
Abstract
Background:
The Lymphedema Functioning, Disability, and Health questionnaire for Upper Limb Lymphedema (Lymph-ICF-UL) is a health-related quality-of-life questionnaire for patients with breast cancer-related lymphedema. Previous testing of this questionnaire showed very good psychometric properties; however, responsiveness has not yet been established. The aim of this study was to determine its internal and external responsiveness.
Methods and Results:
Ninety-five patients treated with decongestive lymphatic therapy in a longitudinal trial were recruited. Patients completed the Lymph-ICF-UL twice within a time interval of 7 weeks (“intensive group” receiving intensive treatment; n = 73) or 3 months (“stable group” receiving maintenance treatment; n = 22), and once the Global Perceived Effect (GPE) questionnaire at the second time point. The significance of change in scores and standardized response mean (SRM) were determined for the total and domain scores. Correlations between Lymph-ICF-UL and GPE were ascertained. In addition, the minimal clinical important difference (MCID) was determined. The Lymph-ICF-UL total score changed significantly in the intensive group (p < 0.001) and nonsignificantly for those in the stable group (p = 0.25). The SRM represented moderate responsiveness (0.65). Patients who reported a clinical improvement ( = responders) after intensive treatment showed a significant decrease in total score (p < 0.001), this was also the case for nonresponders (p < 0.001). Lymph-ICF-UL total and domain scores showed nonsignificant weak correlations with the GPE (p > 0.05). There was a significant difference in mean total score changes between responders and nonresponders (p < 0.001). MCID for the total score was 9%.
Conclusion:
The Lymph-ICF-UL is responsive to change after decongestive lymphatic therapy. No correlations were found between Lymph-ICF-UL change scores and GPE. Future studies should be conducted in a clinical setting, with more variability between participants and their treatment responses.
Introduction
Lymphedema is a troublesome morbidity affecting ∼17% of the women treated for breast cancer. 1 The edema can be measured objectively with different valid and reliable assessment methods (water displacement, circumference measurements, etc.). 2 However, an objective assessment of the volume lacks the power to encounter the real burden of lymphedema.
Besides swelling, patients can suffer from problems in physical, social, and mental functioning.3,4 In addition, breast cancer-related lymphedema (BCRL) lowers the quality of life.5,6 Therefore, the Lymphedema Functioning, Disability, and Health questionnaire for the upper limb (Lymph-ICF-UL) was developed to assess these impairments. 7 This questionnaire aims to quantify impairments in function, activity limitations, and participation restrictions that are related to upper limb lymphedema. In contrast to other lymphedema-related questionnaires, it is based on the terminology of the International Classification of Functioning, Disability and Health (ICF) of the World Health Organization (WHO). 8
The quality and usefulness of a questionnaire are determined by its psychometric properties, including validity, reliability, and responsiveness. The reliability and validity of the Lymph-ICF-UL have already been examined in patients with BCRL and showed very good (reliability) to good (validity) psychometric parameters.7,9 However, responsiveness of the Lymph-ICF-UL has yet to be ascertained.
Therefore, the aim of this study was to examine the internal and external responsiveness of the Lymph-ICF-UL in patients with BCRL.
Materials and Methods
Study design
Participants of the EFforT-BCRL trial 10 were recruited in the University Hospitals of Leuven, Antwerp University Hospital, Ghent University Hospital and General Hospital Groeninge in Kortrijk, Belgium. Approval for this study was obtained by the Ethical Committee of the University Hospitals of Leuven (main Ethical Committee), as well as of the ethical committees of all other participating centers (CME reference S58689, EudraCT Number 2015-004822-33). This study was reported following the COSMIN (COnsenus-based Standards for the selection of health Measurement INstruments) guidelines. 11
Participants
Female patients with BCRL of the arm and/or hand, who were about to start the intensive phase of decongestive lymphatic therapy through participation in the EFforT-BCRL trial ( = intensive group), or participants who were at least 3 months in the trial's maintenance phase of this study ( = stable group), were recruited. Criteria for inclusion and exclusion are presented in Table 1. Note that no formal power analysis has been performed, but that the sample size was completely determined by the response rate of the ongoing EFforT-BCRL trial. 10
Inclusion and Exclusion Criteria
BCRL, breast cancer-related lymphedema.
