling). Subjects in group 2 had blood and urine samples (second sampling) taken after just 10-minute rest. All participants were advised not to do deep abdominal respiration during this time. The urine sample in the control, and groups 1 and 2 were taken when the participants were asked to urinate in the first and second sampling. All participants were able to micturate with no trouble, although the participants in the group 2 with 250 mL water intake had a desire to urinate at 10 minutes after the first sampling.
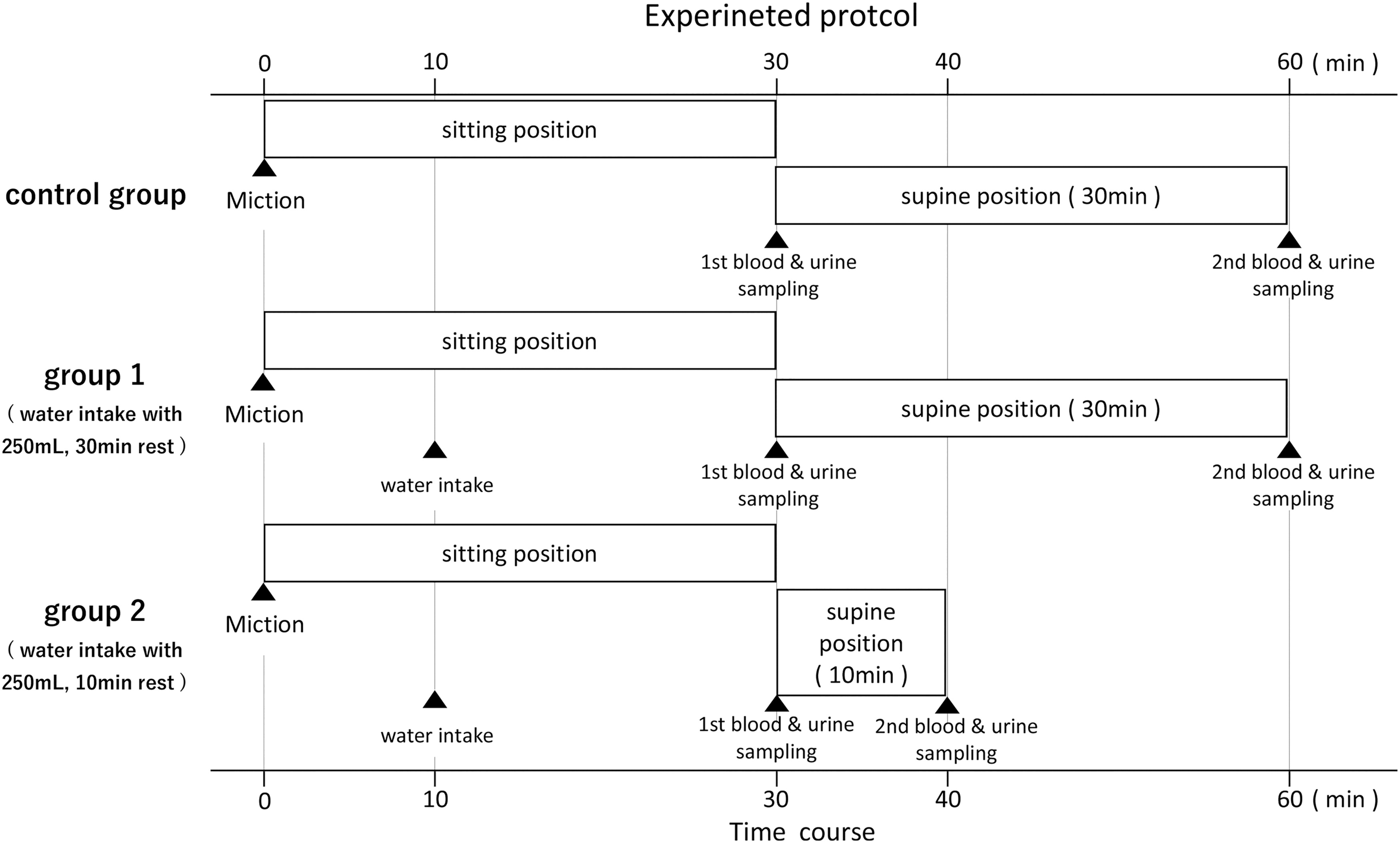
Experimental protocol. A total of 20 healthy volunteers (40.8 ± 3.1 years old, 11 women and 9 men) participated in the study. The participants were divided randomly into three groups: a control group (no water intake with 30-minute rest, n = 8), group 1 (250 mL distilled water intake with 30-minute rest, n = 7), and group 2 (250 mL distilled water intake with 10-minute rest, n = 4).
