
Abstract
Background:
The mechanisms of lymphangiogenesis in the cholestatic liver after partial hepatectomy (PH) remain unclear. We aimed to demonstrate the relationship between lymphangiogenesis and liver regeneration after partial hepatectomy in the cholestatic liver.
Methods and Results:
C57BL/6 mice were subjected to 70% partial hepatectomy only (PH group, n = 20) and 70% partial hepatectomy with temporary common bile duct (BD) obstruction by clipping (BD+PH group, n = 20). Five mice per group were sacrificed at 1, 3, 5, and 7 days after the procedure. The liver function was examined by blood tests, and the liver regeneration rate was assessed by body weight and liver weight. Immunohistochemical staining of lymphatic vessel endothelial hyaluronan receptor-1 (LYVE-1) showed liver lymphangiogenesis. The gene expression of lymphangiogenesis-associated factors (e.g., vascular endothelial growth factor receptor-3 [VEGFR-3]) was examined by a real-time polymerase chain reaction. The liver function in the BD+PH group was worse than that in the PH group on postoperative day 1 (POD1) (aspartate aminotransferase: 6528 ± 1641 U/L vs. 2741 ± 368 U/L, p < 0.05, alanine aminotransferase: 4160 ± 1255 U/L vs. 2315 ± 357 U/L, total bilirubin: 1.36 ± 1.16 mg/dL vs. 0.09 ± 0.01 mg/dL), and the liver regeneration rate in the BD+PH group was worse on POD7 (4.57% vs. 5.91%, p < 0.05). The LYVE-1 expression in Glisson's capsule peaked on POD5 and POD7 in the PH and BD+PH groups, respectively. The peak gene expression of VEGFR-3 in the BD+PH group was delayed in comparison with the PH group.
Conclusions:
Lymphangiogenesis after partial hepatectomy in the cholestatic liver was suggested to be delayed due to impaired liver regeneration and the late expression of VEGFR-3.
Introduction
Intrahepatic cholangiocarcinoma (ICC) is the second-most common type of primary liver cancer following hepatocellular carcinoma. 1 Although liver resection is considered the only option for the curative treatment for ICC, the prognosis remains unsatisfactory even when aggressive surgical treatment is performed.2,3 According to several large studies, the reasons for poor prognosis of ICC include the fact that it easily spreads beyond the liver through the lymph system and that it is associated with more dynamic lymphangiogenesis.4,5 In addition, cholestasis and inflammation are common features of advanced ICC. 6 Thus, a better understanding of the hepatic lymph system and lymphangiogenesis after partial hepatectomy in the cholestatic liver might be an important key for improving the prognosis of ICC and for development of adjuvant therapies.
A few studies have reported that lymphangiogenesis in the liver occurs in various situations, such as tissue repair, 7 inflammation, 8 and malignant tumors.1,2,9 Lymphatic vessel endothelial hyaluronan receptor-1 (LYVE-1) 10 and vascular endothelial growth factor receptor-3 (VEGFR-3) 11 are the lymphatic vessel markers that are most commonly used for the investigation of lymphangiogenesis in the liver. LYVE-1 is a homologue of the CD44 hyaluronan receptor. CD44 is widely expressed in the epithelium and cells of hematopoietic origin, while the expression of LYVE-1 is restricted to the lymphatic endothelium and is not detected in blood vessels. 12 Furthermore, VEGFR-3 is a membrane-anchored tyrosine kinase and is activated by VEGF-C and VEGF-D, which initiate intracellular signaling cascades leading to lymphangiogenesis. 13 It also plays a critical role in the pathogenesis of different proliferative events during chronic liver diseases, including that of lymphatic vessels and cholangiocytes. 14
Liver regeneration after partial hepatectomy in mice generally requires approximately 5–7 days.15,16 Meanwhile, liver cholestasis after partial hepatectomy has been found to significantly inhibit liver regeneration. 17 However, the mechanisms of lymphangiogenesis in the cholestatic liver and regenerating liver after partial hepatectomy have remained unclear. The aim of this study was to investigate the relationship between lymphangiogenesis and liver regeneration after partial hepatectomy in the cholestatic liver.
Materials and Methods
Animal models
We used 8-week-old male and female C57BL/6 mice (Charles River Laboratories, Japan) for this study. All experiments received approval from the Institutional Animal Care and Use Committee of Nagasaki University (No. 1706061384-2), and the experiments were performed in accordance with institutional and national guidelines. Animals were housed at ∼24°C with constant humidity and a 12-hour light/12-hour dark cycle. Mice had ad libitum access to food and water. Before the experiments, the mice were randomly apportioned to several groups.