Study procedure
This study was conducted between March 2016 and October 2018. All patients provided written informed consent before treatment. Descriptive data (participant's age, body mass index, type of breast surgery, side of surgery, hand dominance, type of adjuvant treatment (radiotherapy, chemotherapy, hormone therapy, or immunotherapy), duration, and stage of lymphedema) were collected by interviewing the participants and by consulting their medical record.
Figure 1 shows the study procedure. Patients were asked to complete the Lymph-ICF-UL questionnaire before the start of the intensive treatment phase (intensive group) or at the beginning of month 3 of their maintenance phase (stable group). In addition, the volume of each of the participants' arms was determined by circumference measurements using a perimeter after which the total arm volume was calculated using the truncated cone formula.12,13
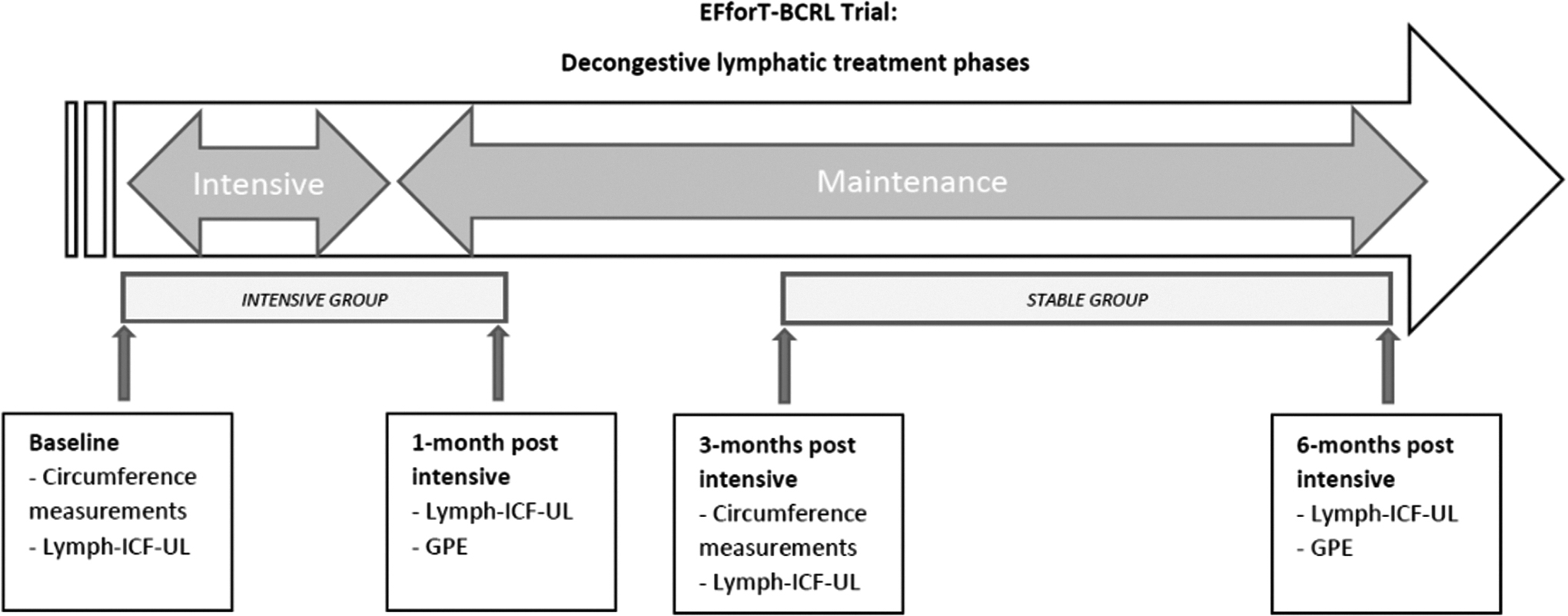
Illustration of the study procedure.