Components analysis
To evaluate the effects of water intake (distilled water, 250 mL) on hemodilution, the participants' blood concentrations of TP, Alb, RBC, and Hb were measured according to the conventional method by the professional technicians of the Department of Laboratory Medicine at Shinshu University School of Medicine. These technicians also measured the urine concentration of sodium ions (Na+) and chloride ions (Cl−), and the urine ionic osmolarity and urine volume. The participants' ADH concentrations were measured commercially using a radioimmunoassay technique by SRL Ltd. (ISO15189-accredited by the Japan Accreditation Board, RML 00080, Tokyo, Japan).
Statistical analysis
All results are expressed as mean ± standard error. Statistical significance was analyzed using Student's t-test for unpaired observations, or one-way analysis of variance followed by Duncan's post hoc test as appropriate. p < 0.05 was considered statistically significant.
Results
Distilled water intake produced a significant decrease in blood concentrations of TP and albumin
We investigated the effects of an intake of 250 mL distilled water and rest on the concentrations of TP, Alb, RBC, and Hb in human blood. Figure 2 shows the summarized data. In the control group, 30-minute rest in a supine position caused a significant decrease in the concentrations of TP and Alb. A greater reduction in TP and Alb concentrations was observed in water-intake groups 1 (TP, 0.91 ± 0.01, n = 8 vs. 0.93 ± 0.01, n = 7 in the control, p < 