
Abstract
Background:
A disturbance of the superficial lymphatic system (dermal backflow) in patients with breast cancer-related lymphedema (BCRL) can be visualized by near-infrared fluorescence imaging or lymphofluoroscopy. In clinical practice, exact measurement of the dermal backflow is difficult. The purpose of the study is to investigate the concurrent validity between the clinical assessments and the lymphofluoroscopy in patients with BCRL.
Methods and Results:
Forty-five patients with BCRL stage I to IIb received lymphofluoroscopy and clinical assessments of their edematous limb (pitting status, skinfold thickness, skin elasticity, water content, lymphedema volume, and extracellular fluid). The correlation between the clinical assessments and the result of the lymphofluoroscopy was determined. The best overall agreement with dermal backflow was found for the clinical assessment pitting status, skinfold thickness, and water content. Overall sensitivity was excellent for lymphedema volume (92.5%), high for skinfold thickness (86.6%) and water content (75.0%), and moderate for pitting status (67.7%). Overall specificity was excellent for skin elasticity (94.7%), high for pitting status (83.4%), and moderate for skinfold thickness (61.6%) and water content (74.8%). In the evaluation of the whole arm, measurements of the excess volume were significantly greater for patients in an advanced stage of dermal backflow in comparison with patients in an earlier stage of dermal backflow (p = 0.002).
Conclusions:
The clinical assessments of skinfold thickness, water content, and lymphedema volume are the most appropriate tools to detect dermal backflow according to the lymphofluoroscopic images. To confirm the absence of dermal backflow, pitting status can be recommended.
Introduction
Breast cancer-related lymphedema (BCRL) is the swelling of the upper limb after treatment for breast cancer (secondary, acquired lymphedema). The regional swelling is usually a result of a disturbed transport capacity (related to radiotherapy and/or surgery) and an increase in lymph load.1–3
There are different methods to evaluate BCRL in a clinical setting, yet, there is no consensus concerning the best standard measurement tool. 4 The volume of the limb can be assessed with circumference measurements; based upon these data, excess volume can be calculated. 5 Water displacement is another technique to assess the volume. 6 Hereby, the extremity is immerged in a container of water and the amount of the displaced water represents the volume of the limb. 7 The amount of water in the edematous limb can also be assessed by means of a pitting test, 8 bioelectrical impedance spectroscopy, 9 or the tissue dielectric constant.10,11 Measurement of the skinfold thickness (Stemmer sign) can be performed, an increased thickness is a typical sign for lymphedema. 12
Near infrared fluorescence imaging of the lymphatic system, also called lymphofluoroscopy, is an imaging technique that can be used to assess the lymphatic architecture. A tracer, indocyanine green (ICG), is injected in the patient's limb. Once excited by a near-infrared light, ICG emits a fluorescent photon. By visualizing this fluorescence of near-infrared light, the lymph flow can be observed.13,14 The technique provides real-time video images of the lymphatic transport. This real-time imaging is an advantage as you clearly see the lymph vessels and areas of disturbances immediately on the screen and are able to mark these areas on the affected limb. The patient can visualize the images himself and will be able to understand the pathology better.
In healthy subjects, lymphofluoroscopy shows a linear lymph transport pattern. Three dysfunctional backflow patterns of lymphatic transport can be distinguished in patients with lymphedema. The first one is the splash pattern, representing a dispersed tracer in tortuous lymphatic channels. The second one, more severe disturbed pattern, is the stardust pattern, which demonstrates spotted fluorescent signals, representing the effusion of lymph fluid out of the lymphatic capillaries into the interstitium. The last type of pattern is the diffuse pattern by which the tracer is widely distributed without identifiable spots. In this pattern, besides the accumulation in the lymphatic capillaries and lymph precollectors, lymph is stagnated in the interstitium. 15
The information obtained by lymphofluoroscopy can be used to optimize the treatment of BCRL. By clearly identifying the dermal backflow areas and the remaining lymph vessels, manual lymph drainage can be adjusted according to that image. This fluoroscopy-guided manual lymph drainage is an individual tailored approach. 16 The pressure of the therapist's hands will be different in an area where dermal backflow can be seen. A more severe dermal backflow pattern requires a higher pressure. The lymph flow stimulating effect of this technique was demonstrated in healthy volunteers and in patients with BCRL.17,18 Also according to the images, adjustment to the compression hosiery can be made. Unfortunately, lymphofluoroscopy is a rather intensive examination that needs to be performed in a medical setting and requires specific and expensive equipment. The question is whether the result of the lymphofluoroscopy can be partially estimated by a clinical assessment of lymphedema so that lymphofluoroscopy will not be necessary in all cases, but an individualized treatment can still be offered.
