
Abstract
Background:
The standard examination for diagnosing lymphedema is lymphoscintigraphy, which has a disadvantage in versatility and radiation exposure. We have reported the usefulness of echography in observing the lymphatic degeneration. The purpose of this study was to investigate the usefulness of lymphatic ultrasound in diagnosing lymphedema.
Methods and Results:
The study included 14 patients (28 lower limbs) who underwent lymphaticovenous anastomosis for lower limb lymphedema. Preoperative echography with a common 18-MHz linear probe was used to detect lymphatic vessels. We evaluated abnormal expansion or sclerosis of lymphatic vessels in the medial legs, which indicated the presence of lymphedema. We proposed the method “D-CUPS” on how to detect and observe the lymphatic vessels. We then performed indocyanine green (ICG) lymphography to diagnose lymphedema. The results of examination were compared. Stage 1 lymphedema was diagnosed in 9 limbs, Stage 2a in 7, Stage 2b in 8, and Stage 3 in 4. Lymphatic vessel detection was possible in all 28 medial thighs and in 27 medial lower legs. The sensitivity and specificity for diagnosis of lymphedema based on echography of the medial leg were 95.0% and 100.0%, respectively. The accuracy rate was 94.6%. We could detect lymphatic vessels with echography in 39 of 54 areas that failed detection using lymphoscintigraphy or ICG lymphography (72.2%).
Conclusion:
The location and degeneration of lymphatic vessels in lymphedematous limbs can be evaluated with a commonly used ultrasound device. Although exclusion of comorbidities is still necessary, lymphatic ultrasound has potential for use in diagnosis of lymphedema or lymphatic dysfunction.
Introduction
Standard diagnostic examination for lymphedema in the extremities includes lymphoscintigraphy or indocyanine green (ICG) lymphography.1–3 Lymphoscintigraphy is a relatively conventional procedure that can provide an image of the lymphatic vessels in the entire body. However, lymphoscintigraphy images are crude. ICG lymphography is a recently developed technique that can accurately detect lymphatic vessel locations. Moreover, the sensitivity for diagnosis of early-stage lymphedema is higher with ICG lymphography than with lymphoscintigraphy. 1 Both examinations are useful in diagnosing lymphedema, but are not widely available. In hospitals where lymphoscintigraphy or ICG lymphography is not available, lymphedema is diagnosed by clinical symptoms and a relevant history, such as pelvic lymph node dissection. 4 As lymphedema is progressive, early diagnosis and treatment are essential, especially in cases with lymphangiectasia,5–7 lymphorrhea, 8 lymphocysts, 9 or cellulitis.10,11
We previously reported the usefulness of echography in detecting lymphatic vessel and subcutaneous vein locations in preoperative examination for lymphaticovenous anastomosis (LVA).12–14 Echography can both accurately locate lymphatic vessels and determine the presence of lymphatic sclerosis. 15 Echography is also used for diagnosing varicose veins in the lower extremities.16,17 This minimally invasive technique valuable as it is available in most hospitals, and can evaluate valvular function in veins.
We theorized that lymphedema might be diagnosed using lymphatic vessel findings on echography. This would make it possible to diagnose lymphedema or presence of lymphatic dysfunction and would lead to early treatment. In this study, we used lymphatic ultrasound before LVA and diagnosed lymphedema according to the degeneration of the lymphatic vessels observed in echography. The aim of this study was to elucidate the usefulness of echography in diagnosing lymphedema.
Materials and Methods
The institutional ethics committee approved the study and written informed consent was obtained from each patient (approval number: 30-8).
We investigated 28 legs of 14 patients with lower limb lymphedema who underwent echography before LVA in March 2019.
Lymphatic ultrasound
Echography was performed by a single experienced lymphatic surgeon on the day before surgery. The surgeon was blinded to the findings of prior outpatient lymphoscintigraphy. Echography was performed with a linear probe that is commonly used for venous evaluation (Noblus EUP-L65; Hitachi Medical Corp., Tokyo, Japan). Depth was set at 2 cm at a frequency of 18 MHz. As the lymphatic vessels in the lower extremities are on the medial side and along the great saphenous vein (GSV), 18 we searched an area from 5 cm anterior to 5 cm posterior to the GSV. The probe was placed orthogonal to the GSV to observe cross-sectional images of the lymphatic vessels.