0.01; Alb, 0.92 ± 0.01, n = 8 vs. 0.94 ± 0.01, n = 7 in the control, p < 0.05) and 2 (TP, 0.92 ± 0.01, n = 4 vs. control, p < 0.05; Alb, 0.92 ± 0.01, p < 0.05) than in the control group where no water was taken. Reductions in RBC (0.94 ± 0.01, n = 8 vs. 0.96 ± 0.01, n = 7 in the control, p < 0.05) and Hb (0.94 ± 0.01, n = 8 vs. 0.96 ± 0.01 n = 7 in the control, p < 0.05) concentrations were significantly greater in group 1 compared with control; however, in group 2, although the procedure produced a marked reduction in the concentrations of RBC (0.94 ± 0.01, n = 4 vs. control, NS) and Hb (0.94 ± 0.01, n = 4 vs. control, NS), this effect was not significantly different to control. These results confirmed the occurrence of distilled water intake-mediated hemodilution as seen in our previous animal studies. 3
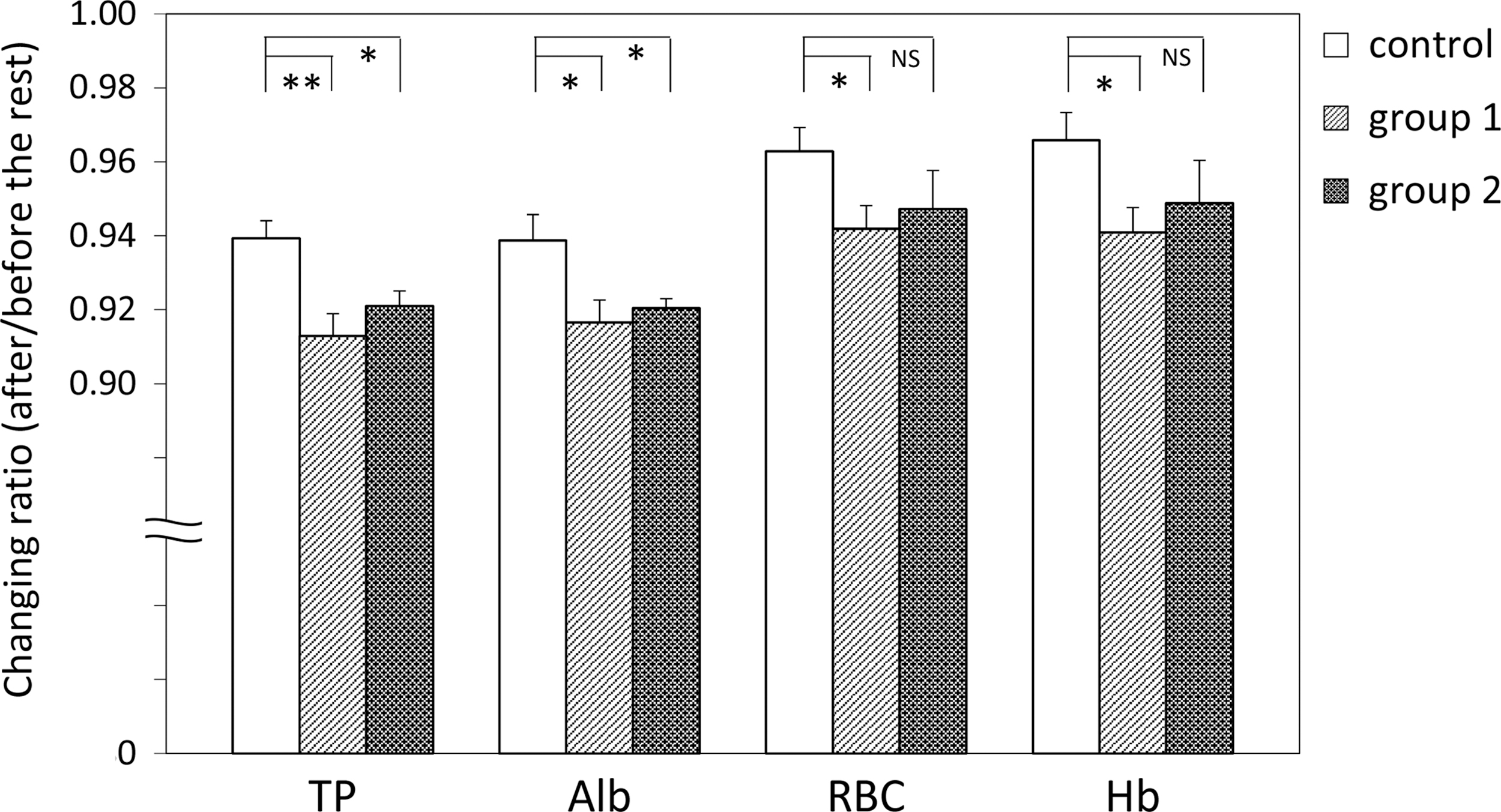
Intake of distilled water by volunteers in groups 1 and 2 produced a significantly greater decrease in the concentration of TP and Alb in the blood compared with the control group. However, a significantly greater reduction in RBC and Hb concentration was only observed after 30-minute rest. Therefore, the procedure for 30-minute rest in the supine position on the bed caused hemodilution, as the concentrations of RBC and Hb were also decreased significantly in this group. The y-axis shows the ratio of each parameter measured after rest against before rest. **p < 0.01, *p < 0.05, NS, not significant. Alb, albumin; Hb, hemoglobin; RBC, red blood cells; TP, total protein.
