
Abstract
Background:
The axillary web syndrome (AWS) occurs in the axilla and on the frontal side of the upper arm and sometimes along the forearm to the thumb. The cord is painful, particularly on movement, and can therefore be very distressing for the patient. Although the phenomenon has been examined and discussed for decades, no evidence for the origin has been found until now. The aim of this study was to perform a histopathologic analysis of cords taken between 1996 and 1998 in the Surgical Clinic, Skane University Hospital, Lund, Sweden.
Methods and Results:
In seven patients, biopsies of the AWS cords were obtained 4–5 weeks after axillary node surgery for breast cancer and examined with standard hematoxylin and eosin and D2–40 (lymphatic endothelial cell) staining. In one biopsy, there was a dilated vessel with a thickened wall, which was confirmed by D2–40 immunostaining to represent a lymphatic vessel. The lumen was occluded by organized thrombus, within which new vessels were being formed, indicating recanalization. In two other biopsies, similar lymphatic vessels with thickened walls were present, although the lumen of the vessels was not visualized in the planes of the section. The other four biopsies do not show specific features.
Conclusion:
Although only one case, this is the first pathological evidence of thrombosis within a confirmed lymphatic vessel from a case of cording. We propose that the axillary cord represents lymphatic vessel thrombosis. Recanalization of the thrombus may eventually restore lymphatic flow consistent with the transient nature of the condition.
Introduction
The axillary web syndrome (AWS), otherwise known as axillary cording or lymphatic cording, is a common occurrence after breast cancer treatment, but its pathophysiology has not been understood. Here, we present evidence that it is of lymphatic origin and likely due to lymphatic thrombosis.
The phenomenon can be visible in the axilla as soon as 2 weeks after axillary node dissection, usually for cancer. Although predominantly observed in the axilla, the cords can often be seen or palpated on the medial side of the upper arm and may extend down into the forearm turning laterally toward the thumb. Cords, such as violin strings, are aligned in the direction of the neurovascular bundle. Tension on the cords through abduction of the arm induces pain and the cords can be seen bowstringing across the axilla and so lifting the overlying skin, hence the term axillary web syndrome.
The pain can limit the range of motion (ROM) of the shoulder. In a prospective, longitudinal study by Johansson et al., 1 cords could be palpated in 77% of cases 1 month after axillary node dissection. The shoulder ROM was reduced in 66% and 43%, at examination 1 and 2 months postsurgery, respectively. However, at 3 months postsurgery, the frequency for reduced ROM had decreased to 3%. This means that the axillary cord is a minor problem in the long term. However, the reduced shoulder ROM and the pain by movement can be very distressing to the patient and may also cause problems with positioning of the arm for radiotherapy. Management varies from manual snapping of the cords to leaving alone for natural resolution. Symptoms can persist for 6 months or more. 2 Doubt remains if AWS can predispose to lymphedema. 3
If the cause of the cord could be determined, a proper treatment could be suggested as, at the moment, many different approaches are applied, often with contradictory background theories.
In a systematic review, Yeung et al. 4 found that biopsies had identified venous or lymphatic pathology, but discrimination between the two vessels was often not possible.1,5–7 Thrombosis of a presumed lymphatic vessel was reported in three studies,5–7 where identification of the type of involved vessel was based only on morphology. Lymphatic endothelial antibodies for lymphatic identity now exist making distinction between small veins and lymphatics possible. 8 Here we report on findings in seven specimens of cording using standard hematoxylin and eosin histopathology and immunocytochemistry to determine the lymphatic origin of the cord.
Materials and Methods
Patients
Biopsies from seven patients with axillary cord were taken between 1996 and 1998. At that time, it had not been possible to distinguish clearly between veins and lymphatic vessels and the results showed a mixture of features. 1 The seven patients with AWS included six females and one male treated for breast cancer (Table 1).
Characteristics of Seven Patients with Axillary Cord Following Axillary Node Dissection Due to Breast Cancer
Volume difference between the arms with no adjustment for dominance.
Increased thickness of the subcutaneous tissue palpated at the medial side of the upper arm.
Patients were informed about the biopsy procedure and gave their oral permission that was noted in their records. Ethical approval was obtained (Dnr 2016/501) with approved amendment for further sections to be cut and stained from the original tissue blocks, 2018-03-26, from the Regional Ethics Review Board, Lund University, Sweden. The archived tissues imbedded in paraffin blocks were requested from Region Skåne Biobank, Department of Clinical Genetics and Pathology, Skåne County, after permission from the Regional Biobank Centrum South Sweden. The tissue biopsy samples were transferred for analysis at the St George's Hospital, London, United Kingdom, after approval from the Swedish Biobank Centrum South Sweden.
