
Abstract
Background:
Bioimpedance spectroscopy (BIS) is a tool that can be used to measure body composition in a variety of populations. Previous studies have investigated novel applications to utilize BIS to measure localized body composition, including in the hand. According to BIS guidelines, there should be no skin wounds at the site of electrodes, and that electrode positions may be modified in specific circumstances, as our group has validated previously in burn wound populations.
Methods and Results:
To determine in noninjured participants, whether BIS measurements recorded using alternate electrode positions on the palm of the hand and forearm, or a combination of electrodes on the dorsum and volar surface of the hand and forearm, were comparable with electrode positions on the dorsum of the hand and forearm. The study demonstrated that drive and sense electrodes on the palm of the hand and volar forearm, and a combination of electrodes on the palm of the hand and dorsum of the forearm, resulted in comparable measures of impedance of extracellular water (difference from reference position: 1.26%–4.75%, p = 0.411–0.558) and total water (difference from reference: 2.15%–2.40%, p = 0.258–0.781). Electrodes on the dorsum of the hand and volar forearm resulted in significantly different measures for the same BIS variables (percentage difference range 4.66%–6.15%, p < 0.001–0.003).
Conclusion:
Electrode positions on the palm of the hand and volar forearm, or on the palm of the hand and dorsum of the forearm, are interchangeable as clinical measures of hand lymphedema and total water impedance.
Introduction
Edema is the accumulation of excess fluid, predominantly in the extracellular space, due to an imbalance in the rate of extravasation and subsequent return to the systemic circulation. 1 This is caused by an imbalance of effective capillary pressure, an obstruction to the venous or lymphatic flow by trauma or surgery, or by muscle weakness or paralysis in an extremity placed in a dependent position.2,3 Lymphedema is an increase in protein concentration in addition to an increase in extracellular fluid, which results in tissue composition in the skin and subcutaneous tissues, 4 resulting from dysfunction of the lymphatic system, either from congenital abnormality or secondary to treatments, such as those associated with cancer. 5 Excessive protein-rich fluid in the hand will disperse between structures, including joint capsules, tendons and tendon sheaths, and fascial layers, 6 resulting in rapid organization of proteinaceous fluid, which may result in loss of hand function and deformity through tissue fibrosis causing structural thickening, adherence, and loss of elasticity.6–8
The clinical measurement of hand volumes has historically been performed using circumferential or figure of eight measures using a tape measure, or the use of water displacement. 1 Figure of eight measures has been shown to be reliable and valid in both noninjured and hand burn injury populations.9,10 However, this technique only provides a linear representation of the limb volume rather than a physiological measure. In that, volume measures are estimated based on calculations, and the measures, although highly associated, are not interchangeable or interpretable with physical or physiological volume measurements, nor can the measure be extrapolated between subjects. 11
Water displacement volumetry, which utilizes the Archimedes' principle of water displacement, is recognized as the “gold standard” for measuring hand volumes in clinical populations. 12 However, volumetry may be challenging in hands with open wounds with respect to infection control practices, and dressings may confound accurate volume measures. 13 Repeat measures of hands in the clinical setting provide a quantification of a change in lymphedema, and the effect of interventions for its management.14,15 However, water displacement has several drawbacks when considering its clinical application and feasibility, as it is a time-consuming process that requires a correct apparatus setup, 9 and requires patient cooperation and compliance.
While these measures of hand volume are reliable and valid in a variety of noninjured and patient populations, they are reflective of overall volumes and may not be sensitive enough to detect lymphedema, or changes in lymphedema volumes, in the clinical setting.16,17 Responding to and changing lymphedema volumes are a vital role of clinicians. Similarly, responding to acute episodes of edema, such as in patients postburn injury or following other trauma, has an impact on the patient's outcome. Clinical assessment of a swollen hand involves observing the hand for loss of skin creases at the joints, and accumulation of fluid beneath the dorsal skin. 18 However, accurate measures of hand volumes for research are often difficult to obtain. 16
Bioimpedance spectroscopy (BIS) is a noninvasive physiological measure of body composition and has the potential to measure body composition in the clinical setting. 19 The impedance to the flow of a small alternating current through the tissues is measured to provide immediate assessment of fluid volumes in the body. BIS uses multiple frequencies of current to enable the extrapolation of frequencies at zero hertz (R 0 ), which is representative of the impedance specific to the volume of extracellular water (ECW) in the tissues, and infinite frequency (R ∞ ) that is associated with total body water (TBW). The BIS algorithms estimate volumes of total and compartmental fluid, using Cole/Cole modeling.20,21 The measured impedance of the intracellular component of the tissues is R i .