The intensive treatment lasted for 3 weeks and consisted of all components of the decongestive lymphatic therapy, as recommended in the consensus document of the International Society of Lymphedema (ISL): manual lymph drainage, skin care, exercises, and multilayer bandaging. When the volume of the arm was decreased optimally and pitting was absent, a compression stocking and glove were measured. When patients received the compression garment, the 6 months lasting maintenance phase started, consisting of: manual lymph drainage, skin care, exercises, and wearing the compression garment.10,14
The second time point for data collection was performed 4 weeks after wearing the stocking (intensive group) in order patients could get used to the feeling of wearing a stocking and/or gauntlet, or at the end of month 6 of their maintenance phase (stable group). Again, this second evaluation consisted of completing the Lymph-ICF-UL questionnaire, this time together with the Global Perceived Effect (GPE) questionnaire (Fig. 1).
All treatments and assessments were provided at the Department of Physical Medicine and Rehabilitation of the University Hospitals of Leuven, at the Multidisciplinary Breast Clinic of the Antwerp University Hospital, at the Departments of Plastic Surgery and Radiotherapy of the Ghent University Hospital, and at the Centre for Oncology at the General Hospital Groeninge in Kortrijk. Measurements were performed by one of three physical therapists, specialized in edema therapy (S.V.D.B., L.V., and T.D.V.) who were blinded for the treatment allocation of patients. Treatments were performed by one of four physical therapists, specialized in edema therapy (L.B., R.V.H., L.V., T.D.V.).
Outcome variables
Following questionnaires and measurements were used.
Lymphedema Functioning, Disability, and Health Questionnaire for upper limb lymphedema7,9
The Lymph-ICF-UL is a self-reported comprehensive evaluation tool assessing impairments in functioning, activity limitations, and participation restrictions in patients with BCRL during a 2-week recall period. It consists of 29 questions, covering five domains: physical function, mental function, household activities, mobility activities, and life and social activities. Each of the questions has to be scored on an 11-point Likert scale with a score between 0 and 10. The total score on the Lymph-ICF-UL and the scores on the five domains range between 0 and 100. The higher the score, the more problems patients experience. Reliability and content validity have shown to be very good; construct validity is good.7,9
GPE questionnaire
The reference criterion used in this study to investigate external responsiveness was the GPE scale. 15 The GPE is a patient-reported outcome measure stating the amount of improvement as perceived by the patient. The following question was asked to the patients of the intensive group: “To what extent did you recover from your lymphedema-related symptoms and complaints since the beginning of the treatment?” Alternatively, to the patients of the stable group, the following question was asked: “To what extent have your lymphedema-related symptoms and complaints (what you feel, can perform,..etc) changed compared to the previous evaluation moment within the EFforT-BCRL study? This means: we want to know the degree of change in your complaints, only between ……(date previous assessment) and ……(today) (not in comparison with the period before your participation in the study).”
It measures the perception of the patient with use of an ordinal scale. A 7-point Likert scale ranging from (1) very much better, (2) much better, (3) a little better, (4) unchanged, (5) a little worse, (6) much worse to (7) very much worse was used, as recommended by Ostelo. 16 Literature shows that scores 1 and 2 can be considered as a clinically relevant improvement, 17 whereas a score of 3 (a little better) should be considered as unchanged as this reflects a minimum degree of improvement that could be experienced in patients just by being treated with attention for the current health-related problems.16,18 Consequently, patients scoring the GPE with 1 or 2 (very much better to much better) are further referred to as “responders,” whereas patients scoring the GPE with scores 3, 4, 5, 6, or 7 (a little better to very much worse) are further referred to as “nonresponders.”16,19–22 The GPE proved to have an excellent reproducibility.[23]
Investigation of responsiveness
There is no consensus on how responsiveness of measures should be quantified and it is further complicated by the multiple definitions that are used. 24 In general, literature suggests that there are two major facets of responsiveness: internal and external responsiveness. Internal responsiveness characterizes the ability of a measure to show changes within a particular period of time. 24 The observed changes in the measures are attributed to clinically relevant changes in health. 24 Consequently, the internal responsiveness of a measure will depend upon the particular treatment that is provided to patients as well as the specific outcomes that are described to determine treatment efficacy. 24
In addition, external responsiveness reflects the extent to which changes in a measure over a particular period of time relate to corresponding changes in an external reference measure of a person's health status. 24 In this type of responsiveness, the measure itself is not of primary interest, but the relationship between change in the measure and change in the external standard. 24 In contrast to internal responsiveness, the external responsiveness of a measure will solely depend on the choice of the external reference measure and not on the investigated treatment. 24
To investigate the internal and external responsiveness of the Lymph-ICF-UL, we were interested in the following topics for which we had formulated subsequent hypotheses:
Internal responsiveness
Whether or not the Lymph-ICF-UL could demonstrate a statistically significant change in scores before and after the intensive treatment phase.