Therefore, the purpose of this study was to examine the concurrent validity between the clinical assessment of a patient with lymphedema and the results obtained from lymphofluoroscopy.
Materials and Methods
Participants
Patients with BCRL of the arm and/or hand were recruited at the University Hospitals of Leuven and the University Hospital of Antwerp for the EFforT-BCRL trial (Effectiveness of Fluoroscopy-guided manual lymph drainage for treatment of BCRL). 16 Data of the first 45 patients were collected between February 2016 and March 2017. The same inclusion and exclusion criteria were used as in the EFforT-BCRL trial: (1) patients with BCRL and >18 years of age, (2) chronic lymphedema (>3 months present, stage I to IIb), and (3) at least 5% difference (measured with circumference measurements) between both arms/hands adjusted for dominance. Exclusion criteria were allergy for iodine, sodium iodine, or ICG, increased activity/benign tumors of the thyroid gland, edema of the upper limb from other causes, active metastasis of the cancer, reconstructive or debulking surgery of the lymphatic system in the past, inability to participate during the entire study period, and mentally or physically unable to participate. This study was approved by the Ethical Committee of the University Hospitals Leuven (S-number 58689) and Antwerp. All participants signed informed consent. For this study, the STROBE statement was used.
Study design
In this cross-sectional study, all included patients underwent near-infrared fluorescence imaging and a series of clinical measurements of their edematous limb, with a maximum of 3 weeks between both assessments. Only measurements at baseline were used.
Lymphofluoroscopy