The lymphatic vessels can be seen as paired, short, parallel hyperechoic lines, ∼0.2 mm apart, resembling an equals symbol (Fig. 1a, b). These short lines indicate the superficial and deep walls of the cross-sectional image of a lymphatic vessel. The lymphatic vessels can be distinguished from fibrotic tissue because they are continuous when traced to proximal and distal ends. Vessels that are dilated due to lymphatic stasis appear on echography as hypoechoic circles, ∼0.5–1.5 mm in diameter (Fig. 1c, d). In more advanced cases, the lymphatic vessels become sclerotic and appear as hyperechoic circles, with or without a hypoechoic circle at the center, measuring ∼0.5 mm in diameter (Fig. 1e, f). This indicates a sclerotic and thickened wall and a narrowed lumen.
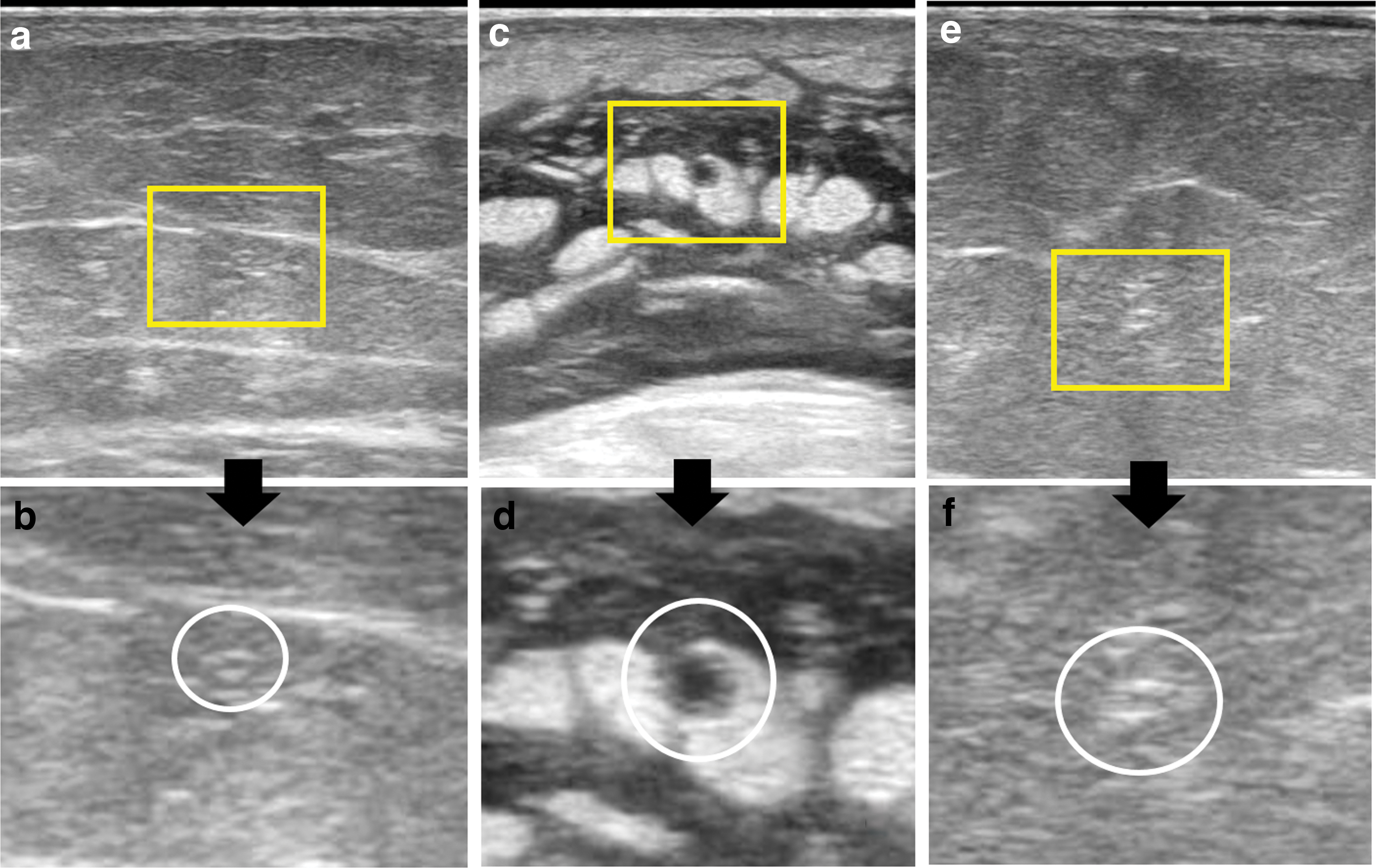
Ultrasonographic findings of lymphatic vessels.