A total of 43 mice were subjected to liver harvest only (control group, n = 3), 70% partial hepatectomy only (PH group, n = 20) and 70% partial hepatectomy with temporary common bile duct obstruction (BD+PH group, n = 20). The surgical procedures were performed according to the methods of a previous study.18,19 Briefly, after the induction of general anesthesia, laparotomy was performed using midline abdominal skin and muscle incisions. For the control group, the liver was harvested without common bile duct injury. For the BD+PH group, the common bile duct was exposed and obstructed with a clip. After 12 hours, the clip was removed from the bile duct and 70% partial hepatectomy was performed. For the PH group, we only exposed the common bile duct (without obstruction) and then performed 70% partial hepatectomy. Five mice in each group were sacrificed at 1, 3, 5, and 7 days after the procedure, respectively.
Biochemical assay of blood samples
Blood was collected from the heart of mice at the time of sacrifice, and then, serum was obtained by centrifugation (3000 rpm for 5 minutes). The levels of total bilirubin (T-Bil), aspartate aminotransferase (AST), and alanine aminotransferase (ALT) were measured using standard laboratory methods.
Regeneration of the liver
The body weight was measured under anesthesia before the operation. The liver was extracted and weighed. The liver weight to body weight (LW/BW) ratio was calculated to evaluate the regenerative ability of the liver.
Hematoxylin and eosin staining
The liver tissue was fixed with 4% paraformaldehyde (Wako Pure Chemical Industries Ltd., Osaka, Japan) for 24 hours, dehydrated with high concentrations of ethanol, embedded in paraffin (Paraplast Plus; Leica Biosystems, Inc., Richmond, IL), and then cut into sections of 5-μm thickness. The sections were stained with hematoxylin and eosin (Muto Pure Chemicals Co. Ltd., Tokyo, Japan). All staining procedures were performed according to the standard staining protocol.
Immunohistochemical analysis
The sections were deparaffinized with xylene and rehydrated in a graded ethanol series. After treatment with preheated pH 9.0 target retrieval solution (Agilent, Santa Clara), the slides were cooled with water for 20 minutes. The sections were rinsed in phosphate-buffered saline and soaked for 10 minutes at room temperature in peroxidase-blocking solution (Agilent). The rabbit monoclonal anti-mouse LYVE-1 antibody (1:200 dilution; Abcam, Cambridge, United Kingdom) was used as the primary antibody. The sections were incubated overnight at 4°C. After washing, sections were treated with horseradish peroxidase-labeled polymer conjugated to goat anti-mouse and rabbit immunoglobulins (Agilent) at room temperature for 30 minutes. Then the sections were stained with 3,3-diaminobenzidine tetrahydrochloride containing hydrogen peroxide (Agilent). The stained sections were observed under an inverted microscope (DP-74; Olympus, Tokyo, Japan).
The number of lymphatic vessels (the expression of LYVE-1) located in Glisson's capsule was counted, and the examined area of the liver was measured. We compared the expression of lymphatic vessels in Glisson's capsule per 100 mm2 and the number of lymphatic vessels per Glisson's capsule.
Quantitative real-time polymerase chain reaction analysis
The liver tissues at each time point were used for mRNA extraction using a spin column (NucleoSpin RNA II; Macherey-Nagel, Düren, Germany) according to the manufacturer's instructions. cDNA was synthesized from total RNA using a high-capacity cDNA reverse transcription kit (Applied Biosystems, Tokyo). The samples were stored at −20°C until use in the polymerase chain reaction (PCR).
The PCR was performed on an Applied Biosystems StepOnePlus Real-time PCR system using the TaqMan Gene Expression Assay Kit (VEGFR-3: FMS-like tyrosine kinase 4: Mm01292604_m1, VEGFR-2: kinase insert domain receptor Mm01222419_m1, HGF: met proto-oncogene: Mm01156972_m1; Applied Biosystems). In brief, PCR amplification was performed using a reaction mixture containing 1 μL of cDNA sample, 0.5 μL of TaqMan Gene Expression Assay probe, 5 μL of TaqMan Fast Universal PCR Master Mix solution (Applied Biosystems), and 13.5 μL of nuclease-free water. Each amplification cycle consisted of 1 second at 95°C and 20 seconds at 60°C. A total of 40 amplification cycles were performed. The expression levels were normalized to that of GAPDH (control liver tissue was set as 1.0), and the mRNA expression was determined using the comparative cycle time (ΔΔCt) method.
