
Abstract
Introduction:
Mass drug administration and morbidity management and disability prevention (MMDP) though considered as two pillars of global program for elimination of filariasis, implementation of MMDP was disregarded in several endemic countries. Limb hygiene is the main component of MMDP and to address its overall clinical benefits, a community-based study was undertaken in three sets of populations.
Materials and Methods:
After obtaining written informed consent, clinical, quality of life (QoL) assessments were carried out and lymphedema volume was measured for three groups of lymphedema patients at intake, at 6, and 12 months follow-up. Filarial lymphedema patients from three sets of villages categorized as “Previous VCRC MMDP,” “State MMDP,” and “Current VCRC MMDP” were considered for the study. Clinical examination and QoL assessment were carried out independently by a medical officer and a sociologist, respectively. Whoever available at the time of three field visits were registered and included in the study. In total, 67, 63, 66 and 75, 74 and 63 lymphedema (LE) patients completed clinical evaluation and QoL assessment from these groups, respectively.
Results:
Assessment of repeated measures of clinical parameters at baseline and two time points of follow-up by Friedman's test showed significant clinical improvements in skin color, texture, moisture, and ulcer (p > 0.05), in nails score and intertrigo score (p > 0.01). Assessed by Wilcoxon signed-rank test showed a significant reduction in the frequency Acute Dermato-Lymphangio-Adenitis episodes at 12 months follow-up in all the three MMDP groups (p < 0.001). However, the reduction of LE volume was significant (p = 0.009) only in the current Vector Control Research Centre (VCRC) MMDP group. There was no significant improvement in the QoL in all three groups.
Conclusions:
To achieve the desired clinical benefits by MMDP home care practices for the filarial lymphedema patients, regular monitoring by the auxiliary health workers is essential. National programs must consider monthly supervision through an integrated approach.
Introduction
World Health Organization (WHO), to eliminate lymphatic filariasis by 2020, launched the Global Programme to Eliminate Lymphatic Filariasis (GPELF) and recommended twin strategies, mass drug administration (MDA) to control transmission of infection in the communities and morbidity management and disability prevention (MMDP) to address the treatment needs of the patients with hydrocele and lymphedema. There is limited information on the burden of these major clinical manifestations of filariasis based on national-level surveys. However, it is estimated that as many as 36 million people suffer from these chronic clinical manifestations that include 16 million lymphedema cases. 1 India launched MDA during the year 2000 and even after 17 years, 255 districts continue to be endemic for filariasis.
MMDP strategy needs to reach >800,000 and 400,000 lymphedema and hydrocele cases registered under the National Vector Borne Diseases Control Programme (NVBDCP) of the country. 2 MMDP aims at mainly minimizing the sufferings of the lymphedema patients and prevent further disease progression through the minimum recommended package that includes prevention of Acute Dermato-Lymphangio-Adenitis (ADLA) and progression of lymphedema.3,4 Lymphedema home care by limb hygiene and effective treatment for ADLA has been found to be effective in preventing further progression the disease.5,6 MDA and MMDP though considered as two pillars of GPELF, implementation of MMDP was disregarded in several endemic countries.1,7 For effective implementation, good health ministry leadership, availability of adequate treatment centers, and committed partners are needed. 8
There are several weaknesses need to be addressed in MMDP implementation. Whereas hydrocele has a surgical cure, lymphedema management is life-long conservative management. The distribution of health care services offering MMDP is scrubby and health professionals lack adequate knowledge. The elimination program also has not recommended specific targets and indicators to assess the successful implementation of MMDP. 9 In the program, the frequency of ADLA attacks and its prevention are considered as main outcome indicators. However, lymphedema patients' major priority is the reduction in lymphedema (LE) volume. Therefore, the program needs to include a reduction in lymphedema volume as one of the major outcome indicator of MMDP.
In addition, other manifestations of skin color, texture, skin folds other secondary skin lesions such as nodules, warts, and intertrigo must also be considered as the important clinical outcome of the MMDP. Improvements of these clinical parameters, in turn, are expected to improve the quality of life (QoL) of the patients. To address these issues, a community-based study was envisaged to assess the impact of ongoing MMDP Programme on clinical outcomes and to identify suitable parameters for evaluation of the impact of the MMDP Programme.