Lymphatic vessels are sometimes difficult to distinguish from veins on echography. We established five indexes (“D-CUPS”) to discriminate the two vessels as follows. As “Doppler” images are sometimes falsely negative because the small veins are not colored, the “CUPS” indexes are more important.
Doppler: Lymphatic vessels are rarely colored with Doppler mode because they contract once in 30–60 seconds (Supplementary Movie S1). In contrast, subcutaneous veins are usually colored with Doppler.
Cross: Lymphatic vessels do not connect with subcutaneous veins, but instead cross past the veins when traced proximally; the veins usually connect with larger veins (Supplementary Movie S2).
Uncollapsible: The lymphatic vessels are less collapsible under probe pressure than the veins because the inner pressure of lymphatic vessels in limbs with lymphedema is higher than in veins.
Parallel: Two lymphatic vessels sometimes run parallel and adhere without connecting (Fig. 2). Subcutaneous veins connect and gradually enlarge in diameter.
Superficial fascia: Collecting lymphatic vessels run horizontally beneath superficial fascia. In contrast, subcutaneous veins run above the superficial fascia and sometimes travel obliquely across adipose tissue to the GSV.
Using these indexes, we evaluated lymphatic vessel degeneration (dilation or sclerosis) in the thigh and lower leg, respectively, and labeled affected locations using a permanent marker that could not be visualized with an infrared camera. We diagnosed lymphedema when dilated or sclerotic lymphatic vessels were identified. When lymphatic vessels could not be identified in the medial legs, we evaluated the lateral lymphosome and degeneration in the lymphatic vessels and used the findings as a reference.19,20 We also evaluated accumulation of lymphatic fluid in subcutaneous tissue.
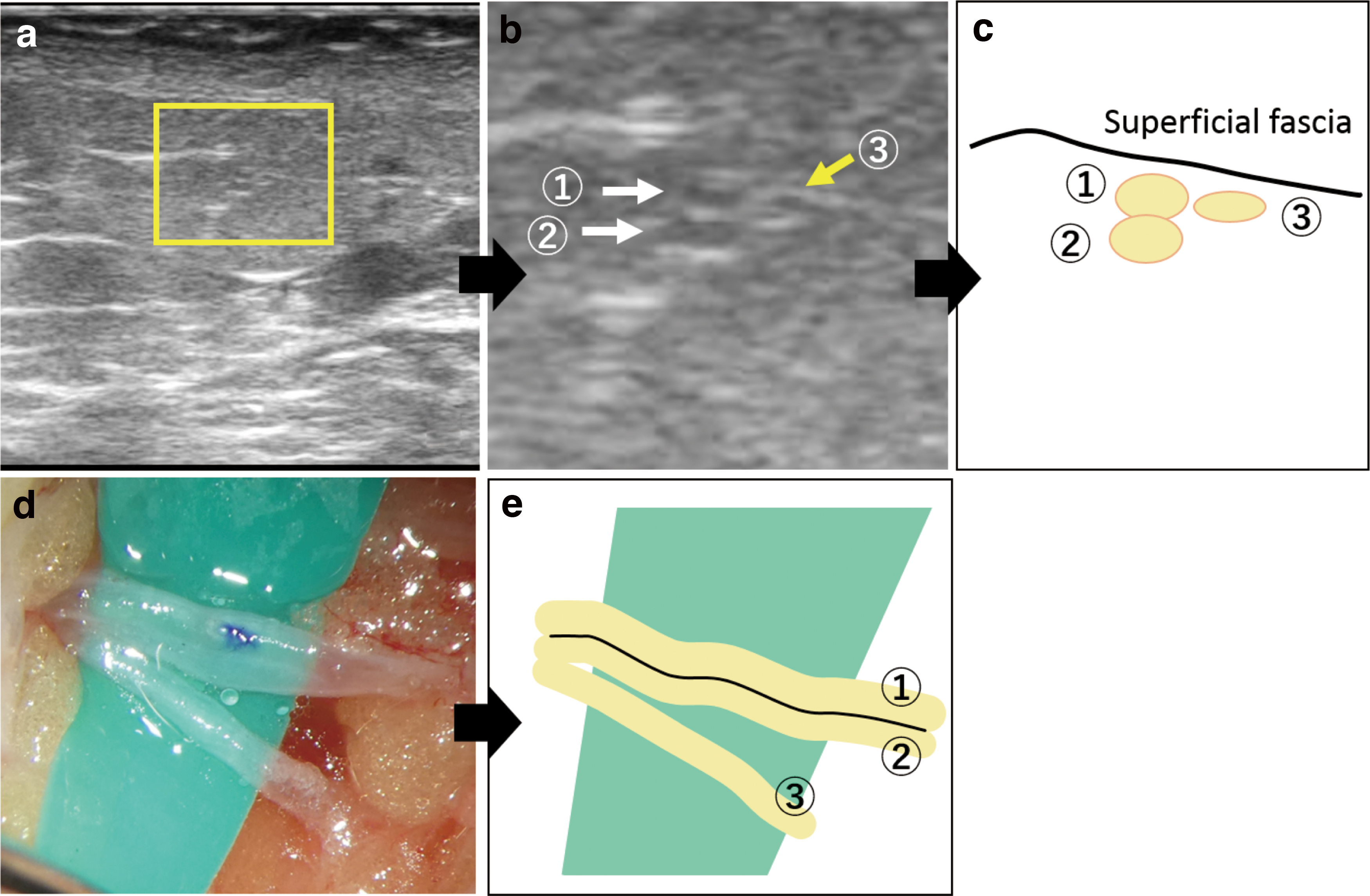
Two lymphatic vessels (#1, #2) run in parallel and adhere without connecting; #3 is another lymphatic vessel running nearby.
ICG lymphography
Next, we performed lymphography by injecting ICG in three lymphosomes per limb and assessed the findings using a near-infrared camera. 19 In brief, we injected 0.05 mL of ICG (0.5% Diagnogreen; Daiichi Pharmaceutical, Tokyo, Japan) into the first web space of the foot, proximal to the lateral condyle, as well as lateral to the superior edge of the knee. Shortly after injection, we observed the lymphogram with an infrared camera (Photodynamic Eye; Hamamatsu Photonics, Hamamatsu, Japan), and marked the location of lymphatic vessels in a linear pattern. We again used the infrared camera on the following day to determine the presence and extent of dermal backflow. Lymphedema was diagnosed when dermal backflow was present.
