
Abstract
Background:
Monofrequency bioelectrical impedance analysis (BIA) protocols seek to further quantify changes in lymphedema compared with traditional circumferential evaluations. Complex decongestive therapy (CDT) is an effective method of reducing unilateral upper limb lymphedema secondary to breast cancer treatments. Comparing lymphedema measurements between segmental tetrapolar BIA, total body BIA, and circumferential measurements during therapeutic changes can improve our quantitative assessment ability for this prevalent medical complication.
Methods and Results:
Twenty-two patients with breast-cancer-related unilateral upper limb lymphedema participated in this prospective observational study. Circumferential measurements, segmental tetrapolar BIA, and total body BIA were obtained and compared before CDT, immediately after 10 sessions of CDT, and 30 days post-CDT to assess lymphedema. The segmental tetrapolar BIA correlated well with improvements in circumferential measurements of the limb. We found that the resistance value cutoff point of 237 Ω could indicate a recurrence of lymphedema.
Conclusions:
Segmental, tetrapolar monofrequency BIA provides a simple method to monitor and evaluate the efficacy of therapy in the outpatient setting by operators with minimal training. This protocol could aid quantitative evaluations of unilateral upper limb lymphedema.
Introduction
Lymphedema is a common condition affecting an estimated 140–250 million people worldwide. 1 Lymphedema is a clinical manifestation of a failure of the lymphatic system from idiopathic or secondary causes such as surgery, radiation therapy, or malignancy. One of the most notable populations suffering from secondary lymphedema are patients after interventions to treat breast cancer. National and international guidelines2,3 identify complex decongestive therapy (CDT) as the gold standard for treating lymphedema. CDT consists of skin care, manual lymphatic drainage, compression garments, and range of motion exercises.
Streamlining of public health resources to increase rehabilitation for this condition requires optimization of monitoring and evaluation techniques according to evidence-based medicine. The measurement for the severity and changes of lymphedema is not standardized and primarily relies on clinical judgment and circumferential limb measurements. Other methods of quantitative lymphedema measurements include water displacement method, perometry, and bioelectrical impedance analysis (BIA). Each method has issues regarding cost, availability, or ease of use. Circumferential limb measurements calculate volumetric changes indirectly and are susceptible to operator biases. Water displacement method, which measures volumetric changes when a limb is submerged, requires a large space, positioning, which can be difficult for patients, and special attention to hygiene. Perometry is an optoelectronic measuring method that is accurate and fast, but the equipment is expensive for clinical use. 4 BIA is a rapid, noninvasive, low-cost examination that detects lymphedema by measuring tissue impedance of a weak electrical current.5,6 Monofrequency and multifrequency BIA exist and are used in the evaluation of lymphedema. In Italy, where this study was performed, monofrequency BIA is the most commonly available and clinically utilized technique due to its lower cost and ease of use.
A pilot prospective observational study was conducted to (1) verify CDT therapeutic effects in patients affected by secondary, unilateral upper limb lymphedema; (2) assess diagnostic accuracy between monofrequency BIA and circumferential limb measurements; and (3) identify the appropriate application and limits of the BIA in the outpatient clinic setting.
Materials and Methods
Investigators recruited participants from the outpatient clinic of the Department of Physical Medicine and Rehabilitation or the Department of Oncology's outpatient breast care unit. Patient characteristics are shown in Table 1. Twenty-two patients with unilateral upper limb lymphedema secondary to breast cancer surgery were eligible (21 women, 1 man) with a medium age 61.2 years (age range of 42–78). Ten patients had right arm lymphedema (45.5%), and 12 patients (54.5%) had left arm lymphedema. A staff physiatrist screened all participants for appropriateness and safety to participate in CDT. Patients with a pacemaker or with complicated lymphedema (phlogosis, infection, lymphosclerosis, and phlebitis) were excluded. This investigation was approved by the institutions ethical review board.
Patient Characteristics
Body mass index precomplex decongestive therapy (T0).
Body mass index immediately postcomplex decongestive therapy (T1).