Statistical analyses
All statistical analyses were performed using BellCurve for Excel version 2.21 for Windows (Social Survey Research Information Co., Ltd., Tokyo, Japan). All data are presented as mean ± standard deviation. Differences between two groups were calculated using Tukey's honest significant difference test. The means of continuous numerical variables were compared using a one-way ANOVA (analysis of variance). p-Value of <0.05 was considered statistically significant.
Results
Liver function of cholestatic liver after partial hepatectomy
Table 1 shows that the levels of T-Bil, AST, and ALT rapidly increased and reached a peak on postoperative day 1 (POD1). Thereafter, they decreased sharply at POD3. In the BD+PH group, the level of AST on POD1 was significantly higher than that in the PH group (6528 ± 1641 U/L vs. 2741 ± 368 U/L, p < 0.05). Regarding the ALT and T-Bil levels on POD1, no statistically significant differences were detected among the groups; however, the level of ALT in the BD+PH group was higher than that in the PH group (ALT: 4160 ± 1255 U/L vs. 2315 ± 357 U/L, T-Bil: 1.36 ± 1.16 mg/dL vs. 0.09 ± 0.01 mg/dL).
Blood Test Result
PH: 70% partial hepatectomy only; BD+PH: 70% partial hepatectomy with temporary common bile duct obstruction by clipping.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; POD; postoperative day; T-Bil, total bilirubin.
Liver regeneration of cholestatic liver after partial hepatectomy
The LW/BW ratio in the PH group increased with time until POD7 (Fig. 1). However, the LW/BW ratio in the BD+PH group increased slowly and was still significantly lower on POD7 (4.57% vs. 5.91%, p < 0.05), indicating poor regeneration in the cholestatic liver.
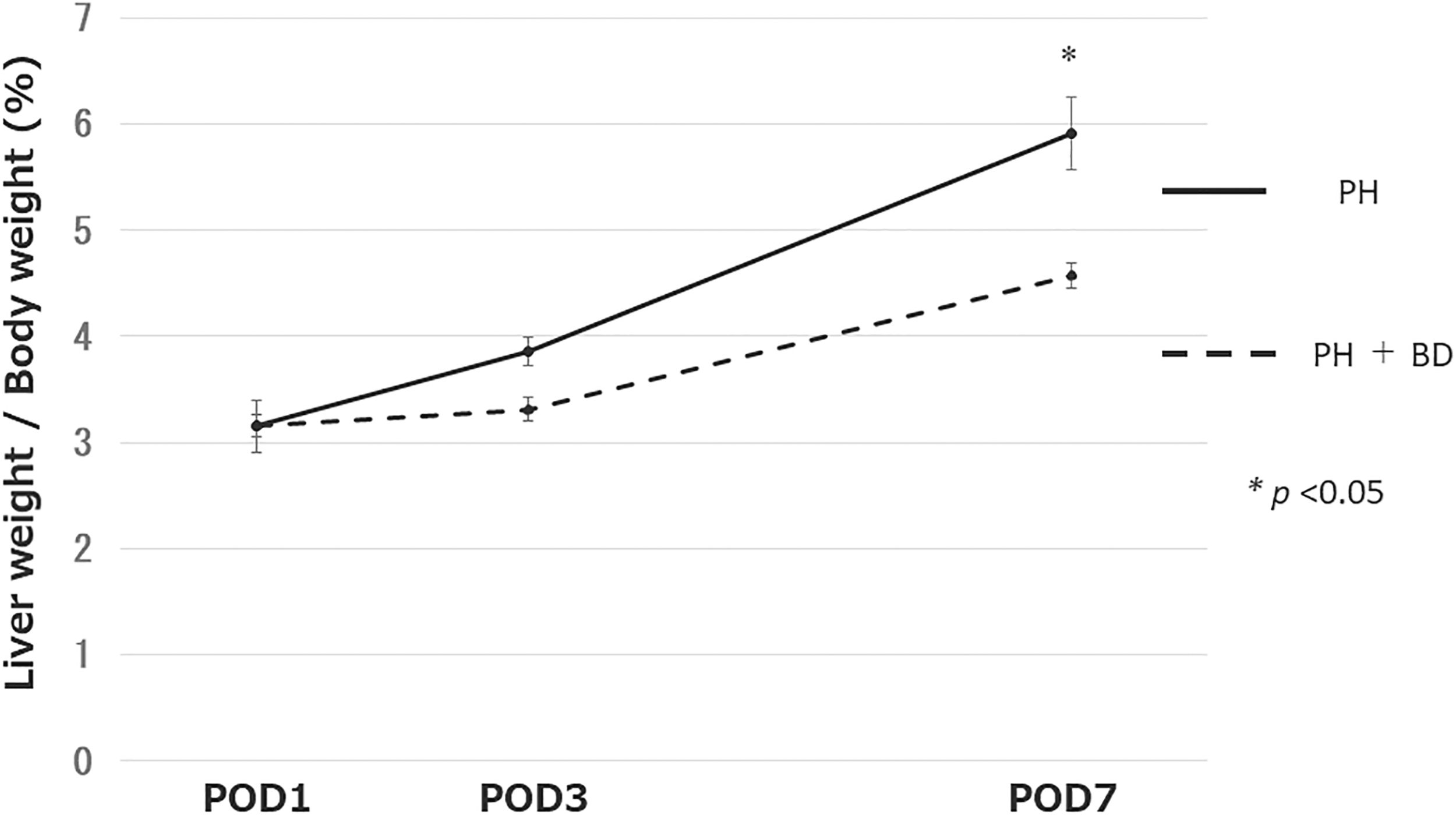