Methodology
Study sites
The study was carried out in Tindivanam and Gingee taluks of Villupuram district of Tamil Nadu State in India. Tindivanam taluk is bordered by the Bay of Bengal on the east, Gingee taluk on the west, Vanur and Villupuram taluks on south, and Cheyyur taluk on the north. As per the India 2011 census, the total population is 446,000 that includes 223,400 males and 222,600 females. The literacy rate of the taluk is 67.66%. Gingee taluk is bordered by Tindivanam on the east, Thiruvannamalai taluk on the west, Villupuram taluk on south, and Vandavasi taluk on the north. As per the India 2011 census, the total population is 422,800 that includes 213,100 males and 209,700 females. The literacy rate of the taluk is 63.41%. Both taluks identified as filariasis endemic areas four decades back and MDA was implemented in 1999. Location of the study villages are shown in Figure 1.

Location of study villages in Villupuram district of Tamil Nadu, India. Group 1,  Group 2, and
Group 2, and  Group 3.
Group 3.
Study population
This includes three groups of lymphedema patients based on the morbidity management services availed from different service providers.
Group 1—Previous Vector Control Research Centre Morbidity Management and Disability Prevention
Vector Control Research Centre (VCRC) had wide field practice areas in Villupuram and Cudallore districts of the Tamil Nadu State to carry out research on filariasis transmission control. These populations were under the supervision of the research teams and MMDP was also provided by the research teams for >5 years. However, MMDP activities were withdrawn about 8 years back and handed over to the state government. This includes a set of lymphedema patients from six villages (Alagramam, Avvaiarkuppam, Peramandur, Chinnanergunam, Muppili, and Thenkalavai) currently receiving MMDP from Tamilnadu State NVBDCP. This group of the population was considered to know the sustainability of the long-term supervision of MMDP activities by a trained service provider.
Group 2—state MMDP
This includes a set of lymphedema patients from nine villages (Nedi, Mozhianur, T. pudupalayam, Sithani, Kongarapattu, Thenber, Chinnathachur, Sendiambakkam, and Mupuli) that has been receiving MMDP from Tamilnadu State NVBDCP. This group of the population was considered for the impact of MMDP under programme mode.
Group 3—Current VCRC MMDP
This includes a set of lymphedema patients from nine villages (Kavarai, Kappai, Olakur, Vairapuram, Ponpathi, Palapattuu, Sithampoondi, Beerangimedu, and Melkaranai) received MMDP under the supervision of the VCRC and were followed up on monthly basis. This group of the population was considered for the impact of MMDP under supervision.
Procedures
The Scientific Advisory Committee (SAC) of VCRC approved the study proposal and Institutional Human Ethics Committee (IHEC) of VCRC cleared the proposal for implementation.
Prerecruitment surveys
A team of trained technical staff visited the identified villages with the available list of LE cases and confirmed their availability through a door-to-door survey. All LE cases identified by the field teams were recorded on the “Proforma for enumeration of LE patients.”
Recruitment procedures
Case confirmation and informed consent
All LE cases identified by the trained technical staff were examined by a medical officer for clinical confirmation of LE and suitability for the study. Old infirm patients, patients suffering from ADLA at the time of examination, and patients not willing to participate in the study were excluded. Principal investigator or his representative explained the study procedures to the patients and provided the written information sheet in the local language. After clarifying the doubts, if any, the investigators obtained written consent from each patient willing to participate in the study. All the participants were aware that they have the right to withdraw from the study at any point of time without assigning any reason and the withdrawal from the study will not affect their liberty to get the routine MMDP services from the NVDCP clinics or primary health centers.