Body mass index 1 month postcomplex decongestive therapy (T2).
A medical file was created for participants' demographic data, medical history, and surgical history (including medical and surgical cancer treatments, lymphedema history, comorbidities, and medications). The physical examination consisted of inspection and palpation of the affected limb. Inspection included notation of skin color, trophic changes, skin temperature, skin lesions, vascular aberrations, and posture. Palpation included notation of skin temperature, nearby lymphadenopathies (laterocervical, axillary, supraclavicular), residual breast and upper limb edema, and shoulder function (muscular and joint evaluation). Pain was evaluated with the Numerical Rating Scale. Body mass index (BMI) was calculated from weight (range: 58.6–96.8 kg) and height (range: 147–166 cm) measurements.
Circumferential measurements of both arms were taken with a nonelastic tape measure by the same physical therapist at the beginning and end of each CDT session. Then, circumferential measurements were collected every 10 cm starting at the volar wrist and progressing proximally to 40 cm. 7 A Delta value calculated the difference between the affected and nonaffected arm. An excel file prepared with the cone–trunk geometrical formula 7 was used to convert circumferential measures (cm) to volumetric estimates (mL). The measurements between the metacarpal joints and wrist were excluded from the cone–trunk geometrical formula due to inherent anatomical variations prohibiting standardization.
Every patient received BIA in the Clinical Nutrition Department. BIA was performed three times: pre-CDT (T0), post-CDT treatment within 24 hours of final CDT session (T1), and at 1-month follow-up (T2). BIA was scheduled before same-day chemotherapy infusions to avoid measurement errors. BIA was performed by a first-year physical medicine and rehabilitation resident after 1 day of training and successful performance of the required techniques. Training was given by a dietician with a master's degree in body composition measurements and 20 years of BIA experience, who was available for supervision.
The monofrequency BIA 101 (Akern, Florence) model used had a resistance range 0–999 Ohm (Ω), reactance range 0–100 Ω, and an active phase between 1 and 10. Disposable low impedance Biatrodes™ electrodes (size 27 × 29 mm; Akern) were applied by the resident physician investigator after orientation to the BIA device and instruction on electrode placement. Successful bioelectrical impedance data collection took <15 minutes under the supervision of expert user. 8 Metal objects (e.g., bracelets, rings, and necklaces) were removed to avoid interfering with the device.
Each BIA session collected a total of four measurements: total body method followed by the tetrapolar segmental method was performed bilaterally. 9 The participant was in a relaxed supine position with 35°–40° shoulder abduction for BIA preparation and data collection. The total body method requires two pairs of electrodes positioned on the dorsum of the ipsilateral hand and foot. The signal injectors electrodes (red) were placed distally (on the ipsilateral metacarpals and metatarsals). The sensor electrodes (black) were placed proximal to signal injector electrodes (between the styloid processes of the radius and ulna and between the medial and lateral malleoli).
The tetrapolar segmental method9,10 requires one signal injector and sensor pair on the dorsum of the ipsilateral hand and wrist (mirroring the total body method), and a second electrode pair with the sensor electrode on the contralateral dorsum of the wrist (level of styloid process) and signal injector electrode on the ipsilateral dorsum of metatarsal heads. The alternating current, flowing between the ipsilateral foot and hand, measures the potential difference between the ipsilateral hand and contralateral hand.
After initial BIA evaluation (T0), patients began a series of 60-minute physical therapy sessions, 5 days a week for a total of 10 sessions, focused on CDT. Sessions included manual lymph drainage, multilayer compression bandages, and a lymphedema-specific exercise program. Every therapy session for all participants was directly supervised and performed by the same physical therapist, who was a specialist in lymphatic treatments. All sessions were augmented with a home exercise program.
At the end of the 10th session, a physiatrist performed a same-day re-evaluation and prescribed an upper limb compressive garment to continue at home. Within 24 hours of the last physical therapy session, patients underwent their second BIA evaluation (T1). One month later, the final BIA was repeated (T2).