Regenerative ability of the liver. The liver weight to body weight ratio of mice in the partial hepatectomy only (PH) and partial hepatectomy with temporary common bile duct obstruction with a clip (BD+PH) groups at 1, 3, and 7 days after procedure.
Lymphangiogenesis after partial hepatectomy
Lymphatic vessels were observed around Glisson's capsule, as shown in Figure 2A. The expression of lymphatic vessels in Glisson's capsule per 100 mm2 in the PH group peaked on POD5 (POD1: 36.7% ± 3.6%; POD3: 43.4% ± 5.4%; POD5: 52.4% ± 2.3%; POD7: 42.0% ± 3.2%) and at POD7 in the BD+PH group (POD1: 30.5% ± 6.1%; POD3: 47.1% ± 2.1%; POD5: 51.4% ± 1.7%; POD7: 55.2% ± 3.6%) (Fig. 2B). In each group, the peak value was significantly higher than the lowest value on POD1 (p < 0.05). The number of lymph vessels per Glisson's capsule was similar to that of lymphatic vessel expression, that is, it peaked on POD5 in the PH group (POD1: 0.87 ± 0.14; POD3: 0.98 ± 0.24; POD5: 1.30 ± 0.12; POD7: 0.98 ± 0.19) and at POD7 in the BD+PH group (POD1: 0.83 ± 0.24; POD3: 1.10 ± 0.14; POD5: 1.06 ± 0.19; POD7: 1.37 ± 0.18) (Fig. 2C). However, the difference between the peak value and the lowest value was not significant.

Lymphangiogenesis after partial hepatectomy.
The gene expression levels after partial hepatectomy
The gene expression of VEGFR-3 peaked on POD5 in the PH group and POD7 in the BD+PH group (Fig. 3A). Although the PH group of peaked value was significantly higher than the lowest value at POD1 (p < 0.05), no significant difference was observed in the values of the BD+PH group. The expression of VEGFR-2, which is associated with angiogenesis and lymphangiogenesis, also peaked on POD5 in the PH group, but the highest and the lowest values showed no significant difference (Fig. 3B). Although the expression of HGF peaked earlier on POD1 in the PH group and POD5 in the BD+PH group, there was no significant difference in the values (Fig. 3C).