Clinical examination
One medical officer assessed the patients and recorded his findings on clinical report form. The medical officer was trained in lymphedema assessment as per the “Training module on community home-based prevention of disability due to lymphatic filariasis—Tutor's Guide”—WHO/CDS/CPE/CEE/2003.35—Part 2 in 2006 and continues to manage the filariasis clinic for the past 12 years independently. The clinical examination included skin condition of lower limbs, color, texture, moisture, ulcer, nodule, and skin folds. Toe-web intertrigo was clinically assessed for depth, redness, itching, pain, and discharge. Toenails were assessed for discoloration and cracks. Each of the aforementioned parameters was scored clinically based on preset criteria as given hereunder:
“0” normal compared with finger nails; “1” mild discoloration; “2” moderate discoloration; “3” black; “4” brittle and cracks
In addition, the number of ADLA attacks endured for the past 1 year was obtained by the recall. One year recall has been considered as acceptable as ADLA episode that incapacitates the patients could be remembered for a long period.10,11
Volume measurement
Water displacement volumetry described by Beach RB 12 is the gold standard method and the same procedure was carried out in the study. In brief, the patient immersed the unaffected limb in the water-filled to a preset level to which a calibrated glass tube was attached and the water displaced into the calibrated glass tube was recorded. This procedure was repeated for the affected limb. The difference between these two readings was referred to the volume chart and recorded as lymphedema volume.
Quality of life assessment
QoL assessment was done by a social worker using a standardized VCRC 7D5L questionnaire, which is an extended form of EuroQoL 5D7L.
A structured and pretested questionnaire was used on each patient and data for different health domains such as physical, psychological, social functions, and symptoms were elicited. 13 The severity levels were scored by assigning a numerical value between 0 and 4. The score 0 is given to worst quality and 4 is given to best quality. Lower scores indicate a more negative impact of the disease and poorer QoL, and higher scores indicate greater QoL.
Training of the patients
Patients in Group 3 received the training on “limb hygiene” procedures. Trained staff nurse demonstrated limb hygiene procedures in small groups of 3–6 patients in one of the houses of the LE patients. After the demonstration, each patient performed the limb hygiene procedures under the supervision of the trainer and any imperfection observed was corrected by the trainer in the field. This group of patients also received a kit containing the materials for maintaining limb hygiene. In addition, these patients also recorded the practice of limb hygiene on a day-to-day basis and the fever/ADLA episodes on a monthly calendar provided to them.
Follow-up
Patients in Groups 1 and 2 were followed up at 6 and 12 months after the intake. Clinical examination and scoring as described at intake were carried out for all the clinical parameters. Volume measurement and QoL assessment were also repeated and recorded without referring to the findings at intake. Patients in Group 3 were visited once a month emphasized on limb hygiene and provided limb hygiene materials.
Statistical analysis
Data were entered in Microsoft Excel and cross-checked before analysis. Simple statistics such as proportions/percentages, mean and standard deviation, median and interquartile range for the variables age, gender, ADLA annual frequency, ADLA duration, LE volume, LE Grade, QoL score, skin color, texture, moisture, ulcer, nodule, skin folds, toe-web intertrigo score, and toe-nail score were calculated appropriately groupwise for each of the time point. To compare the aforementioned variables between groups at intake, the Kruskal–Wallis test was applied. To compare the aforementioned variables between time points for each group, Friedman test for repeated measures was used followed by Wilcoxon signed-rank test for pairwise comparisons. All these analyses were carried out on SPSS software (IBM SPSS Statistics for Windows, Version 22.0. IBM Corp., Armonk, NY. Released during 2013) and the level p < 0.05 was considered as significant.
Results
In total, 172, 90, and 96 lymphedema patients from three sets of populations were enlisted, respectively. Among these, based on the availability and willingness to give written informed consent, 67, 63, 66 and 75, 74 and 63 LE patients completed clinical evaluation and QoL assessment from “Previous VCRC MMDP,” “State MMDP” and “Current VCRC MMDP,” respectively. The characteristics of the participants are given in Table 1. As seen in other surveys, the proportion of female patients was more and the grade-1 LE was very less. Age, ADLA frequency, ADLA duration, and LE volume at intake was similar in all the three groups. About 50% lymphedema patients from all the three groups had more than two episodes of ADLA annually and >500 mL of lymphedema volume.
Details of the Participants Recruited in Three Study Groups
ADLA, Acute Dermato-Lymphangio-Adenitis; LE, lymphedema; MMDP, morbidity management and disability prevention; SD, standard deviation; VCRC, Vector Control Research Centre.