All lymphofluoroscopies were performed by the same vascular surgeon, who is experienced in performing these investigations and was assisted by an experienced physical therapist. A standard protocol for lymphofluoroscopy was applied. 16 With one syringe of 1 mL, a solution of 0.2 mL ICG, saline water, and pure water was strictly injected intradermal at the first and fourth web space, dorsally in the hand of the edematous limb. To visualize the lymphatic system, an infrared camera system (PDE Camera®; Hamamatsu, Japan) was used.
All the information about the lymphatic transport was documented in a standard evaluation document. The active lymph nodes and vessels as well as the dysfunctional backflow patterns (splash, stardust, diffuse) were drawn on a body diagram (Fig. 1).
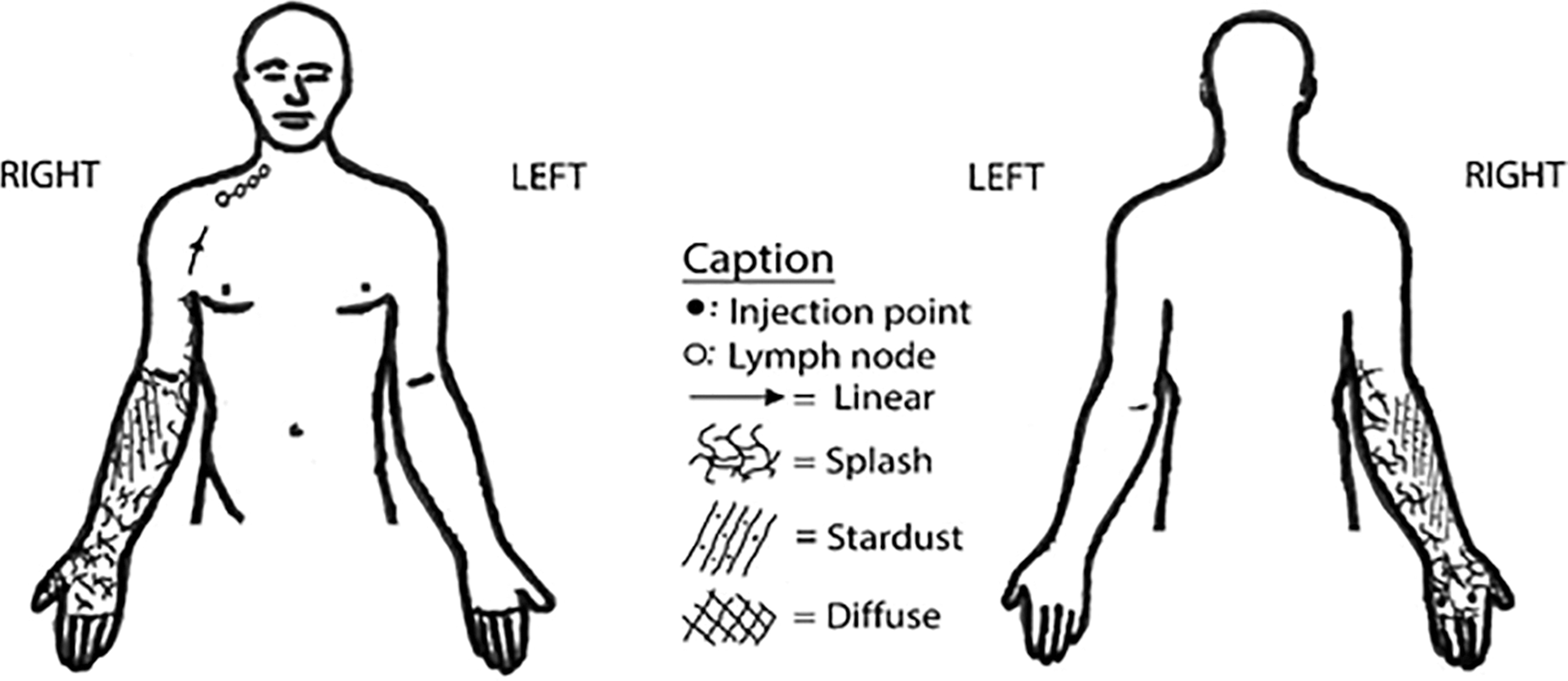
Example of a body diagram based on the lymphofluoroscopic images.
Clinical assessment
Table 1 gives an overview of the different clinical assessments. Three experienced investigators performed all measurements. To ensure blinding, the investigator of the clinical measurements was different from the one performing the lymphofluoroscopy.
Description of the Different Clinical Assessment
TDC, tissue dielectric constant.
Data processing
First, two researchers analyzed the lymphofluoroscopic image independently. Thereafter, they discussed their findings to reach a consensus about the evaluation of the lymphofluoroscopy. Finally, they analyzed the clinical assessments.
Lymphofluoroscopy
A transparent body diagram with the reference points was placed on the body diagram of the lymphofluoroscopy, the presence of dermal backflow at seven different reference points (Fig. 2) was determined (yes/no). Second, arm dermal backflow stage (ADBS) was determined. Five different stages are differentiated (ADBS stage I–V): ADBS I shows a splash pattern; in ADBS II, a stardust pattern is seen proximally to the olecranon; in ADBS III, the stardust pattern exceeds the olecranon; in ADBS IV, the stardust pattern is seen in the whole arm; and in stage V, a diffuse pattern is detected. This is a severity staging system that illustrates a significant correlation with clinical stage. 19