The use of BIS to measure hand volumes has been investigated in both normal and lymphedema populations. BIS was shown to be more sensitive than three-dimensional scanning (perometry) to changes in hand volume elicited by a postural change for a period of 3 minutes in a healthy population,22,23 and is more sensitive in discriminating women with lymphedema than scanning method volume measures. 22 Fluid volumes in the body are based on the formula of an equivalent cylinder, and include coefficients for the length of the body segment and the resistivity of the body fluid. 24
The guidelines for the measurement of BIS state that there should be no lesions at the site of the electrodes, and should wounds be present, then the site of the electrodes should be changed. 25 Broader application of the BIS technique in clinical practice is afforded by the research to date, which addresses this issue and confirms novel electrode configurations that provide interpretable BIS measures.26,27 The use of alternate electrode positions for the measurement of limb segment and whole-body BIS has been examined in noninjured and burn wound populations.26,27 These studies confirmed that whole-body and upper limb segmental BIS measures are equivalent to standard electrode positions in both populations with alternate hand electrode positions and standard foot positions. Localized BIS measures have been shown to be reliable and more sensitive than traditional circumferential measures in detecting volume change in a number of studies,28,29 and that alternate electrode positions can be used to assess localized impedance of tissues in a variety of clinically applicable configurations. 30
The location of wounds on the dorsum of the hand commonly precludes the use of standard electrode configurations for measuring hand BIS. The aim of this study was therefore to determine whether BIS measurements recorded using alternate electrode positions on the palm of the hand and forearm, or a combination of electrodes on the dorsum and volar surface of the hand and forearm, were interchangeable with electrode positions on the dorsum of the hand and forearm.
Materials and Methods
Subjects
A sample of convenience was recruited from staff and students at Fiona Stanley Hospital. Participants were between the ages of 18 and 65 years, with a body mass index (BMI) within 15–40 kg·m−2. Subjects were excluded from participating based on contraindications according to the manufacturer's specifications, including pregnant or breastfeeding participants, and subjects with implantable surgical devices including cardiac pacemakers and/or electronic life support devices. Human Research and Ethics Committee approval from The University of Notre Dame Australia (015158F) was received for the project, and the project was registered with the South Metropolitan Health Service Governance, Evidence, Knowledge and Outcomes System (GEKO) as a Quality Improvement project (10830) as required when health staff are approached for recruitment.
Instrumentation
Bioimpedance measures were recorded using the ImpediMed SFB7 (ImpediMed Ltd, Brisbane, Australia) multifrequency bioelectrical impedance analyzer. The SFB7 uses a single-channel tetra-polar configuration, and BIS measures are performed at 256 discrete frequencies from 4 to 1000 kHz. The SFB7 records impedance measures in triplicate, with each measure 1 second apart. The electrodes used were Ag/AgCl Eurotrode PFR2034 disposable resting ECG tab electrodes (reference code 12774; Pirrone srl, Milan, Italy).