Distilled water intake caused a significant reduction in urine [Na+], [Cl−], and osmolarity
To evaluate the effects of distilled water intake-mediated hemodilution on the production of urine, we examined changes in urine [Na+], [Cl−], osmolarity, and volume in the experimental participants. Figure 3 shows the summarized data for this experiment. In the control group, no significant changes in the urine [Na+], [Cl−], osmolarity, or urine volume were observed. In contrast, participants from both groups 1 and 2 had significantly greater decreases in urine [Na+] (group 1, 0.43 ± 0.07, n = 8; group 2, 0.49 ± 0.04, n = 4 vs. 1.25 ± 0.15, n = 7 in the control, p < 0.01 each), [Cl−] (group 1, 0.43 ± 0.07, n = 8; group 2, 0.47 ± 0.06, n = 4 vs. 1.09 ± 0.13, n = 7 in the control, p < 0.01 each), and osmolarity (group 1, 0.46 ± 0.07, n = 8; group 2, 0.53 ± 0.04, n = 4 vs. 1.09 ± 0.08, n = 7, in the control, p < 0.01 each) over the course of the experiment than those from the control group. Of interest, participants from group 1 (3.94 ± 0.48, n = 8 vs. 0.80 ± 0.10, n = 7 in the control, p < 0.01), but not group 2 (0.98 ± 0.02, n = 4 vs. control, NS), had a significantly greater increase in urine volume than control participants. Intake of 250 mL of distilled water followed by 10-minute rest in a supine position therefore caused little to no increase in urine volume.

Distilled water intake in groups 1 and 2 caused a significantly greater decrease in urine [Na+], [Cl−], and osmolarity compared with that seen in the control group. Conversely, group 1 urine volume increased significantly compared with control, with no significant difference between group 2 and control. The y-axis is the same as in Figure 2. **p < 0.01, NS, not significant.
Distilled water intake produced a significant decrease in the plasma concentration of ADH after 10-minute rest, but a significant increase after 30-minute rest