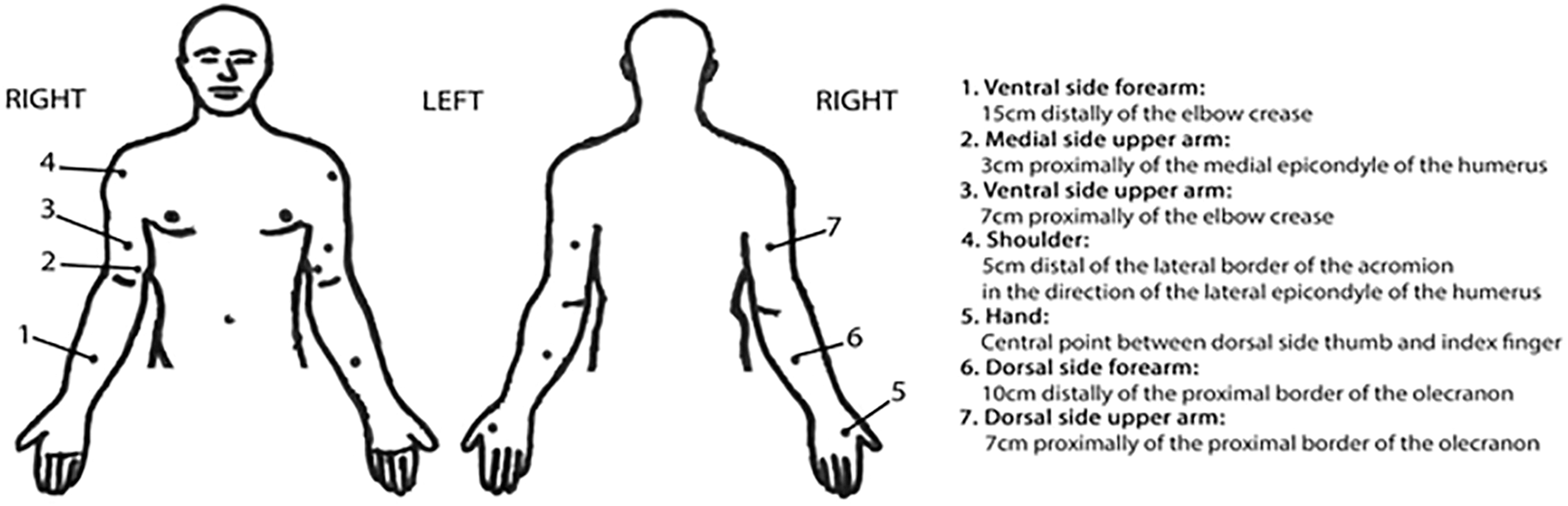
Description of the different reference points needed for the local clinical assessments and to determine the presence of dermal backflow.
Clinical assessment
Results of the clinical measurements of pitting status, skinfold thickness, elasticity, and water content (scored as positive or not positive, detailed description of the scoring is presented in Table 1) were evaluated at the same reference points (Fig. 2) as used in the evaluation of the lymphofluoroscopy.
The lymphedema volume was assessed by the water displacement method and by bioelectrical examination. The water displacement method reference points are shown in Figure 3. The volumes of the different regions defined by the water displacement reference points were matched to the reference points of the above-mentioned clinical measurements to enable comparison: the volume of the hand (up to point A) corresponded to the reference point at the dorsum of the hand (point 5), the volume of the lower part of the forearm (up to point B) to the point at the ventral side of the forearm (point 1); the volume of the upper part of the forearm to the point at the dorsal side of the forearm (point 6); and the volume of the upper arm to the points at the medial side of the upper arm, ventral side of the upper arm, and dorsal side of the upper arm (point 2, 3, 7).
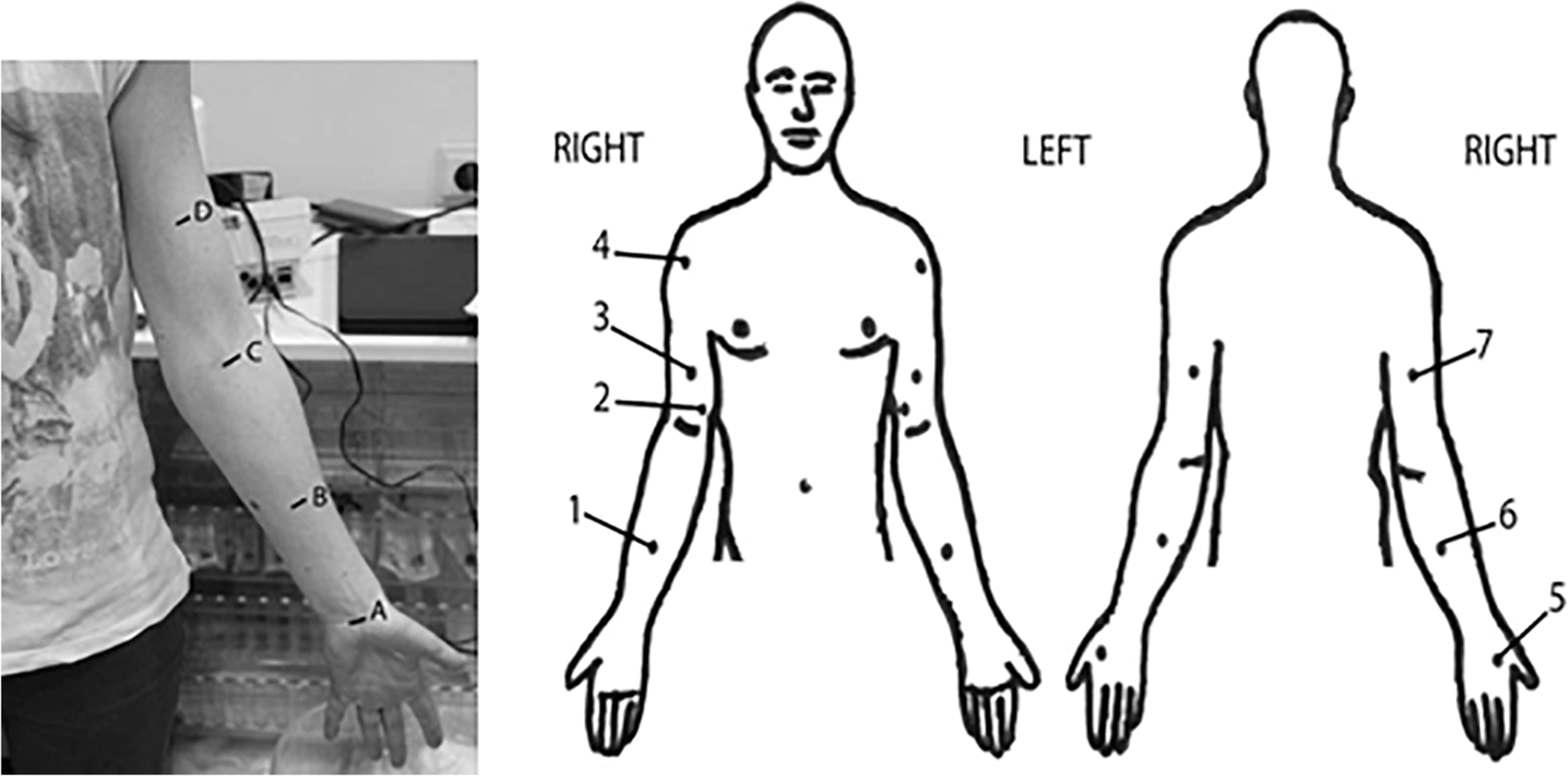
Matching the reference points for the volume measurements
Concurrent validity
To determine the correlation between the lymphofluoroscopy and the clinical assessments, the results of the clinical measurements (pitting status, skinfold thickness, skin elasticity, water content, and lymphedema volume) were compared to the presence of the dermal backflow (yes/no, independent of the type of dermal backflow pattern) seen by the lymphofluoroscopy at the seven reference points. The results of the lymphedema excess volume and extracellular fluid of the whole arm were compared to the different stages of the arm dermal backflow. The sensitivity and specificity of the clinical assessments were controlled by lymphofluoroscopy.