Procedures
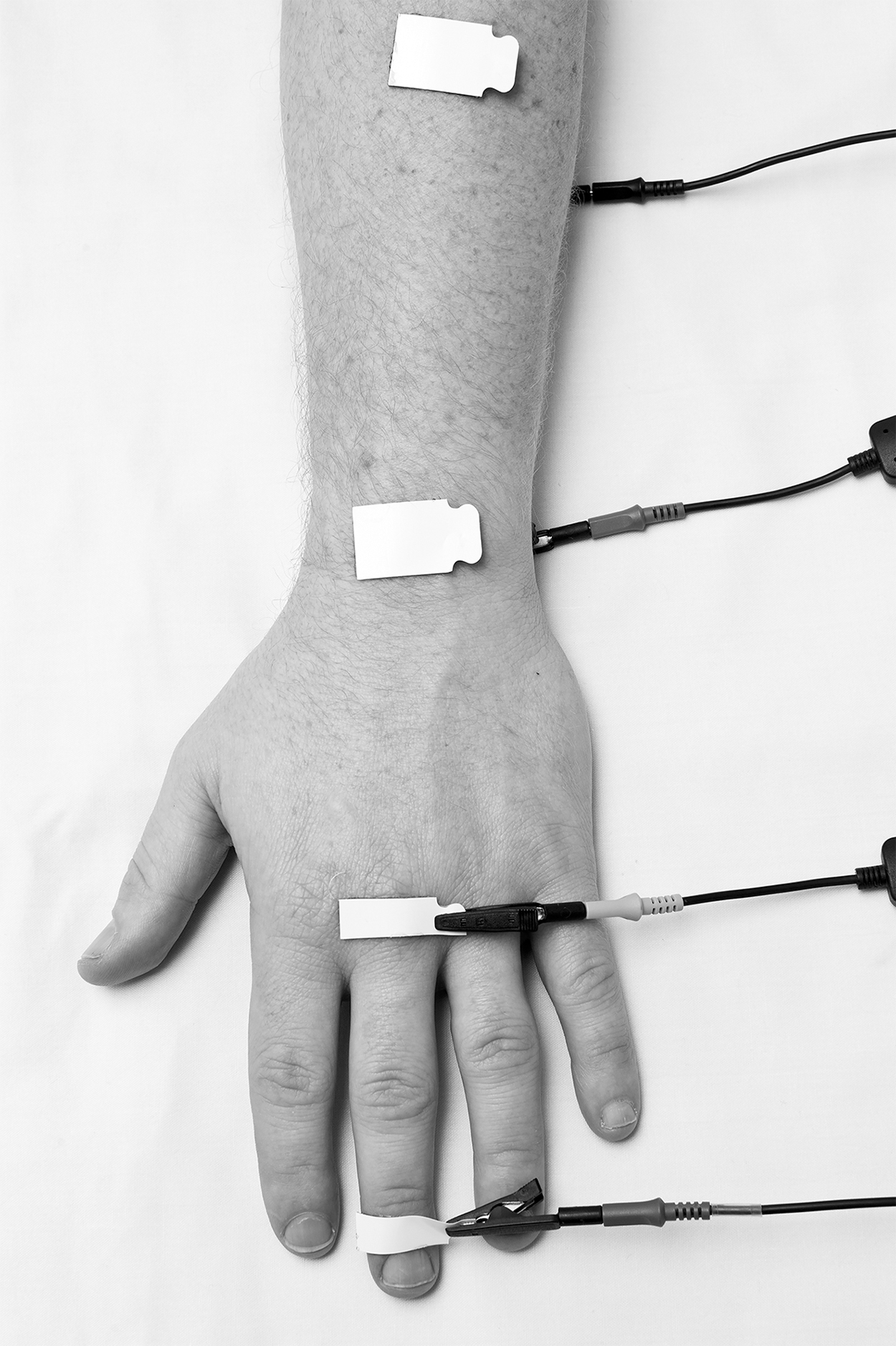
Before the assessment of BIS, participant height, weight, and age were recorded, as the software for the SFB7 device requires this information to calculate body composition. Measurement of hand volumes using BIS was previously described with four electrode positions on the dorsum of the hand and forearm (Position 1—Fig. 1). 23 The current injection (or drive) electrode is positioned on the dorsum of the distal phalanx of the middle finger, below the level of the nail bed. The distal current sense electrode is at the level of the third metacarpophalangeal joint, and the proximal current sense electrode is on the wrist at the level of the ulnar styloid. The proximal current drive electrode is positioned at midforearm level, measured as the distance between the olecranon and the ulnar styloid. The distance between the sense electrodes was measured using a nonstretch tape measure.

Electrode Position 1 (reference position).
Three alternate electrode positions were investigated to determine whether these alternate positions resulted in BIS measures equivalent to Position 1.