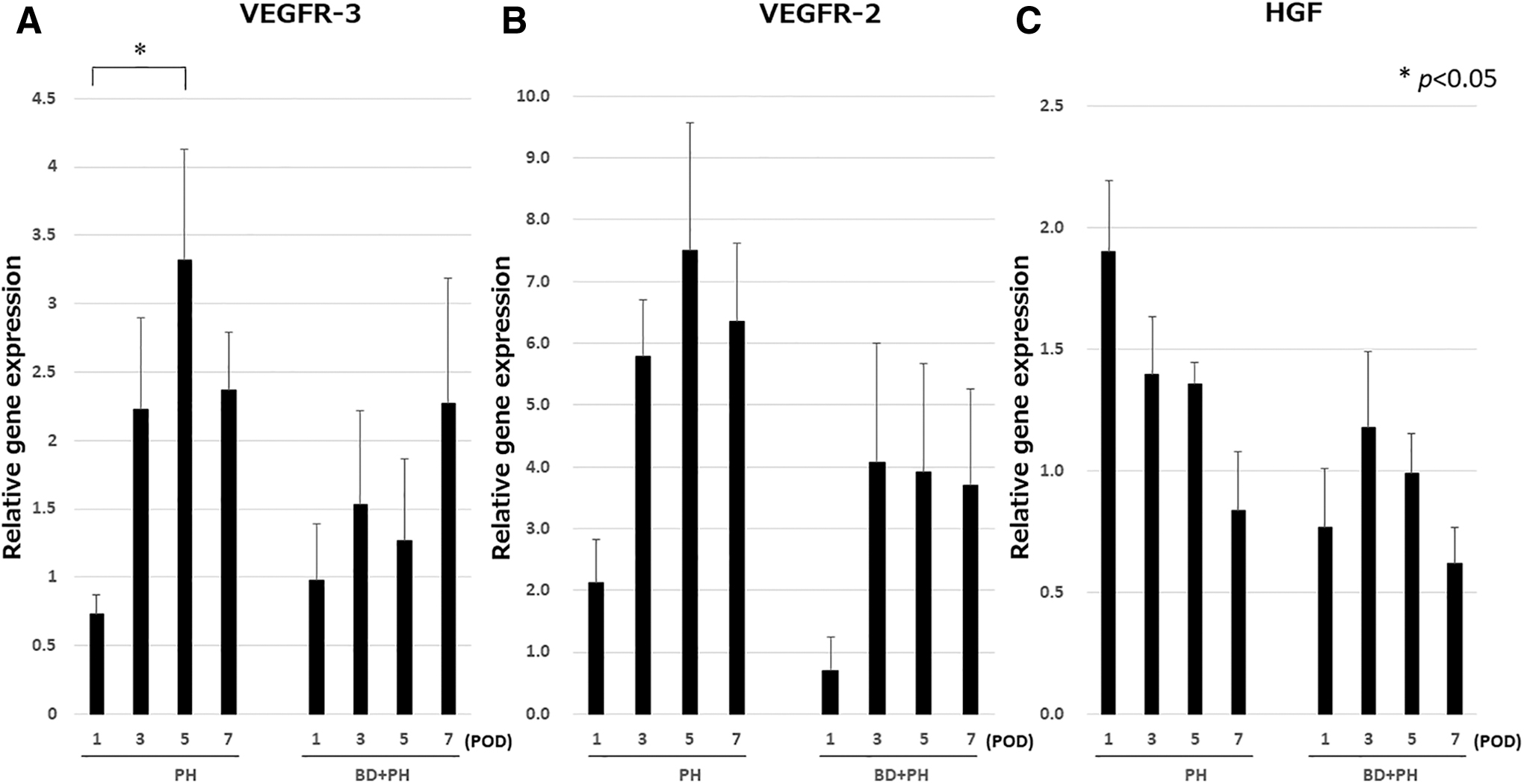
The results of the PCR. The mRNA expression of VEGFR-3
Discussion
The present study investigated the relationship between lymphangiogenesis and liver regeneration in cholestatic liver after partial hepatectomy. The results showed that the liver function of the cholestatic liver after partial hepatectomy was worse than that of the normal liver. In addition, we demonstrated that the liver regeneration and lymphangiogenesis of the cholestatic liver were delayed in comparison with the normal liver.
The liver could be considered a crucial organ for lymphatic fluid, because 25%–50% of lymph passing through the thoracic duct originates from the liver. 20 However, the lymphatic system in the liver has been unclarified, because the anatomy of the hepatic lymphatic system is complicated. 21 The hepatic lymphatic vessels are classified as portal, sublobular, and superficial. It is reported that more than 80% of hepatic lymph drains into the portal lymphatic vessels, while the remaining 20% drains through the sublobular and superficial lymphatic vessels. 22 In this study, the expression of LYVE-1 was observed around the portal lymphatic vessels and the distribution did not change during development or in response to injury.