Data analysis
Statistical analyses were performed with SPSS 24.0. A 5% level of significance was applied. Patient and clinical characteristics were described using descriptive statistics.
To determine the agreement between the lymphofluoroscopy (0 = no backflow, 1 = dermal backflow [splash, stardust, and diffuse]) and the clinical assessments (pitting status, skinfold thickness, elasticity, water content, and lymphedema volume) (0 or 1, Table 1), Cohen's kappa statistics was used. The kappa coefficients were interpreted as follows: <0.400 was a weak agreement, between 0.400 and 0.744 was a moderate agreement, between 0.745 and 0.900 was a strong agreement and >0.900 was a very strong agreement. 20
Sensitivity and specificity were interpreted as follows: <60% was a weak sensitivity or specificity, between 60% and 74% was a moderate sensitivity or specificity, between 75% and 90% was a high sensitivity or specificity, and >90% was an excellent sensitivity or specificity.
A Kruskal–Wallis test was used to compare the lymphedema volume of the whole arm and extracellular fluid of the arm to the ADBS. To make comparison possible, three different groups were created based on the ADBS. The first one included ADBS I, which represented an early stage of dermal backflow. The second one represented a partial stardust pattern (ADBS II and III). The third one described an advanced lymphatic dysfunction (ADBS IV and V). To compare the differences between the stages, post hoc analyses were performed with the Mann–Whitney U-test. Due to multiple comparisons and the associated risk of type I error, a Bonferonni correction was applied to the significance level.