Position 2 (Fig. 2) placed the distal current drive and sense electrodes on the dorsum of the hand, and the proximal current sense and drive electrode on the volar surface of the wrist and forearm. Electrode Position 3 (Fig. 3) was the reverse of this, with the distal current drive and sense electrodes placed on the volar surface of the middle finger and hand, and the proximal current sense and drive electrodes placed on the dorsum of the wrist and forearm.
Electrode Position 2.

Electrode Position 3.
Position 4 (Fig. 4) placed the electrodes on the volar surface of the hand and forearm. Distal current drive electrode was on the volar surface of the middle finger distal phalanx. The distal current sense electrode was the palmar surface of the hand in line with the third metacarpophalangeal joint. The proximal current sense electrode was placed on the volar surface of the wrist in line with the ulnar styloid, and the proximal current drive electrode was placed on the volar midforearm.
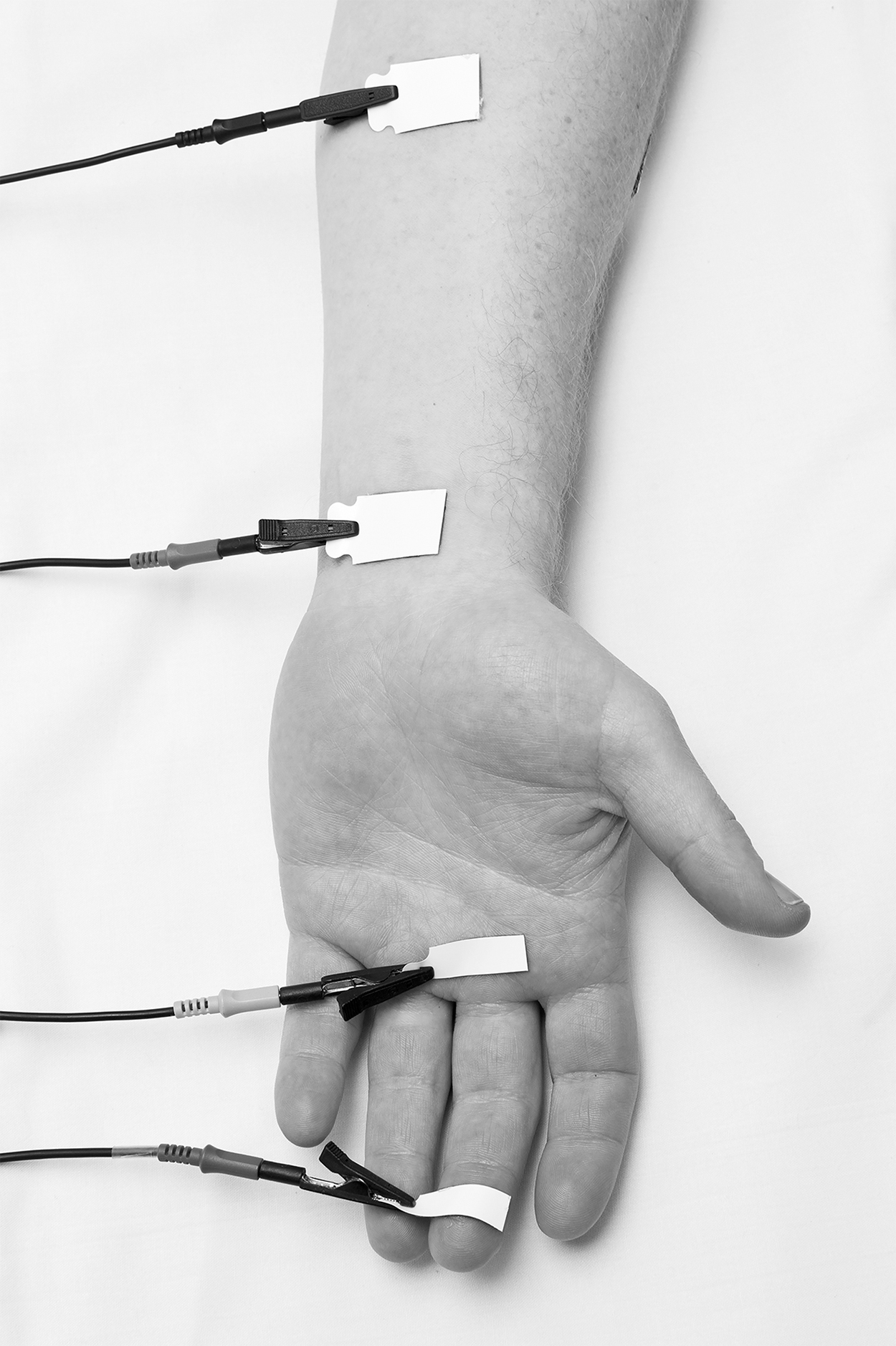
Electrode Position 4.