Procedure
Four to 5 weeks postbreast cancer surgery and with the patient in a supine position, passive abduction of the shoulder on the operated side was measured with a goniometer. The ROM was expressed in degrees as recommended by the American Academy of Orthopedic Surgeons. 9 Once the cords were identified by palpation, a local anesthetic was infiltrated. Through a 2-cm-long cut over the hard, palpable cord, 1–2 cm of the cord were ligated and taken out with some connective tissue around the cord. The biopsies were fixed in formalin and embedded in paraffin at the Clinical Pathology Unit, Lund, Sweden, according to the clinical standards of tissue processing.
Fixation time of the tissue cannot be exactly reported as fixation time varied depending on tissue type, variable transfer time to the pathology unit, and processing method. Tissues embedded in paraffin and archived in biobanks at room temperature shrink and dry out with the passage of time.
Immunohistochemistry
Formalin-fixed paraffin-embedded tissue blocks were cut on a Leica RM 2250 microtome. The tissue was cut at 3-μm-thickness (Leica microtome No. 2255) slides. The slides were pretreated using heat-induced antigen retrieval with high pH (EnVision FLEX Target Retrieval Solution, K8010; Dako, Glostrup, Denmark) in a Dako pretreatment module. Immunohistochemical stainings were carried out in a Dako Autostainer Plus (DakoCytomation, Glostrup, Denmark).
Endogenous peroxidase activity was blocked with 0.3% hydrogen peroxide for 10 minutes. The slide sections were then incubated for 1 hour with rabbit polyclonal antibodies directed against Prox1 (1:300, ab38692; Abcam, Cambridge, United Kingdom) or mouse monoclonal antibodies against Ki-67 (1:300, M7240; Dako). Staining was visualized using polymer/horseradish peroxidase (HRP)-linked secondary antibodies (K8010; Dako) and 3,3′-diaminobenzidine chromogen (brown-colored product, SK-4100; Vector Laboratories, Burlingame, CA). Next, the slide sections were treated with a denaturating solution kit (DNS001L; Biocare Medical, Concord, CA) for 5 minutes to prevent additional binding to the first primary antibody.10,11 The slide sections were then incubated for 1 hour with mouse monoclonal antibodies against D2–40 (1:25, CM266; Biocare Medical), and staining was visualized using polymer/HRP-linked secondary antibodies (K8010) and Vina Green chromogen (green-colored product, BRR807AS; Biocare Medical). Finally, the nuclei were stained blue with Mayer's hematoxylin, and slide sections were air-dried and mounted with Pertex (Histolab® Cat. No. 00840).
Results
Demographic and clinical data for the seven patients can be found in Table 1.
Histopathologic analysis
The biopsy from patient 7 shows a dilated large caliber vessel with thickened fibrotic wall. The lumen is partly occluded by thrombosis, which is undergoing organization and recanalization with angiogenesis. The endothelial cells in the vessel stain positively with D2–40 (Fig. 1). The biopsies from cases 5 and 6, each also shows part of a vessel with thickened fibrotic wall, similar to case 7. However, thrombosis was not seen in the lumen of case 5. In case 6, the plane of section did not include the lumen. The biopsies from the other four cases show fibroadipose tissue without evidence of a dilated large caliber vessel with thickened fibrotic wall, as is present in the other three cases.
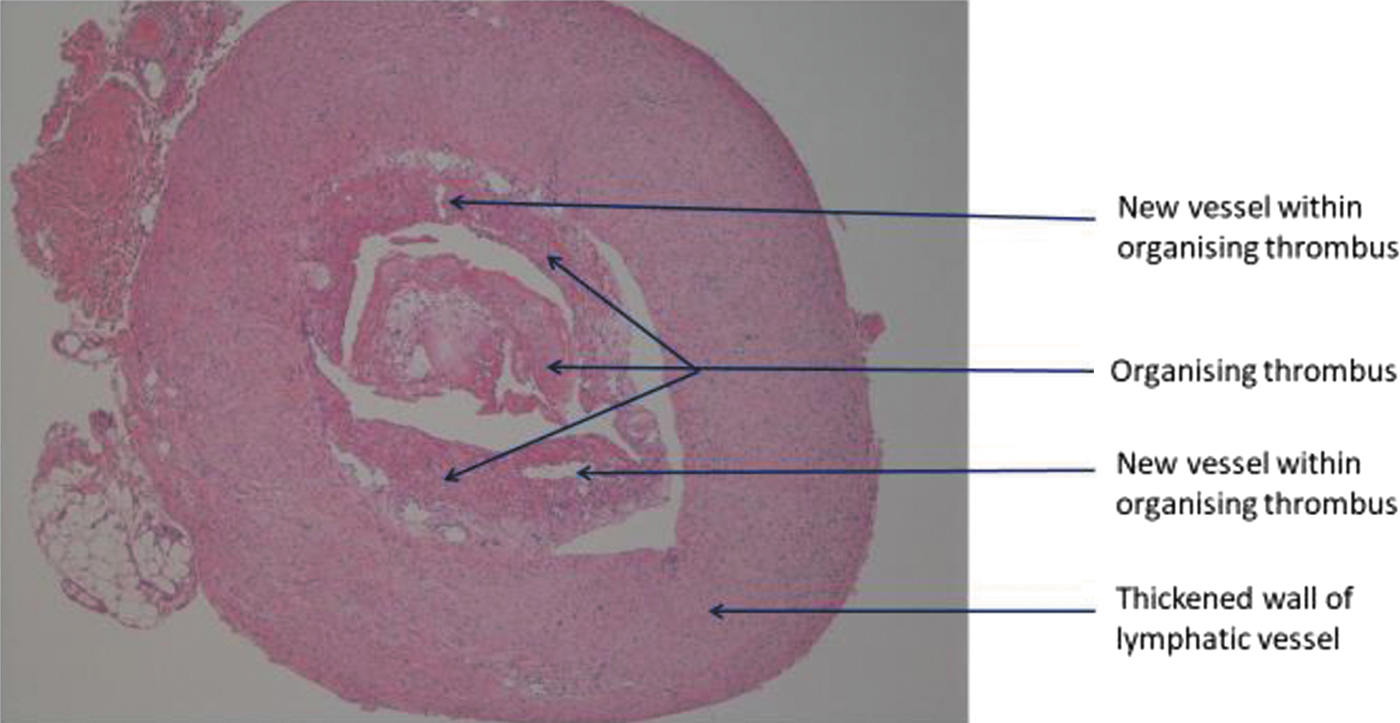
Thrombosis of a thickened lymphatic vessel. Color images are available online.