Hypothesis 1: In the intensive group, there would be a statistically significant change in mean total scores of the Lymph-ICF-UL between the two evaluation moments (p < 0.05).
Whether or not the Lymph-ICF-UL could demonstrate a statistically significant change in scores before and after the 3 months of maintenance treatments.
Hypothesis 2: In the stable group, there would be no statistically significant difference in mean total scores of the Lymph-ICF-UL between the two evaluation moments (p > 0.05).
Whether or not the Lymph-ICF-UL is able to show a relatively small level of variability in change scores in relation to the average change in scores between the two evaluation moments, by means of the standardized response mean (SRM) as an effect size.
Hypothesis 3: The calculated SRM values reflecting the variability of the change scores of the Lymph-ICF-UL would represent moderate (≥0.50) to large (≥0.80) responsiveness for the Lymph-ICF-UL total score. 24
External responsiveness
Whether the Lymph-ICF-UL could demonstrate a statistically significant change in scores before and after intensive therapy in the responders on the one hand and in the nonresponders on the other hand. In addition whether the Lymph-ICF-UL could demonstrate a statistically significant difference in mean change score between responders and nonresponders after intensive treatments.
Hypothesis 4: The change in mean Lymph-ICF-UL total score before and after intensive treatment would be statistically significantly different between responders and nonresponders (p < 0.05).
Whether the Lymph-ICF-UL would show a correlation between the change in scores (before and after intensive/maintenance treatments) and the GPE.
Hypothesis 5: There would be at least a moderate correlation (≥0.3) between the change in mean Lymph-ICF-UL scores (of both the intensive and the stable group together) and the score on the GPE.
The minimal clinical important difference (MCID) of the Lymph-ICF-UL.
Hypothesis 6: The MCID for responders on the total score of the Lymph-ICF-UL would be <10 (10%).
Statistical analyses and interpretation
Data analyses were performed using the Statistical Package for Social Sciences 25 for Windows (SPSS, Inc., Chicago, IL). Normality of the variables was tested using the One-Sample Kolmogorov–Smirnov test and descriptive statistics were calculated. The 0.05 level of significance was applied.
Data are presented as number and percentage for categorical variables and mean with standard deviation (SD) (normal distribution) or median with interquartile range (non-normal distribution) for continuous variables, unless otherwise stated.
Considering the investigation of internal responsiveness, the following statistical tests were performed:
Wilcoxon-signed-rank tests were used to determine whether the Lymph-ICF-UL total and domain scores were significantly different before and after the intensive treatment phase. Also to determine whether the Lymph-ICF-UL total and domain scores were significantly different between the two evaluation moments during the maintenance phase, the Wilcoxon-signed-rank tests were performed. The SRM as effect size was calculated for the responsive group using the following formula
24
:
Considering the investigation of external responsiveness, the following statistical tests were performed:
Wilcoxon-signed-rank tests were used to determine whether the Lymph-ICF-UL total and domain scores were significantly different before and after the intensive phase of treatment in the responders and nonresponders group separately. Comparability of the group responders and nonresponders was tested with Mann–Whitney-U for numeric data and with chi-square for categorical data. In addition, to investigate significant differences in the mean change in scores between responders and nonresponders before and after intensive therapy, a two-way analysis of variance (ANOVA) for repeated measures statistic was applied.
Spearman's rho correlation analysis was performed on the entire group (both the intensive and stable groups) to determine the correlation between the change in Lymph-ICF-UL scores and the reported GPE. According to Cohen, the correlations required values of 0.3 or higher to be regarded as a good anchor.28,29
The MCID represents the smallest change in score that the participant perceives as a meaningful improvement. 30 If a participant's score is above the MCID, it is considered clinically relevant. To define the MCID, the mean change scores on the Lymph-ICF-UL of the participants who reported an important clinically important improvement (responders scoring the GPE with 2, i.e., “much better”) were used. 30 Consequently, to investigate the MCID, descriptive statistics were used to describe the mean (±SD) of the total and domain scores corresponding to the responders of the entire group (both the intensive and stable groups).