BIS measures were recorded with the participants lying supine, with their hands resting by their sides, arms abducted so that their hands were away from the body, and their legs separated. Before application of the electrodes, the skin surfaces were cleaned using alcohol swabs. Where the sense electrodes were on the same side of the hand and wrist, the distance between the closest edges of the sense electrodes was measured using a tape measure, that is, between the proximal edge of the distal sense electrode and the distal edge of the proximal sense electrode.
Two different methods were used to assess the distance between the electrodes where the sense electrodes were on opposite sides of the hand (in Positions 2 and 3). The first method recorded a diagonal linear measure of the distance between the electrodes, assessed using a spring caliper. The diagonal distance was measured between the proximal edge of the distal sense electrode and the distal edge of the proximal sense electrode.
The second method used the linear axial measure recorded between the sense electrodes on the same side of the hand and wrist, and as the proximal wrist electrode was placed in line with the ulnar styloid at the wrist crease, it was assumed that the theory of equipotential points, where points perpendicular to the longitudinal current flow in narrow sections of the body are equipotential in axial positions, and measurement electrode positions on anterior, lateral, and posterior surfaces should result in the same measured reading. 20 The measure for Position 1 (dorsum of hand and wrist) was used in the analysis for Position 2, while the measure for Position 4 (palmar surface of hand and wrist) was interpreted for Position 3.
Measurements of the volume of the hand using BIS were calculated using the formula described in the literature for the calculation of tissue volumes20,23,24:
where V is the volume of the hand, R represents R i or R 0 , L is the interelectrode distance, and ρ is the resistivity coefficient of the fluid, as defined by the SFB7: 235.5 (ECW) and 894.2 (ICW) for females, 273.9 (ECW) and 937.2 (ICW) for males in noninjured, healthy populations. 31 The volumes were calculated for each electrode configuration, using R 0 to calculate the volumes of ECW and R i for the calculation of ICW.
An additional parameter that is recorded by the SFB7 is cell membrane capacitance, which is reflective of cell volume and cell membrane thickness and porosity. 32 Cell membranes interact with applied electrical currents, providing an indicator of tissue composition. 33 Reduced membrane capacitance is linked to deterioration of muscle cell membranes in neuromuscular disease, 34 is a prognostic indicator of survival in head and neck cancer, 35 and is reduced in children with active nephrotic syndrome. 36 Increased membrane capacitance has been noted in disease states resulting in hypertrophy of the cells, such as dilated cardiomyopathy or proliferative vitreoretinopathy.37,38
The electrodes were applied to each point on both hands before BIS recordings so that the measurements could be completed in quick succession. The order of the recordings was randomized. Participants were required to abstain from eating, drinking, or toileting between measures. Measurements were completed in less than 10 minutes for each participant.
Data analyses
The data were downloaded from the SFB7 using supplied software (Bioimp version 5.4.0.3; ImpediMed Ltd, 2012) and processed for analysis according to the Cole model to determine the resistance at zero frequency (R 0 )—impedance of the ECW; resistance at infinite frequency (R∞)—impedance of the TBW; and the resistance of the intracellular compartment (R i ). All analyses were performed using Stata Statistical Software, release 14 (StataCorp LP, 2015, College Station, TX). Descriptive analyses were completed and presented using means and standard deviations (SD). Percentage difference values were also calculated, through which each BIS variable from the alternate electrode positions was expressed as a percentage change of the value obtained from the standard site (Position 1). All further statistical analyses were performed using the raw BIS (not percentage difference) variables.