Discussion
This represents the first report where an axillary cord is demonstrated conclusively by immunohistochemistry to be caused by a thrombosed lymphatic vessel. The biopsies examined in this study were originally examined by standard cellular pathology at the time they were taken between 1996 and 1998, but results were considered to represent venous thrombosis. The surgeon's comments at the time were that the cords had the appearance and texture of inflammatory vein/phlebitis, a bit thick and similar to patients' varices he had operated through the years.
In one of our cases (case 7), we demonstrate that the axillary cord is represented by a dilated lymphatic vessel with a thickened fibrotic wall and occlusion by thrombosis. The lymphatic nature of the vessel is confirmed by immunohistochemical staining with D2–40. Our findings are very much in line with previous reports that have indicated thrombotic occlusion of a lymphatic vessel, although these other studies did not include confirmation of the lymphatic nature of the vessel by immunohistochemical staining. Thus, it could not be categorically concluded that the vessels were lymphatic vessels.5–7 Our findings are also in keeping with a case report 12 where D2–40 immunohistochemistry confirmed a thickened lymphatic vessel as the cause of the axillary cord. Unusually, in this case, the cord developed following a furuncle, rather than the usual sequela of axillary surgery for breast cancer. In this case, however, there is no thrombotic occlusion of the vessel.
Two of our other cases each showed a large vessel identified as lymphatic with thickened walls, although thrombotic occlusion was not evident. The sections of the other four cases revealed fibroadipose tissue without a similar large vessel with thickened wall. In our original study from 2001, vessels, identified morphologically at that time as veins, were present in six of the cases. 1 Based on the current reanalysis, the vessels are now regarded as thickened lymphatic vessels. The slide sections from the original study have been discarded. Instead, in the current study, newly cut slide sections were examined from the same tissues preserved in the original paraffin blocks. This factor most likely accounts for the apparently discrepant finding of a vessel in only three cases rather than the original six. It is most probable that the material containing the vessel in the other three cases has been cut out from the tissue paraffin block and is therefore not represented in the newly cut sections.
Understanding the pathogenesis of AWS has eluded investigators. It is a reasonable hypothesis that the cording represents lymphatic thrombosis because (a) the phenomenon occurs after severance of lymphatic vessels and (b) lymph does clot. 13 Other pathogenic explanations could include a change in the fascia or venous thrombosis, but ultrasound examination failed to identify any structures consistent with either explanation. 14 The ability to snap the cords is consistent with a thrombosed vessel. The triad of Virchow describes the concept of thrombus formation as being the result of one or more of the following broad pathological changes: disruption in flow, endothelial damage, and hypercoagulability. Axillary node surgery can clearly account for disruption and stasis in lymphatic flow and damage to lymphatic vessels.
The finding of thrombotic occlusion of the dilated lymphatic vessel with recanalization of the organized thrombus by angiogenesis corresponds to the transient nature of the axillary cord. The cord resolves as the vessel gradually recanalizes. This agrees with the natural history of AWS, showing a reduction of symptoms and normalization of ROM within 3 months postoperatively.1,15 Thus, the patients with an axillary cord should be reassured and informed that this condition will improve, even without treatment.
Conclusion
Although only one case, this is the first pathological evidence of thrombosis within a confirmed lymphatic vessel from a case of cording. We propose that AWS represents lymphatic vessel thrombosis. Recanalization of the thrombus and its resolution are consistent with the transient nature of the condition.
Footnotes
Acknowledgment
The authors thank Professor Christian Ingvar, Lund University, who took out the biopsies between 1996 and 1998.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by grants from the Swedish Cancer Foundation.