Statistical analysis
Descriptive statistics included are mean ± standard deviation, Student's t-test for paired data, and statistical comparison for independently sampled and quantitative data. A linear regression evaluated the relationship between sample data to estimate a conditional, expected value of a dependent variable. To measure the accuracy of continuous variables and to identify the optimal cutoff value and maximize the difference between true positives and false positives, we used the receiver operating characteristic (ROC) curve analysis technique. The distribution of variables is represented by a box and whiskers plot, subdivided into quartiles and a median central value. All analyses were considered significant if p < 0.05.
All statistical analyses were performed with MedCalc Statistical Software version 18.11.3 (MedCalc Software BVBA, Ostend, Belgium).
Results
After rehabilitative treatment with CDT, 18 of 22 patients (81.8%) experienced a reduction in circumferential measurements and volumetric calculations of the pathological limb. The same patients experienced an improvement in edema shown by BIA with increased bioelectric resistance (Ω).
It was not possible to establish a statistically significant difference in the Delta of the lymphedematous and normal limb for circumferential measurements and volumetric calculations. However, we did find a statistically significant correlation between circumferential and bioelectrical resistance measurements (T0: p < 0.0001, r = 0.75; T1: p < 0.0001, r = 0.77). There were no statistically significant changes in bioelectrical impedance values obtained with the total body method at T0, T1, and T2 (Table 2). However, the tetrapolar segmental method, shown in Table 3, shows statistically significant variations in resistance, reactance, and phase angle of the edematous limb with respect to the normal limb (T0: p < 0.0001; T1: p < 0.0001; T2: p = 0.0003).
Total Body Method Bioelectrical Impedance Analysis
Precomplex decongestive therapy (T0).
Immediately postcomplex decongestive therapy (T1).
One month postcomplex decongestive therapy (T2).
Tetrapolar Segmental Method Bioelectrical Impedance Analysis
Unilateral upper extremity affected by breast-cancer-related lymphedema.
Precomplex decongestive therapy (T0).
Immediately postcomplex decongestive therapy (T1).
One month postcomplex decongestive therapy (T2).
Variation in resistance values in the tetrapolar segmental method in T0 versus T1 is significant in the normal limb (p = 0.0009); the edematous limb approaches but does not reach significance (p = 0.09). We found no statistical significance comparing reactance and phase angle T0 versus T1 in the lymphedematous limb or the normal limb (p = 0.6 and 0.2 in the lymphedematous limb; p = 0.3 and 0.8 in the normal limb).
The statistically significant values of the tetrapolar segmental method bioelectrical impedance correlated with the circumferential and volumetric values at T0 and T1. This correlation for both edematous and normal limbs was statistically significant (Table 4).
Correlation Between Segmental Tetrapolar Bioelectrical Impedance Analysis and Circumferential Measurements of Lymphedema
Unilateral upper extremity affected by breast-cancer-related lymphedema.
Precomplex decongestive therapy (T0).
Immediately postcomplex decongestive therapy (T1).
Volumetric calculations based on circumferential measurements.
Figure 1 illustrates the positive clinical response to CDT correlates with the increased resistance observed from T0 to T2. Figure 2 illustrates the sensitivity and specificity of the resistance cutoff (237 Ω) predictive of upper limb lymphedema recovery T0 to T2. No adverse reactions of any kind were observed or reported during BIA assessments.

Lymphedematous upper extremity segmental tetrapolar bioelectrical impedance. Precomplex decongestive therapy (T0), immediately post-therapy (T1), and 1-month post-therapy (T2). Min < LQ < median > UQ > max, fences (1.5 and 3.0 IQR). IQR, interquartile range; LQ, lower quartile; UQ, upper quartile.