Twelve clinical parameters were considered to assess the impact of the MMDP Programme in three different settings. The median score and the minimum, maximum score (in parenthesis) for each of these parameters are given in Table 2 and these parameters were assessed by the Kruskal–Wallis test. At intake, it was observed that the clinical scores for the skin color, ulcer, warts, nodule, skin fold, intertrigo, toenails, ADLA frequency, ADLA duration, and LE volume were similar (p > 0.05). However, the clinical score for the skin texture and moisture were significantly different (p < 0.05) among the three groups at intake itself (Table 2).
Comparisons of the Clinical Parameters of Three Morbidity Management and Disability Prevention Groups at Intake
Kurskal–Wallis test.
Repeated measures of clinical parameters at baseline and two time points of follow-up (at 6 and 12 months) were compared using Friedman's test, and it was observed that there were significant changes in skin color, texture, and ulcer in Previous VCRC MMDP and in skin color, texture and moisture in State MMDP, respectively. However, in Current VCRC group, we observed significant change in four clinical parameters: skin color, texture, moisture, and ulcer (Table 3).
Comparisons of Skin Clinical Parameters at Intake, 6, and 12 Months
Friedman's test.
Friedman's test on comparison of intertrigo score and toenails score showed that there was a significant change in toenails score (p = 0.007) in Previous VCRC MMDP group at 12 months follow-up. However, there were significant clinical improvements in both intertrigo score and toenails score in State MMDP group (p = 0.019; p = 0.028) and in Current VCRC group (p = 0.001; p = 0.013), respectively (Table 4).
Comparisons of Intertrigo and Toenails at Intake, 6, and 12 Months
Friedman's test.
Pairwise comparison of the differences in median scores at 6 and 12 months follow-up for each skin clinical score using Wilcoxon signed-rank test was carried out to know the improvements in clinical parameters. Table 5 depicts the changes in the other skin clinical scores in all three groups. It was observed that there were significant clinical improvement in skin color and texture in the Previous VCRC MMDP group and State MMDP group at 6 and 12 months follow-up (p < 0.05). However, in Current VCRC group, there was a significant improvement in skin color, texture, and moisture at 6 months (p < 0.05), and further improvements at 12 months follow-up (p < 0.05) in addition to the clinical improvement in ulcer at 12-month follow-up (p < 0.05).
Pairwise Comparisons of Skin Clinical Parameters Between Intake and 6 Months as Well as Between Intake and 12 Months
Wilcoxon signed-rank test.
Pairwise comparison of the differences in median scores at 6 and 12 months follow-up for intertrigo and toenails using Wilcoxon signed-rank test was carried out to know the clinical improvements. Clinical improvement was observed in intertrigo at 6 and 12 months follow-up in Previous VCRC MMDP group (p < 0.05). In State MMDP group clinical improvement in intertrigo was not observed at 6 months follow-up (p = 0.10). Under Current VCRC MMDP group clinical improvements (p < 0.05) were observed in intertrigo as well as in toenails at both 6 and 12 months follow-up (Table 6). Similarly, there was a significant reduction in ADLA frequency in all the three MMDP groups at one follow-up (p < 0.01).
Pairwise Comparisons of Intertrigo and Toenails Between Intake and 6 Months as Well as Between Intake and 12 Months
Wilcoxon signed-rank test.
However, there was no significant reduction in LE volume at 12 months follow-up in Previous VCRC and State MMDP groups (p = 0.29 and p = 0.81). However, reduction of LE volume was significant (p ≤ 0.001) only in Current VCRC MMDP (Table 7).
Pairwise Comparisons of Acute Dermato-Lymphangio-Adenitis Frequency and Lymphedema Volume Between Intake and 12 Months
Wilcoxon signed-rank test.
Impact of MMDP on the HRQoL of lymphatic filariasis patients
Comparison of baseline HRQoL scores and HRQoL scores after 1 year
The health-related quality of life (HRQoL) scores of the three groups of lymphatic filariasis (LF) patients who received MMDP package from three different sources were assessed using the VCRC 7D5L questionnaire, which is an extended form of EuroQoL 5D7L. The baseline HRQoL and HRQoL assessed after 1 year indicate that the QoL has come down in grade 3 and grade 4 LF patients in Groups 1 and 2 villages (Figs. 2 and 3). However, the difference is not statistically significant. The QoL in LF patients in Group 3 is maintained at 1 year, including grade 3 and 4 LF patients (Fig. 4). The baseline HRQoL scores and the scores after 1 year were almost similar. However, it was observed that the QoL scores were not lower than the baseline scores as in the case of Groups 1 and 2. The reason could be due to the regularity of limb hygiene practiced by the patients as these patients were on monthly supervisory visits.