Lymphoscintigraphy
We performed lymphoscintigraphy to determine the severity of lymphedema using 150 MBq of 99mTc-labeled albumin radioisotope injected into the bilateral first web spaces. Scintigrams were recorded at 15, 30, 60, and 90 minutes after injection. Images obtained 60 minutes after injection were classified using the Maegawa classification. 3
Statistics
We compared lymphatic ultrasound and ICG lymphography results for the thigh and lower leg separately, and calculated the sensitivity and specificity for diagnosing lymphedema.
Results
All participants were females with secondary lymphedema and average age of 59.7 years (range: 48–84 years). The cause of lymphedema was uterine cancer in 13 patients and ovarian cancer in 1. Based on the International Society of Lymphology criteria, Stage 1 disease was present in 9 limbs, Stage 2a in 7, Stage 2b in 8, and Stage 3 in 4. Using lymphoscintigraphy findings, Type 1 images were observed in 9 limbs, Type 2 in 4, Type 3 in 5, Type 4 in 9, and Type 5 in 1.
Lymphatic vessel detection was possible in all 28 medial thighs and in 27 medial lower legs. The sensitivity for lymphedema diagnosis was 95.0%, with specificity of 100.0% (Table 1). The overall accuracy was 94.6%, with 96.4% in the thigh and 92.9% in the lower leg.
Comparison of the Result Between Lymphatic Ultrasound and Indocyanine Green Lymphography in Diagnosis of Lymphedema
Sensitivity and specificity of lymphatic ultrasound in diagnosing lymphedema were 95.0% and 100.0%, respectively, with 94.6% accuracy.
ICG, indocyanine green.
Lymphatic vessels could not be detected in the medial lower leg in one case, but dilated vessels on the lateral side were detected, enabling diagnosis of lymphedema. In a case in which results were falsely negative in the thigh, we observed normal lymphatic vessels in the medial thigh but could not detect lymphatic vessels in the lateral thigh. It was difficult to diagnose lymphedema with echography in this case, even in retrospect. In contrast, in a case in which results were falsely negative in the lower leg, we observed normal lymphatic vessels in the medial lower leg but dilated lymphatic vessels on the lateral side, and diagnosed lymphedema retrospectively.