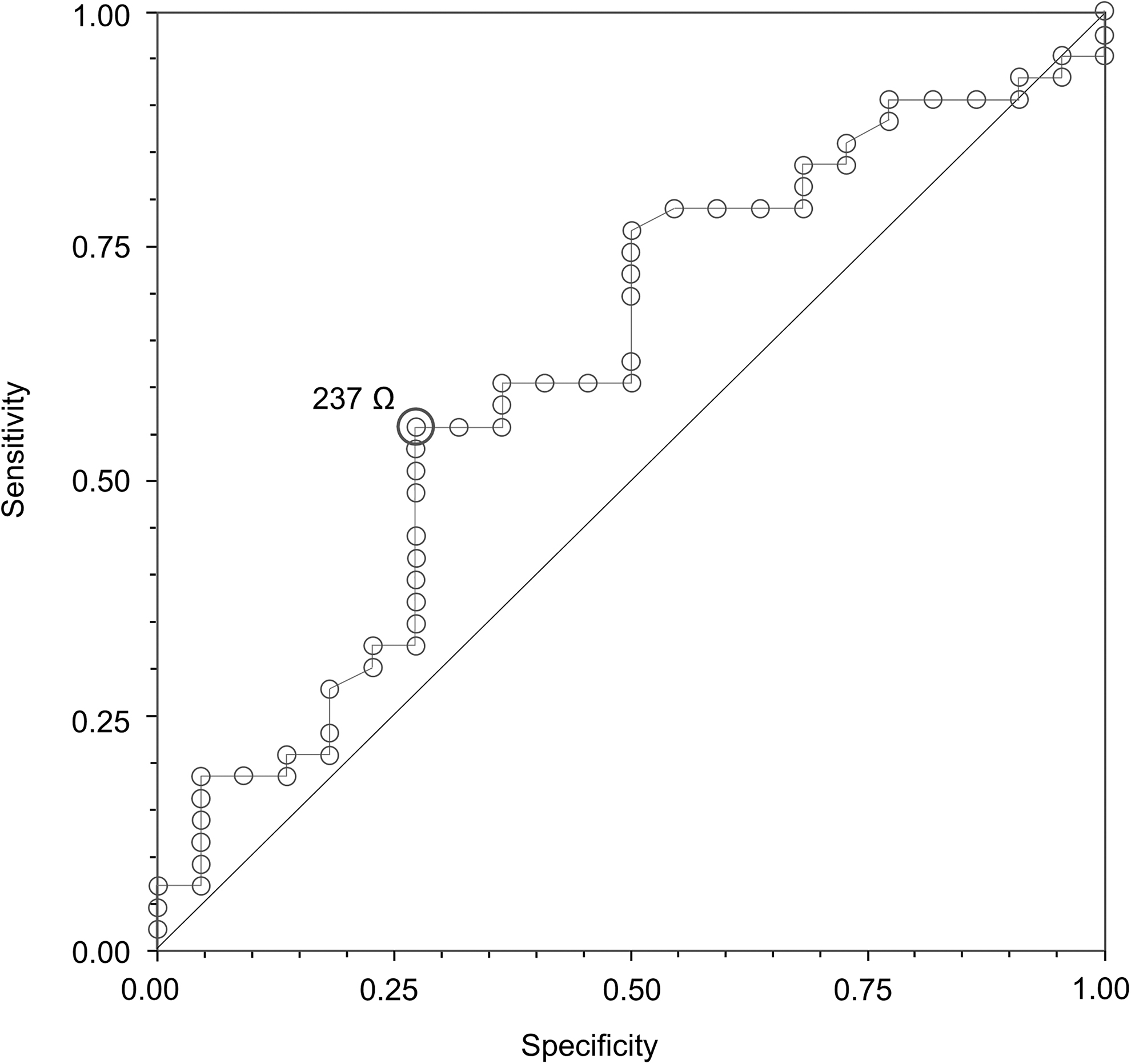
ROC curves of segmental tetrapolar bioelectrical impedance in lymphedematous upper extremity. Schematic of ROC curve detected with bioelectrical impedance analysis tetrapolar segmental method. Resistance value 237 Ω represents the threshold for recurrence of lymphedema. ROC, receiver operating characteristic.