We measured the plasma concentration of ADH in the experimental participants to establish the relationship between the plasma concentration of ADH and urine osmolarity, Figure 4 shows the summarized data. Surprisingly, 250 mL distilled water intake with 30-minute rest (group 1) caused a significant increase in the plasma concentration of ADH (1.12 ± 0.07, n = 8 vs. 0.98 ± 0.21, n = 7; p < 0.01). In contrast, in group 2, where participants were rested for only 10 minutes, the change in plasma concentration of ADH was significantly lower than in the control group (0.64 ± 0.04, n = 4 vs. 0.98 ± 0.21, n = 7; p < 0.01).
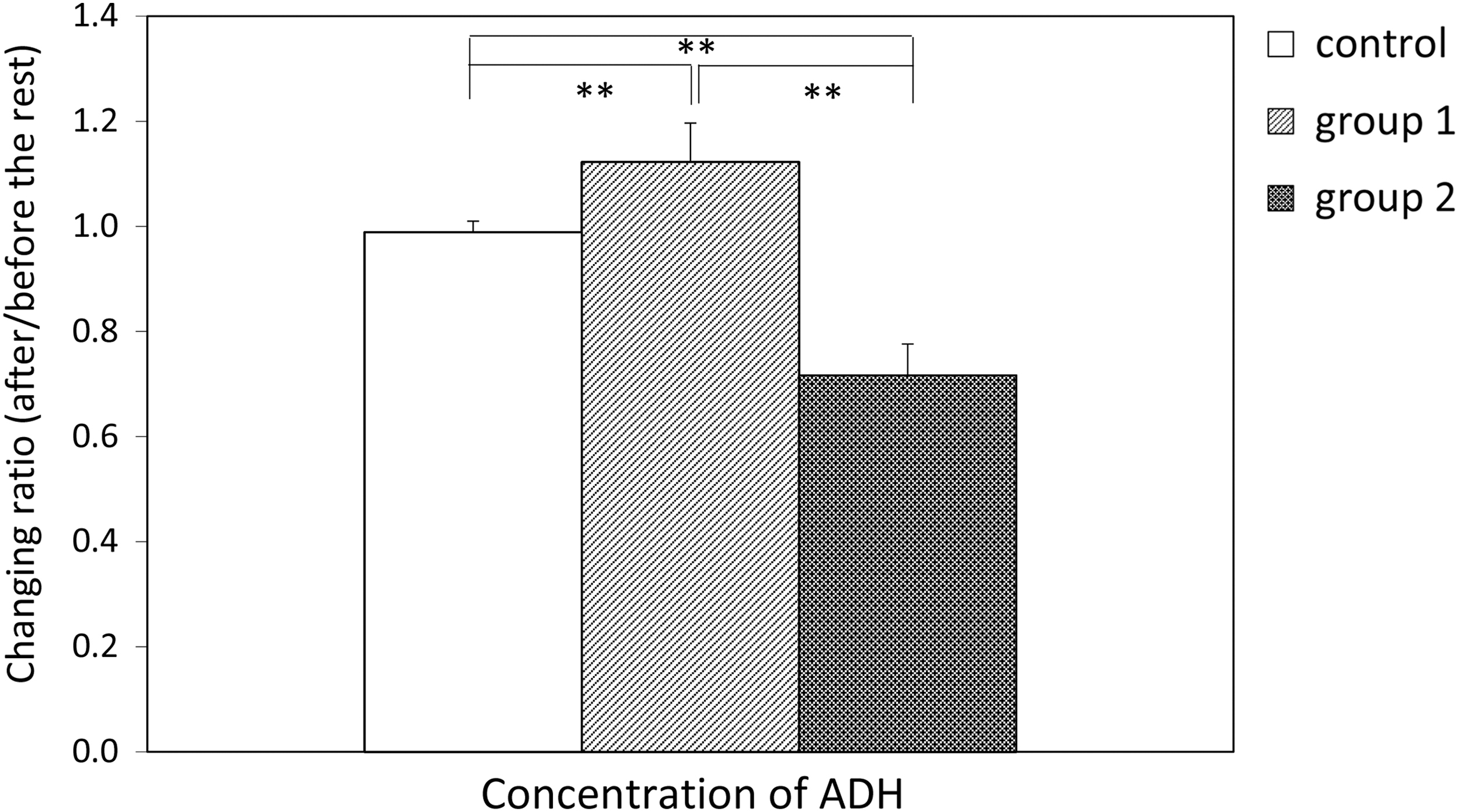
Plasma concentration of ADH was significantly increased over the course of the experiment in group 1 compared with the control group, indicating distilled water intake produced a significant increase in the plasma concentration of ADH after 30-minute rest. Plasma concentration of ADH decreased significantly in group 2, indicating a decrease in ADH levels after 10-minute rest. The y-axis is the same as Figure 2. **p < 0.01. ADH, anti-diuretic hormone.
Linear relationship between the plasma concentration of ADH and urine osmolarity
To assess whether this procedure could be used as a method for evaluating human lymph flow through the thoracic duct using urine osmolarity, we measured the relationship between plasma concentration of ADH and urine osmolarity. Figure 5 shows the data collected from four participants in group 2. The exact plasma concentrations of ADH before 10-minute rest in the four participants were 2.2, 2.5, 3.0, and 2.0 pg·mL, respectively. The corresponding values after 10-minute rest decreased to 1.1, 1.8, 2.1, and 1.3 pg·mL, respectively. In keeping with these data, the urine osmolarity of these participants was also reduced, from 520 to 201, 354 to 194, 370 to 180, and 601 to 240 mOsm·L in each participant, respectively.