Group 1. AQS at baseline and at 1 year follow-up. AQS, average quality score.
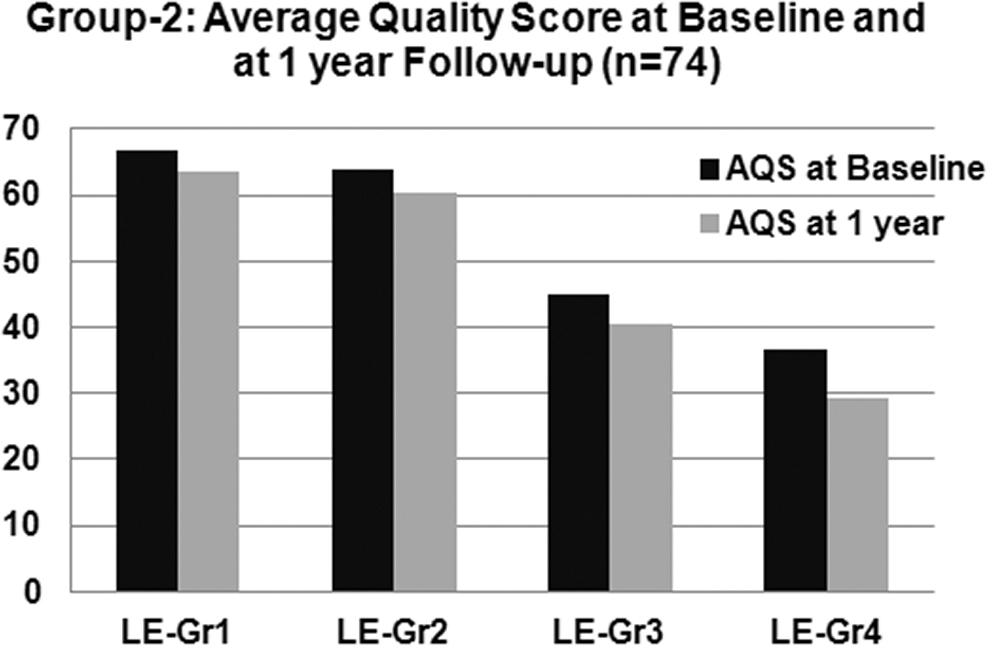
Group 2. AQS at baseline and at 1 year follow-up.

Group 3. AQS at baseline and at 1 year follow-up.
Discussion
There are several unsettled issues in filarial lymphedema, including the factors that trigger the onset of edema. The progression of lymphedema is usually slow and factors associated are complex. However, recurrent episodes of ADLA play a significant role in lymphedema progression.14–16 To achieve elimination, the minimum package of home care advocated by WHO needs to be expanded to 100% geographical areas in endemic countries. 4 It is well established through several studies that practicing regular limb hygiene as home care effectively brings down the frequency of ADLA attacks.17–20 However, despite achieving the transmission control to a great extent through annual MDA, the MMDP component of the national filariasis elimination program in several filariasis endemic countries gained minimal attention. It is evident that only 34 filariasis endemic nations have implemented MMDP component and of these only 25 nations monitor the MMDP coverage under the program. 1 It was also observed that complete geographical coverage was not achieved despite implementing the MMDP services. Underutilization of MMDP services offered in exclusive filariasis clinics due to lack of awareness among the patients and health providers is also a major issue that requires specific attention. 21
Although MMDP is aimed at the prevention of recurrent episodes of ADLA and further progression, LE patients expect overall improvements especially reduction in LE volume. Several investigators observed a reduction in lymphedema volume after therapy under institutional setup.6,22 However, accessibility and affordability are the major concerns for availing institutional therapy in poor resource settings. It has been established that patients hesitate to utilize morbidity management services due to a lack of confidence in treatment outcome. 7 One of the major weaknesses of the MMDP in filariasis elimination program is that the effect of limb hygiene on LE volume and the associated clinical parameters under program mode have not been studied at all. To get the community support and patients' compliance for MMDP, it is highly desirable that treatment assures overall improvement in clinical conditions of LE, including volume reduction.