All three repeated, within-session measurements were recorded and included in the analysis, multilevel mixed-effects linear regression analyses were therefore used to assess associations with differences in BIS variables between the different electrode positions. All models were adjusted for the interelectrode distance. As BMI, gender, age, and hand dominance are known to influence upper limb BIS measures, these factors were also included in the models to assess any interactions. A stepwise, backward elimination of variables was performed to produce the final model, and only statistically significant interactions were included in the final model. The interelectrode distance between the sense electrodes was also assessed for interactions with each electrode position. The results of the regression analyses were reported as regression coefficients, with 95% confidence intervals. A p-value of less than 0.05 was considered statistically significant.
Bland and Altman39,40 described statistical measures of agreement between different methods of clinical assessment, and applicable to assessing a new clinical measure against a gold standard reference. The bias and limits of agreement were calculated for each alternate electrode position against the reference of Position 1.
Results
Participants
Thirty participants (15 female) were included in the study, with measures performed on 60 hands. Mean age of the participants was 33.9 ± 9.87 years; mean BMI was 25.3 ± 3.89 kg·m−2. Summary statistics by gender is shown in Table 1. Two participants (one female and one male) reported being left-handed. The size of the participants' hands is shown in Table 2.
Participant Summary Statistics
BMI, body mass index; SD, standard deviations.
Interelectrode Distance for Each Electrode Configuration
Measures in cm.
IQR, interquartile range.
Hand bioimpedance spectroscopy variables
Mean and SD for hand BIS raw impedance variables for each electrode position are shown in Table 3. Each raw BIS variable has also been adjusted using the distance between the sense electrodes (Ω/cm).
Hand Bioimpedance Spectroscopy Impedance Variables Obtained from the Standard Position and Alternate Positions
Data presented as mean (SD) and difference (%) of the value obtained from standard Position 1.
Percentage of Position 1 reference value.
BIS, bioimpedance spectroscopy.
Examination of the regression coefficients demonstrated that gender, age, and the dominant hand were significantly associated with the raw BIS measures recorded in this study (Table 4). BMI did not significantly influence the BIS measures. Increasing age, being of male gender, and the dominant hand significantly decreased R 0 , R i , and R∞ using both interelectrode measures. There were no interaction effects between the electrode position and the interelectrode distance for the diagonal interelectrode distances. The interaction effect between electrode position and the axial interelectrode distance significantly influenced R 0 and R ∞ .
Changes in Hand Impedance Variables When Alternate Electrode Positions Are Compared with the Standard Electrode Position
p-Value <0.05.
Measures of membrane capacitance were compared for each electrode position to assess for differences between electrode positions (Table 5).
Changes in Membrane Capacitance When Alternate Electrode Positions Are Compared with the Standard Electrode Position
p-Value <0.05.
The analysis demonstrated that there was a significant difference in membrane capacitance between all positions when using the diagonal measures for the interelectrode distance. Using the linear axial measure, there was a significant distance x position interaction for membrane capacitance—X 2 (3, n = 704) = 7.74, p = 0.05. The dominant hand, age, weight, and male gender all influenced the measured membrane capacitance.
Hand volumes were calculated using the BIS variables and the interelectrode distances using each configuration, and compared with the volumes calculated for the Position 1 reference (Table 6).
Calculated Hand Volumes Using Bioimpedance Spectroscopy Variables
Percentage of Position 1 reference value.
Bland/Altman analysis for agreement between Position 1 and each alternate electrode position, using both measures for interelectrode distance, was calculated for the BIS variables R 0 , R i , and R ∞ (Table 7).