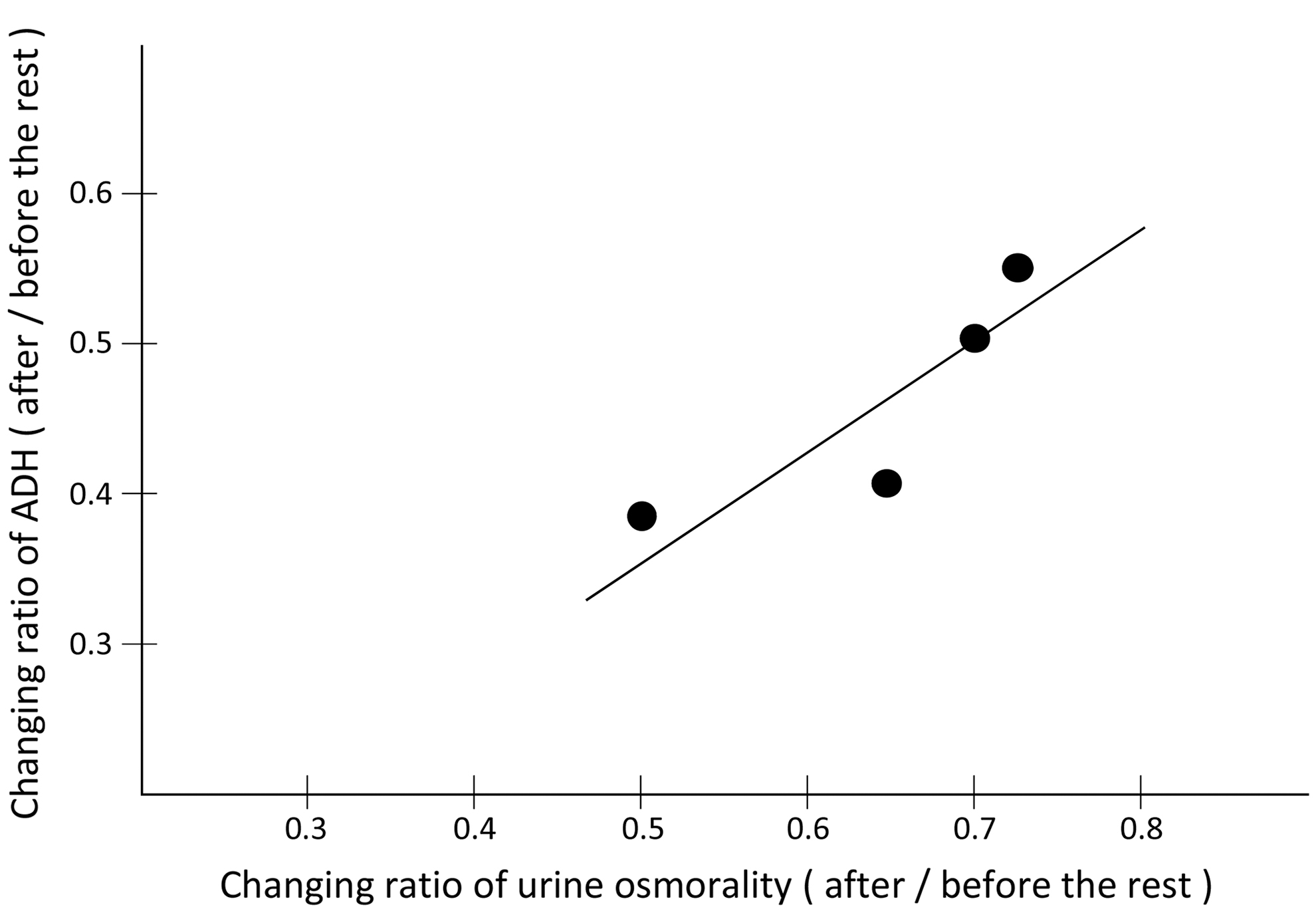
The relationship between the plasma concentration of ADH and urine osmolarity in group 2 (n = 4). The dots show the calculated values of blood ADH and urine osmolarity for each of the group 2 volunteers. The y-axis and x-axis are equivalent to the y-axis in Figure 2.