In this study, the investigators looked into the clinical benefits achieved by the LE patients through limb hygiene in three different sets of populations with exposure to three MMDP service resources. The difference in median scores between intake and at 6, 12 months follow-ups was considered for the pairwise comparison with appropriate nonparametric tests. In addition, the impact on the QoL of the LE patients in a short span of 1 year was also assessed. Results of the study have shown that clinical improvement with reference to skin conditions, intertrigo, toenail conditions, and also reduction in the frequency of ADLA episodes are possible with MMDP under program condition. However, LE volume reduction in the patients' pre-eminent expectation could be achieved only under the Current VCRC group as the patients from this group received monthly support and supervision by the health workers. It has already been shown that MMDP implementation, if unsupervised, frequency of ADLA will increase. 23 Yahathugoda et al. observed significant improvement in clinical parameters and reduction in LE volume in both the groups of patients under daily as well as monthly follow-up schemes and there was no significant difference between the two groups. 24 This indicates that monthly supervision is sufficient to motivate the patients to follow the home care procedures. It was also found to be feasible to implement integrative management of lymphedema in resource-poor village settings as home care management after training with the desired outcome in terms of reduction in LE volume among the patients with large volume lower extremities. 25 If accessibility and affordability are ensured, patients can be easily motivated to achieve the desirable effects. It has already been shown that once the patients were motivated to be responsible for their own treatment outcome, the response in terms of reduction LE volume was better among the self-care group compared with the patients treated by the physiotherapists. 26
This study also showed that despite achieving the improvements in clinical parameters and reduction in LE volume under current MMDP group, there was no significant improvement in the LEHRQoL. Impact on QoL in chronic diseases such as filarial lymphedema has been built over a period of time and determined by several factors and, therefore, the QoL was not improved in a short period of 1 year.
The major limitation of the study is that only the available patients at the time of visit to the villages were included in all the three sets of populations. We have not attempted to select the participants by random. The second limitation is that two villages in Group 2 were in proximities to two or three villages in Group 3 and few of the patients also availed MMDP services from more than one source. Therefore, contamination of information and services could not be avoided due to ethical reasons.
Conclusions
This study showed that it is possible to achieve the desired clinical benefits, including a reduction in LE volume by MMDP home care practices. However, to achieve the desirable clinical benefits regular monitoring by the auxiliary health workers is essential. The ELF programs envisage that even after achieving the transmission control, the activities under MMDP need to be continued as chronic manifestations of filariasis continue to remain in the population and several cases continue to be detected or reported for another two or three decades. National filariasis elimination programs must initiate steps to provide MMDP services through primary health care portal and the health system should be strengthened to meet these challenges. National lymphatic filariasis elimination program needs to ensure that MMDP impact assessments are carried out at regular intervals, including the clinical parameters, ADLA and LE volume as indicators in addition to operational indicators.
To achieve improvement in QoL, long-term strategies in coordination with the social welfare department have to be devised and implemented in the communities. Or else, joint programs as in Ethiopia for filariasis and podoconiosis 27 may have to be streamlined to have better access and monitoring under the program. In India, leprosy is re-emerging in states declared to have reached the elimination stage and, therefore, leprosy-filariasis joint control program can be considered as an option for more accessibility to the patients of leprosy and filarial LE patients. Once the patients are motivated, the success is not far away.
Footnotes
Acknowledgments
First, the authors thank all the participants from all the villages for their participation, especially the participants from Group 3 for their regularity in attendance and in following the instructions. Technical supports provided by Mr. Kumareson, P.M. Azad, and Mr. Joseph are also gratefully acknowledged. We thank Dr. P. Jambulingam, Director VCRC, for providing infrastructural facilities and providing intramural funding for the project.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Indian Council of Medical Research (ICMR), Ministry of Health and Family Welfare, Government of India funded this project IM1401CEC through the intramural funding of the VCRC, Pondicherry.