Results
In this study, 95 participants were recruited. Of these, 73 participants were enrolled in the intensive group and 22 participants in the stable group. The mean age of the participants was 62 (±10) years and mean body mass index was 29 (±6) kg/m2. In the intensive group (n = 73), the mean absolute difference in lymphedema volume of the arm was 541 (±481) mL. In the stable group (n = 22), the mean absolute difference in lymphedema volume of the arm was 384 (±282) mL. The characteristics of the participants are presented in Table 2.
Characteristics of the Participants (n = 95)
BCRL stages as described by the International Society of Lymphology; descriptive statistics are depicted as mean (SD).
SD, standard deviation.
Internal responsiveness
Change in Lymph-ICF-UL scores after treatment: intensive group
The mean pre- and postintensive treatment scores of the Lymph-ICF-UL are given in Table 3.
Mean Pre- and Posttreatment Scores of the Lymph-ICF-UL in Both the Intensive and Stable Group
p-value <0.05, **p-value <0.01.
Lymph-ICF-UL, Lymphedema Functioning, Disability, and Health questionnaire for the upper limb.
A statistically significant difference (p < 0.05) was present in the intensive group between the pre- and postintensive treatment total scores of the Lymph-ICF-UL as well as in all domain scores, except for the mobility activities domain (p = 0.06).
Change in Lymph-ICF-UL scores after treatment: stable group
The mean pre- and postmaintenance treatment scores of the Lymph-ICF-UL are presented in Table 3. There was no statistically significant difference in total nor domain scores between the two assessments (p > 0.05).
Effect size: SRM
SRM values are presented in Table 4. The effect size of the total score represented moderate responsiveness (0.65). Highest SRM value is shown in the physical functions domain (0.99), representing good responsiveness. Lowest value was for the mobility activities domain, showing small responsiveness (0.21).
Standardized Response Means Calculated for the Intensive Group (n = 73)
SRM, standardized response mean.
External responsiveness
Difference in pre- and postintensive treatment scores for responders and nonresponders
Table 5 presents an overview of the mean total and domain scores of the Lymph-ICF-UL before and after intensive treatment, as well as the mean change scores before and after intensive treatment for/between responders and nonresponders. Responders (n = 39) showed a statistically significant decrease in the Lymph-ICF-UL total score, physical function, mental function, and mobility activities domain scores over time (p < 0.05). Other domains were not significantly different before and after intensive treatment. Nonresponders (n = 34) showed a statistically significant decrease in the Lymph-ICF-UL total score, physical function, mental function, and household activities domain scores (p < 0.05).
Separate Mean Pre- and Posttreatment Scores of Lymph-ICF-UL for Responders and Nonresponders and the Mean Change in Scores Before and After Intensive Treatment Between Responders and Nonresponders
p-value <0.05, **p-value <0.01.
ANOVA, analysis of variance.
Preintensive treatment scores on the Lymph-ICF-UL were significantly different in both groups for the total score (p = 0.02) as for the domains physical function (p = 0.01), household activities (p = 0.08), and life and social activities (p = 0.04) domain scores of the Lymph-ICF-UL, in which the nonresponders showed relatively more problems in functioning at baseline compared with the responders.
The mean change in scores before and after intensive treatment was significantly different between responders and nonresponders for the total score (p < 0.001), physical function (p < 0.001), mental function (p < 0.001), household activities (p = 0.01), and life and social activities (p = 0.03) scores (Table 5).
Correlations between change scores and GPE
Correlations between changes in scores of the Lymph-ICF-UL (Δ-Lymph-ICF-UL) and the GPE scores are given in Table 6. The scores of all the 95 participants were used. The Lymph-ICF-UL total score as well as the physical functions, mental functions, household activities, and mobility activities domains showed nonsignificant weak positive correlations with the GPE.