This was the first study to investigate lymphangiogenesis and liver regeneration after partial hepatectomy in a model of liver cholestasis. Experimental common bile duct ligation is one method for establishing models of liver cholestasis. 19 At first, we performed partial hepatectomy on mouse models with common bile duct ligation; however, few of the mice could survive. Furthermore, in the clinical situations, ICC and other diseases are associated with improved postoperative cholestasis due to lesion resection and biliary tract reconstruction. For these reasons, temporary occlusion of the common bile duct was suitable for recapitulating the clinical situation. Oruc et al. reported a new technique of reversible common bile duct obstruction using a plastic cannula in rats 23 ; however, common bile duct of mice was too small to use the technique. Thus, we used a clip to occlude the common bile duct in our models of liver cholestasis. The level of T-Bil was approximately 10 mg/dL for 12 hours (data not shown). This method was easier to perform and results in a more precise representation of ICC treatment in the clinical setting.
Lymphangiogenesis was expected to proceed after hepatectomy; however, the term of activation has not been reported. This study showed that lymphangiogenesis after partial hepatectomy peaked on POD5 (Fig. 2B). Meanwhile, LYVE-1 was expressed not only in the lymphatic endothelial cells but also in the liver sinusoidal endothelial cells. Meng reported that the expression of LYVE-1 in liver sinusoidal endothelial cells gradually increased with time after partial hepatectomy in mice and peaked on POD5. 24 However, the LYVE-1 expression in liver sinusoidal endothelial cells is suggested to be diminished in the inflamed human livers. 25 Our study demonstrated that the expression of LYVE-1 in liver sinusoidal endothelial cells and lymphatic endothelial cells was similar.
The expression of VEGFR-3 was observed in cholangiocytes of normal rat livers and elevated in livers with cholestasis induced by bile duct ligation. 26 However, in this study, the expression of VEGFR-3 in the cholestatic and normal liver after hepatectomy did not differ to a statistically significant extent at various time points, because partial hepatectomy was performed and the cholestatic liver was induced by the temporary occlusion of the common bile duct with a clip. On the contrary, expression of VEGFR-3 gradually increased and peaked on POD5 in the normal liver group and on POD7 in the cholestatic liver group.
Liver regeneration and lymphangiogenesis involve a complicated process with various factors and signaling pathways. 15 Oikawa et al. hypothesized that lymph production increased due to increased portal pressure caused lymphangiogenesis. 27 Tanaka and Iwakiri reported that the extent and duration of lymphangiogenesis were determined by balances between lymphangiogenic factors and antilymphangiogenic factors. 21 Cao et al. showed that HGF, which is a representative liver regeneration factor, also acts, indirectly, as a lymphangiogenic factor. 28 On the contrary, the liver function and regenerative ability of cholestatic liver are greatly disturbed. 29 Yokoyama et al. reported that the mechanism responsible for impaired liver regeneration in cholestatic liver was due to decreased portal venous flow, attenuated production of liver proliferation-associated factors, increased hepatic apoptosis, and lack of enterohepatic circulation. 30 In this study, the expression of LYVE-1 and VEGFR-3 peaked on POD5 in the normal liver and on POD7 in the cholestatic liver. Delayed lymphangiogenesis in the cholestatic liver after hepatectomy was presumed to be caused by impaired regeneration due to inflammation of cholestasis, and decreased lymphangiogenic factors (e.g., FGF-1, FGF-2, and VEGF-C) that bind to the VEGFR-3 liver.
The present study was associated with several limitations. First, the induction of temporary common bile duct obstruction with a clip was the condition acute cholestasis. Thus, this study did not analyze chronic cholestasis. Second, although the BD+PH group required a second laparotomy to remove the clips, the PH group required only one laparotomy. Although the incidence of direct injury to the liver was the same in the two groups, it was unknown how laparotomy influenced the lymphangiogenesis of the liver. Third, we wanted to try to evaluate the expression of FGF-1, FGF-2, and VEGF-C/VEGF-D, but could not because we had used up the sample materials to assess VEGFR-3, VEGFR-2, and HGF.
In conclusion, partial hepatectomy in the cholestatic liver was highly invasive, had poor hepatic regenerative ability, and slower lymphangiogenesis. In the cholestatic liver, lymphangiogenesis after partial hepatectomy was delayed in comparison with the normal liver due to impaired liver regeneration and the late expression of VEGFR-3.
Footnotes
Acknowledgment
All authors agree with the content of the article and the submission.
Authors' Contributions
Conception and design: T.H., M.H., Y.S., and S.E.; acquisition or analysis of data: T.H, M.H., M.T., Y.S., H.Y., K.N., S.O., T.A., A.S., and S.E.; writing and revision of the article: T.H, M.H., M.T., Y.S., H.Y., K.N., S.O., T.A., A.S., and S.E.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was not funded by any educational or commercial organization.