Discussion
Development of a method for evaluating human lymph flow through the thoracic duct using urine osmolarity
To evaluate human lymph flow through the thoracic duct, we used the procedure of 250 mL distilled water intake with 10- or 30-minute rest in a supine position, instead of abdominal respiration, to accelerate the mesenteric and cisterna chyli lymph flow into the thoracic duct. In previous studies, we demonstrated that intragastric administration of distilled water causes a significant increase in lymph flow through the mesenteric lymph vessels and cisterna chyli in rats in vivo. 3 In keeping with our animal studies, intake of 250 mL distilled water followed by rest produced more marked hemodilution than that seen after rest alone. Intake of 250 mL distilled water with 10-minute rest in a supine position caused a similar reduction in plasma ADH concentration to that produced by abdominal respiration in the supine position. 1 In agreement with the distilled water intake-mediated reduction of plasma ADH, significant decreases in urine [Na+], [Cl−], and osmolarity were observed in the experiments. In addition, an approximately linear relationship between the after/before-rest ratio of plasma ADH (ranging from 1.1 to 3.0 pg·mL) and the after/before-rest ratio of urine osmolarity (ranging from 180 to 601 mOsm·L) was confirmed in this experiment. Based on these findings, we tried to calculate human lymph flow through the thoracic duct using the change in urine osmolarity induced by distilled water intake. This is a reflection of the reduction in the ratio of plasma ADH with body weight-dependent circulatory blood volume in each participant.
In conclusion, 250 mL distilled water intake with 10-minute rest in a supine position caused hemodilution and a decrease in plasma ADH-dependent urine osmolarity. Measuring urine osmolarity could be used as a clinical readout for evaluating human lymph flow through the thoracic duct without the need for blood sampling. This method could also be used as a practical test to evaluate the manual technique of lymph edema therapists. The conclusion was compatible with studies4–6 that have approximated a linear relationship between plasma ADH (ranging from 0.5 to 3 pg·mL), urine osmolarity (ranging from 0 to 450 mOsm·L), and plasma osmolarity (ranging from 270 to 295 mOsm·L).
Sampling time-dependent change in the concentration of plasma ADH
Surprisingly, 250 mL distilled water intake with 30-minute rest in a supine position caused a significant increase in plasma ADH. Urine volume after the procedure was ∼150–180 mL in all participants compared with ∼25–30 mL before the procedure. Higher levels of ADH in the blood could be explained through the activity of a compensatory mechanism. Plasma ionic osmolarity-dependent secretions of ADH from the pituitary gland are broken down in <5 minutes7–10 ; therefore, a reduction in plasma ionic osmolarity related to increased urine volume produced during the 30-minute rest could have stimulated the secretion of plasma ADH. In support of this fact, we confirmed in preliminary rat in vivo experiments that little to no ADH was measured in the mesenteric lymph flow into the thoracic duct.
On the contrary, the action time for plasma ADH-mediated aquaporin receptor-dependent diuresis in the kidneys is known to be ∼15–20 minutes.4,11 Our findings may be mainly related to the difference of urine volume between the 10-minute rest and the 30-minute rest in this experiment. This evidence was able to explain why urine volume in group 2 (250 mL water intake, 30-minute rest) arrived at ∼150–180 mL. The differences of bladder volume and miction sensitivity in each participant may also explain differences in urine volume.
To fully describe a new method for evaluating human lymph flow through the thoracic duct using urine osmolarity, additional studies with more participating volunteers are required to determine the most suitable volume of distilled water to use for intake, and the most reasonable time course for blood and urine sampling.
Footnotes
Acknowledgments
The authors thank Masao Sakaguchi, Norimasa Morimitu, Hideya Momose, Eiji Ikeda, Sigeki Kanai for their assistance with experiments.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Department of Innovation of Medical and Health Sciences Research in Shinshu University School of Medicine was established and is supported financially by donations from BOURBON, Co. Ltd. (Kashiwazaki, Niigata, Japan) and Aizawa Hospital (Matsumoto, Nagano, Japan). This study was financially supported, in part, by Grants-in-Aid for Scientific Research (18K05503, 18K07241) from the Japanese Ministry of Education, Science, Supports, and Culture.