In comparing the results of echographic detection of lymphatic fluid accumulation in subcutaneous tissue with the results of ICG lymphography for the diagnosis of lymphedema, the sensitivity was 42.5%, with specificity of 93.8% (Table 2) and accuracy of 57.1%.
Comparison of the Result Between Ultrasonographic Assessment of Lymphatic Fluid Accumulation in Subcutaneous Tissue and Indocyanine Green Lymphography in Diagnosis of Lymphedema
Sensitivity and specificity of ultrasonography, detecting subcutaneous edema, in diagnosing lymphedema were 42.5% and 93.8%, respectively, with 57.1% accuracy.
The lower limb was separated into four areas (medial thigh, lateral thigh, medial lower leg, and lateral lower leg) and scanned for lymphatic vessels. Among 54 areas in which no lymphatic vessels were observed on lymphoscintigraphy or ICG lymphography, we detected dilated lymphatic vessels in 39 cases (72.2%) and were able to perform LVA.
Discussion
This report demonstrated the usefulness of lymphatic ultrasound in evaluation of lymphatic degeneration and diagnosis of lymphedema. The sensitivity and specificity for diagnosis of lymphedema were 95% and 100%, respectively, suggesting that diagnosis was possible with lymphatic ultrasound.
Lymphoscintigraphy is a standard method used for diagnosing lymphedema, and is useful in evaluating lymphatic function and lymph accumulation. However, the images are crude and cannot identify individual lymphatic vessels. Therefore, lymphoscintigraphy is inadequate for evaluation before LVA. Moreover, not all hospitals or clinics have scintigraphy equipment and radiation exposure is also a concern.1,3
ICG lymphography provides more detailed image of lymphatic vessels and is suitable for preoperative examination for LVA.1,2,21 The sensitivity is also higher than that of lymphoscintigraphy. However, only superficial vessels within 1–2 cm from the skin surface can be observed with ICG lymphography. Moreover, patients with iodine allergy cannot undergo ICG.
Magnetic resonance lymphography, bioimpedance spectroscopy, and tissue dielectric constant measurement have recently been used to diagnose lymphedema.21,22
Although each technique has merits and demerits, the equipment required for these examinations is not available in every hospital or clinic, especially those not specialized for treatment of lymphedema.
This study used lymphatic ultrasound to diagnose lymphedema and demonstrated high accuracy. Ultrasound is commonly used in many medical facilities and the technique is the same as that for ultrasonography of leg veins. Hayashi et al. reported the use of ultrahigh-frequency ultrasound (70 MHz) to observe the lymphatic vessels.22–24 It is especially useful in observing the superficial layer, although the device is special and not equipped in every hospital. In this study, no special equipment, probe, or contrast agent is required. The examination is painless and allergy is not a concern. Lymphatic ultrasound can be introduced as a standard examination for diagnosing the presence of lymphatic dysfunction, and can help to diagnose lymphedema.
An advantage of lymphatic ultrasound is the ability to evaluate lymphatic degeneration. ICG lymphography, lymphoscintigraphy, and other diagnostic techniques can detect lymph accumulation or dermal backflow in lymphatic vessels, but cannot evaluate lymphatic dilation or sclerosis. Even lymphatic vessels with a linear appearance on ICG lymphography are sometimes dilated or sclerotic. 25 Lymphatic ultrasound can observe degeneration in individual lymphatic vessels and can be considered an important technique, especially as the preoperative evaluation of the surgical treatment for lymphedema.26–28
In lower limb venous echography, the probe is placed parallel to the longitudinal axis of the leg to evaluate blood flow or reflux. 29 It may also be possible to evaluate lymphatic flow or reflux in diagnosing lymphedema. However, the diameter of lymphatic vessels is ∼0.2–1.5 mm and the long axis view may be difficult to observe. Moreover, the lymphatic vessels in lymphedematous limbs sometimes run in a spiral pattern, making observation difficult. In future, improved observation capability may be possible using super-high-frequency ultrasound.
In conclusion, lymphedema could be diagnosed with lymphatic ultrasound. The sensitivity and specificity in diagnosing lymphedema were 95% and 100%, respectively. In addition, lymphatic ultrasound is useful in preoperative evaluation. In this study, detection of lymphatic vessels was possible in 72.2% of areas where none were observed on ICG lymphography and ICG lymphography. Although exclusion of comorbidities is still necessary, lymphatic ultrasound has potential for use in diagnosis of lymphedema or lymphatic dysfunction.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.