Discussion
CDT produced a circumferential and calculated volumetric reduction as well as an increased resistance in BIA of the lymphedematous limb in most patients. Likely due to the small sample size, this reduction in edema was not significant for therapeutic efficacy of CDT, and no threshold value of treatment effectiveness could be identified. Even with this limitation, the confirmation of BIA as an objective, reproducible measurement method for upper extremity lymphedema is an important finding. Among the two BIA methods used in the study, the most suitable for the evaluation of upper limb lymphedema was the tetrapolar segmental method. The total body method evaluates the quantity of liquids in the whole person and did not help in detecting changes in resistance, reactance, and phase angle in a focal area. The tetrapolar segmental method provides data on fluid presence specific to an upper limb, minus the most distal aspect of the hand. The bioelectrical impedance of the hand cannot be obtained due to inherent anatomical variations excluding standardization; the same limitation exists in the volumetric calculations of circumferential measurements.
The variations in resistance neared statistical significance, and the variations of reactance and phase angle between T0, T1, and T2 with segmental technique in the lymphedematous limb. We assume that this lack of significance is due to the small sample size; the correlation of the impedance resistance value with the circumferential reduction of lymphedema with the three-stroke ROC curve supports this hypothesis. The predicted resistance cutoff of clinically relevant edema was 237 Ω with a 56% sensitivity and 73% specificity for identifying lymphedema. BIA cannot detect changes in tension or consistency of soft tissues. Currently, clinical evaluation remains the most comprehensive way to evaluate and diagnose lymphedema and the therapeutic effect of CDT.
In addition, it is interesting to note that these data show that the lymphedema improvement after 10 CDT sessions was maintained or even further improved at 1-month follow-up in T2. The data suggest efficacy not only of the “intensive” rehabilitation treatment in a health care environment but also the importance of a self-directed, daily, home maintenance program, including compression garments and exercise. It would be interesting to reassess patients examined at progressive intervals of 60 and 90 days to evaluate the long-term effectiveness of CDT and home interventions.
Study limitations
Limitations include small sample size, breast-cancer-related lymphedema only, use of monofrequency BIA instead of multifrequency spectroscopic BIA.
Conclusion
This study suggests that the BIA tetrapolar segmental method can be a simple, quantitative way to measure and monitor changes in upper extremity lymphedema for clinical and research purposes. Both the traditional circumferential measurements with volumetric calculations and BIA correlated in showing this improvement after CDT and at 30-day follow-up. The continuation of a home treatment program with compression garments and exercise is likely important in maintaining the effects of CDT.
The data obtained from the monofrequency BIA with a segmental technique indirectly confirm what was observed by York et al., 11 namely the ability of this method to record quantitative (even if not qualitative) volumetric variations of the limbs, like the multifrequency spectroscopic BIA. 12 Currently, there are no reference values for body composition for tetrapolar segmental BIA (only for total body BIA), but studies sponsored by the equipment manufacturing companies are underway.
In the future, it is conceivable that tetrapolar segmental BIA will provide qualitative as well as quantitative information on body composition. This would allow clinicians and physical therapists to accurately identify the “gap” between healthy and pathological limbs, and define the quantitative cutoffs for therapeutic efficacy.
BIA could routinely support the clinical evaluation and eventually aid in edema-type identification. BIA certainly offers clinical advantages over the traditional measurements in terms of personnel resources and comfort for the patient. BIA is quick to perform with low costs and has no known side effects. While BIA and circumferential measurements take a similar amount of time to perform, depending on operator proficiency, the quantitative results of lymphedema in BIA are less operator dependent compared with circumferential measurements. BIA, therefore, could reduce errors in both scientific and clinical evaluations of lymphedema. It is still necessary to have adequate training of the health care doctors and technicians for the correct execution and interpretation of the data.
The possibilities demonstrated by the segmental BIA suggest the need for more robust studies to evaluate the ability of this method to (1) assist in the differential diagnosis, (2) predict the duration and therapeutic effects of lymphedema treatments, and (3) provide long-term monitoring of lymphedema.
Footnotes
Acknowledgment
This study is original without previous publications or presentations.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.