Bland/Altman Limits of Agreement with Position 1 for Each Alternate Electrode Position
Discussion
The use of BIS in the clinical setting provides a number of variables that enables the clinician to measure lymphedema. Raw impedance variables provide an index of volume, while measuring interelectrode distances allows the clinician to gain an understanding of the volume of lymphedema within the measured segment. This study showed that when measuring the lymphedema parameters of the hand, compared with the reference electrode array (Position 1), adjusting for axial distance between the electrodes, the alternate positions resulted in variation in R 0 and R ∞ of less than 5% for Position 3 (−2.48% to −1.26%) and Position 4 (2.15% to 4.75%) (Table 3). This is due to impedance varying with body composition and cross-sectional area. 32
The regression analysis when using the axial measures showed that there was a significant difference for each alternate position for R 0 and R∞ (p < 0.001). The position x distance interaction, however, showed that Position 3 and Position 4 were interchangeable with Position 1 for R 0 : X2 (3, n = 723) = 23.51, p < 0.001) and R ∞ : X2 (3, n = 723) = 10.16, p = 0.0172, indicating that Position 3 and Position 4 are interchangeable with Position 1 for measuring R 0 and R ∞ (Table 4). This is also reflected in the measurements for membrane capacitance between positions (Table 5).
Hand dominance is known to result in larger hand volumes, requiring the use of ratios to compare dominant and nondominant hands to inform the measurement of lymphedema.22,41 The dominant hand in this study resulted in decreased impedance (Table 4) and increased capacitance (Table 5), indicating increased size compared with the nondominant hand. For the measurement of hand volumes to detect lymphedema, using these alternate electrode positions, it is recommended that electrode Positions 1, 3, or 4 may be used to assess the hand volume, however, the same electrode configuration should be used on the affected limb and the contralateral limb to assess the interhand ratio.
Acceptable variations using BIS have previously been investigated. Within-day total body resistance varied between 0.3% and 1.9% in a study by Kushner and Schoeller. 42 Variations of less than 5.6% have been shown to be attributed to measurement error using BIS in performing individual measurements. 43 We would consider the acceptable cutoff for comparability (interchangeability) to be 5%, as values larger than this were determined to be clinically significant variability for measures of total body fluid. 19
The alternate Positions 2 and 3 placed the sense electrodes on opposite sides of the hand. The interelectrode distance between the sense electrodes was measured using a diagonal (through the hand) measure, and a linear axial measure along the dorsum or volar surface of the hand to the proximal wrist at the level of the ulnar styloid. Limits of agreement with Position 1 were calculated for each alternate position, using both interelectrode measures (Table 7). The results indicate improved agreement with Position 1 for alternate Positions 2 and 3 when using the axial measurements over the diagonal measures.
The improved agreement using the linear axial measures was also reflected in the regression analyses for impedance and membrane capacitance. There was a significant difference between each alternate position and Position 1 using the diagonal measures for each BIS variable (p < 0.001–0.042), except for R 0 measured in Position 2 (p = 0.304). There was no interaction between electrode position and the interelectrode distance when using the diagonal measure for each BIS variable (Tables 4 and 5), indicating that the alternate electrode positions using diagonal measures are not interchangeable with Position 1 for using BIS to measure hand lymphedema volumes.
Measures for the impedance of the intracellular component (R i ) compared with Position 1 were significantly different for each alternate position except Position 2 using an axial measure (p = 0.443), which was 1.57% less than Position 1. The other alternate positions were also clinically different from Position 1, with greater than 5% variation using both interelectrode measures. As there was no interaction between electrode position and distance for R i , the alternate electrode positions investigated in this study are not interchangeable with Position 1 for measuring R i .
Male gender significantly decreased all BIS impedance variables and increased membrane capacitance using both interelectrode measures, which has been shown previously. 26 These results are reflective of the larger hands and increased intrinsic hand muscle bulk in males, and the decreased R i corresponds with increased muscle mass (Gittings et al., unpublished data).
The hand volumes were calculated using the formula described by Ward et al. 23 (Table 6). The formula is validated for calculating the volume of limbs using BIS and is based on the geometric conical shapes of the limbs. 44 The measures for ECW using Position 4 and ICW using Position 2 were the only calculated volumes within 5% of the calculated measures for Position 1. The complex irregular shape of the hand may require the calculation of a formula specific for hand volume calculation to allow use of BIS for volume calculations, which is reflected in the clinically significant differences (>5% difference) calculated for each electrode configuration.