Spearman's Rho Correlations Between Change Scores of Lymph-ICF and Global Perceived Effect Scores (n = 95)
ΔLymph-ICF-UL, mean change of scores of Lymph Functioning, Disability, and Health questionnaire for upper limb lymphedema.
MCID in Lymph-ICF-UL score
An overview of the MCIDs (SDs) associated with the Lymph-ICF-UL total and domain scores is provided in Table 7. The MCID estimate for the Lymph-ICF-UL total score was 9%, physical function 14%, mental function 7%, household activities 8%, mobility activities 6%, and life and social activities 5%.
Overview of the Minimal Clinical Important Differences (Standard Deviations) of the Lymph-ICF-UL Scores According to the Different Scores on the Global Perceived Effect (n = 95)
Scores are depicted as mean (SD).
MCID, minimal clinical important difference.
Discussion
The aim of this study was to investigate the responsiveness of the Lymph-ICF-UL questionnaire.
As an answer to the methodological inconsistencies in the literature regarding responsiveness, the COSMIN panel reached consensus on the definitions of measurement properties for health-related patient-reported outcomes in an international Delphi study. 31 A checklist was developed to determine the methodological quality of studies on measurement properties.32,33 The definition of responsiveness according to the COSMIN initiative is “the ability of a health-related patient reported outcome instrument to detect change over time in the construct to be measured.” 31 In this study, this was translated to the ability of the Lymph-ICF-UL to detect a clinically important change in number of problems in functioning of patients with BCRL, as part of the external responsiveness of the questionnaire.
Results showed that, in this study, only one out of the six hypotheses regarding the internal and external responsiveness was rejected. All three hypotheses regarding internal responsiveness (hypotheses 1–3) were accepted. There was a statistically significant difference in the intensive group between the pre- and postintensive treatment total scores of the Lymph-ICF-UL as well as in all domain scores, except for the mobility activities domain (Hypothesis 1). A reason for this might be that restrictions in mobility activities can be influenced by other factors as well, besides BCRL. Furthermore, there was no statistically significant difference in total nor domain scores between the two evaluation moments in the maintenance phase (Hypothesis 2). Finally, the effect size of the total score represented moderate responsiveness (SRM 0.65), suggesting that the questionnaire is able to indicate a clinically meaningful change in total score 24 (Hypothesis 3).
Regarding external responsiveness, 2 out of 3 hypotheses (hypotheses 4 and 6) were accepted. We expected that there would be a statistically significant difference between the change in total score of the responders and nonresponders, which was confirmed by this study (Hypothesis 4). Only for the mobility activities domain, this change score was nonsignificantly different.
Responders showed a statistically significant decrease in total score as well as in most of the domain scores of the Lymph-ICF-UL after the intensive treatments. However, surprisingly this was also the case for nonresponders. Whereas our analyses revealed that the nonresponders showed a relatively higher level of problems in functioning at baseline than the responders. Consequently, in patients with a higher number of problems in functioning at baseline, a relatively greater improvement in functioning after treatment can be expected.
Furthermore, when correlating the change scores of the Lymph-ICF-UL with the reported GPE, we expected at least moderate correlations (Hypothesis 5). However, results revealed mainly nonsignificant weak positive correlations. Therefore, this hypothesis could not be accepted. A major drawback for this correlation analysis was the relatively under-representation of patients who reported to be deteriorated after their treatment. Whereas, while designing this study, we decided to include also a subgroup of patients who were currently at the end of the maintenance phase (the stable group) as an attempt to encounter this and to include also patients who might have been deteriorated. Nevertheless, results indicated that, of the entire group, only 4% reported to be worse, 16% reported to be unchanged, 33% reported to have a little bit improved, and 47% reported to have improved (much or very much better). Consequently, the majority of participants reported to be improved or unchanged, resulting in a rather homogeneous study sample. Other authors have discussed the use of GPE as an anchor as it might be very dependent on the status of a patient and, therefore, it might be more a measure of the patient's status than of the change in health status over time.23,34
Lastly, we hypothesized that the MCID for responders on the total score of the Lymph-ICF-UL would be <10 (10%) (Hypothesis 6), which was an arbitrary chosen cutoff point based on empirical experience. As the total score of the Lymph-ICF-UL represented an MCID of 9%, our last hypothesis could be accepted as well. This result entails that if this total score decreases with at least 9 on 100, an overall clinical improvement will be experienced. This MCID exceeds the earlier reported standard error of measurement of 5, thereby eliminating the possibility that the change in score could be due to any measurement error. 9 Consequently, the reported limitation that the MCID does not take measurement precision into account 35 is partially compensated this way.