The impedance of the skin is influenced by the thickness of the stratum corneum, and by the hydration status of the skin.45,46 The standard electrode array places the electrodes over the dorsum of the hand and forearm, and the unique anatomy and function of the hand dictate highly mobile skin, which is thinner than other areas of the body. Several researchers have investigated the electrical impedance of skin at different sites of the body, with increased electrical impedance of the volar forearm skin compared with the skin on the dorsum of the hand,47,48 indicating that this skin is thicker than that on the dorsum of the hand. Membrane resistance of the stratum corneum decreases with improved hydration, while the effective capacitance increases under the same conditions. 46 While the skin was prepared in the same method for each electrode configuration in this study, and the within-subject measures were completed within 2 minutes per hand, the use of moisturizers by the participants was not noted.
Mathematical modeling of skin has variously assumed stratum corneum thicknesses of between 10 and 40 μm at the forearm.49,50 The thickness of the stratum corneum of the volar forearm was calculated, based on a number of cohort studies of females, to be 14 ± 3 μm. 45 In comparison, the thickness of the stratum corneum at the palmar fingertip of the middle finger was measured using optical coherence tomography to be 98 ± 12 μm in females and 111 ± 14 μm in males. 51 The impedance of the stratum corneum of the palm of the hand is therefore greater than nonglabrous skin. Martinsen et al. 49 found that the stratum corneum mainly contributes to the measured impedance at frequencies less than 1 kHz, where higher frequency measurements were representative of the deeper viable layers of the skin. The SFB7 measures from 4 to 1000 kHz, which overcomes the stratum corneum influence, and the tetra-polar arrangement of electrodes minimizes the skin-electrode contact impedance so that the measured impedance relates to the underlying body tissues only, 20 however, small-area segmental and localized BIS results in lower tissue impedances when compared with whole-body BIS measures, which the SFB7 is designed to measure. 52
While the tetra-polar arrangement minimizes skin-electrode contact impedance to measure BIS, it is dependent on similar contact impedance at each electrode position. The skin-electrode contact impedance varies according to body site measured, and is relatively large, which can distort the measured tissue impedance. 52 This may lead to high-frequency artifact when measuring BIS due to the capacitive effect of the cells, leading to errors in the derived Cole parameters at these increased frequencies. 53 The electrode impedance mismatch does not appear to affect the measures of R 0 , which is the BIS measure representative of ECW, and therefore, lymphedema as the artifact occurs at higher frequencies. 53
The electrode impedance mismatch also allows for spot measurement of lymphedema. Impedance transverse to the longitudinal direction of current flow, or spot measurement, is calculated using vector algebra from a combination of bipolar and tetra-polar BIS measures. Bipolar measurement techniques measure impedance in the tissues parallel and transverse to the current flow, while tetra-polar BIS measures tissue impedance parallel to the direction of the current flow.54,55 This technique therefore isolates the impedance of the skin from the underlying soft tissues, which can determine the composition of these tissue changes with the progression of lymphedema. 54
Conclusion
The results in this study indicate that electrodes may be placed on the volar surface of the hand and forearm, or a combination of electrodes on the palm of the hand and the dorsum of the forearm, to measure R 0 and R ∞ . This provides a technique to measure hand lymphedema where wounds otherwise preclude the use of electrodes on the dorsum of the hand and forearm. The raw BIS variables should be interpreted for changes in tissue volumes in a clinical setting, as calculated volumes may result in clinically significant variation.
Future Studies
Future investigations are required to determine if reverse electrode positions counter the electrode-skin contact mismatch, and if spot measurement of lymphedema is a valid technique in the hand. The use of hand BIS and these alternate electrode positions needs to be validated in wound populations. Improved formulae for calculating hand volumes using BIS to account for the complex geometrical shape of the hand also need to be determined.
Footnotes
Author Disclosure Statement
There are no conflicts of interest to be reported.
Funding Information
Dale Edwick's part-time research salary (Chevron Fellowship) is supported by the Fiona Wood Foundation, Western Australia. Dale Edwick's PhD research is also supported by the Australian Government Research Training Program Scholarship.