Limitations and strengths
A strength of this study is that, in the investigation on responsiveness, the recommendations of the COSMIN panel were taken into account. An integrated system making use of multiple methods to define internal and external anchor-based responsiveness was applied.
Some limitations should be considered. First, as this investigation was conducted on a cohort of participants of the EFforT-BCRL trial, patient characteristics, protocol, and treatment outcomes were rather homogeneous as the majority of the participants indicated to have improved or not to have changed, which might have induced a selection bias. There was a lack of participants who reported a deterioration (only 4 out of 95 participants), which was a shortcoming for the purpose of this investigation.
Second, the moment of completion of the questionnaires was for each patient at the end of a 1-hour clinical assessment. This could have entailed an influence on patient's motivation and concentration level to spend some extra time and effort on reading every question with full attention. For this reason, we might suspect that some interpretation errors of the scoring system could have occurred (for instance when the anchors “very well” and “not at all” were converted in some questions but was not noticed by the participant). However, this was explained in advance. Last, as completion of the questionnaires occurred at the end of fixed evaluation moments in accordance with the EFforT-trials' protocol, the time in-between the two evaluations was different for the intensive group (7 weeks) as for the stable group (3 months). However, we believe this has not affected our study results.
Implications for clinical practice
The Lymph-ICF-UL questionnaire already proved to be appropriate and useful in clinical practice by showing very good reliability (intraclass correlation coefficients between 0.79 and 0.95 and Cronbach alpha coefficients higher than 0.80), very good face and content validity, and good construct validity (79% of accepted hypotheses regarding convergent/divergent validity). 9 This study reveals that the Lymph-ICF-UL is sensitive to detect changes over time. A change of 9% in total score indicates a clinically relevant change in the number of problems in functioning, of a patient with BCRL. A change of 14% in the physical function domain score designates a clinically relevant change in the number of problems regarding physical functions. Furthermore, a change of 7% in the mental function domain score indicates a clinically relevant change in the number of problems regarding mental functions. In the household activities domain, a change of 8% describes a clinically relevant change in the number of problems regarding household activities. Likewise, in the mobility activities domain, a change of 6% indicates a clinically relevant change in the number of problems regarding mobility activities. Lastly, in the life and social activities domain, a change of 5% indicates a clinically relevant change in the number of participation problems.
Recommendations for future research
When correlating the Lymph-ICF-UL scores with the GPE, the questionnaire showed a reduced ability to discriminate between the number of changes in Lymph-ICF-UL scores and the actual clinical improvement as reported by participants. As in our opinion, this is mainly due to the strict protocol in which this investigation occurred, a future investigation should be continued in a clinical setting, resulting in more variability between the study participants and consequently in their treatment responses. Furthermore, attention should be paid on the moment of completion of the questionnaires in order patients to be fully concentrated.
Conclusion
This study revealed that the Lymph-ICF-UL questionnaire is responsive to change after decongestive lymphatic therapy, in patients with BCRL. Based on the GPE as anchor-based method, an MCID of 9% indicates a clinically relevant change. No correlation between Lymph-ICF-UL change scores and GPE was found. Future studies should be conducted in a clinical setting, enabling a greater amount of variability between the study participants and treatment responses.
Footnotes
Acknowledgments
The authors are very grateful to the hospitals collaborating in this study. The authors also extend grateful thanks to the study participants, to Lien Billiet, Roxane Van Hemelrijck, and Lore Vos for performing the treatments and to Shanah Van den Bosch and Lore Vos for measuring and handing over the questionnaires to the study participants. All authors critically revised the article for important intellectual content and approved the final article. A.D.G. is a postdoctoral research fellow of the FWO-Flanders.
Clinical Trial Registration Number
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is financed by the Agency for Innovation by Science and Technology, Applied Biomedical Research (IWT 150178). To arrange such financing, a separate collaboration agreement has been signed by the KU Leuven and the beneficiaries.