Results
Forty-five patients with a mean age of 61.3 years (range 37–82; SD 9.9) were included in the study. Body mass index (BMI) ranged between 20.9 and 39.3 (mean 27.8; SD 4.8). Detailed patient characteristics are summarized in Table 2.
Overview of the Characteristics of the Included Patients
Mean and standard deviation for continuous data; frequency and percentage for discontinuous data.
Not normal distributed: median (interquartile range).
ADBS, arm dermal backflow stages; BMI, body mass index.
Table 3 shows the agreement between the presence of dermal backflow and the clinical measurements at the seven reference points. For lymphedema volume, a moderate agreement was found for the hand (kappa = 0.636) and ventral forearm (kappa = 0.545). A strong agreement was noticed for the dorsal forearm (kappa = 0.760). For pitting status, evaluation of the skinfold and water content, an overall moderate agreement was found. The clinical outcome parameter elasticity showed a moderate agreement for the shoulder region (kappa = 0.483).
Correlation Between Lymphofluoroscopy (Dermal Backflow Yes/No) and Clinical Measurements (Positive or Negative Test 0/1)
Statistical significance was determined at the level of p < 0.05.
Table 4 shows the sensitivity and specificity of the different clinical measurements in comparison to the dermal backflow patterns obtained by lymphofluoroscopy. Overall sensitivity was excellent for lymphedema volume (92.5%), high for skinfold thickness (86.6%) and water content (75.0%) and moderate for the clinical outcome parameter pitting status (67.7%). Overall specificity was excellent for elasticity (94.7%), high for pitting status (83.4%), and moderate for the clinical outcome parameters skinfold thickness (61.6%) and water content (74.8%).
Sensitivity and Specificity of Clinical Measurements
The agreement of dermal backflow with lymphedema volume and extracellular fluid of the whole arm was determined by the different stages of the ADBS.
Table 5 describes the number of patients, median, and interquartile range for lymphedema excess volume and extracellular fluid of the whole arm for the different stages of ADBS. There was a significant difference between the lymphedema excess volume for the different ADBS (p = 0.004). The excess volume was significantly greater for patients in ADBS II/III in comparison with patients in ADBS I (p = 0.002). There was borderline significant difference in excess volume for patients in ADBS IV/V in comparison with patients in ADBS I (p = 0.090). There was no significant difference in excess volume between ADBS II/III and ADBS IV/V (p = 1.000).
Description of Number of Patients, Median, Interquartile Range and p-Value for Lymphedema Excess Volume, and Extracellular Fluid of the Whole Arm for the Different Arm Dermal Backflow Stages
Statistical significance was determined at the level of p < 0.05.
N, number of patients.
The amount of extracellular fluid did not show a significant difference for the different ADBS (p = 0.100). In more detail, no significant difference was found in amount of extracellular fluid between ADBS I and II–III (p = 0.144), ADBS I and IV–V (p = 0.136), and ADBS II–III and IV–V (p = 1.828).
Discussion
To our knowledge, this is the first study investigating the concurrent validity between clinical assessments and dermal backflow obtained from lymphofluoroscopy in patients with BCRL.
The pitting test showed an overall moderate agreement with the presence of dermal backflow. Especially the hand, dorsal forearm, ventral forearm, and dorsal upper arm had a moderate agreement with dermal backflow. For these regions, the result of the pitting test agreed with the lymphofluoroscopic image. A high overall specificity was found for the pitting test. Be aware that in this study, only stage I to IIb lymphedema patients were included. One of the inclusion criteria for the EFforT-BCRL trial was the presence of pitting somewhere in the limb. Patients with lymphedema stage III, where the pitting is no longer present because of advanced fibrotic changes, did not take part in the study. In conclusion, patients in stage I to IIb lymphedema without pitting are likely not to have dermal backflow.
The skinfold thickness showed an overall moderate agreement with the presence of dermal backflow. Especially the hand and dorsal forearm had a moderate agreement with dermal backflow. A high overall sensitivity for skinfold thickness was seen. Therefore, if an increased skinfold thickness is found in patients with lymphedema stage I to IIb, a disrupted lymphatic transport can be expected.
A weak agreement was seen between elasticity and the presence of dermal backflow. If manual palpation indicates that there is no or soft edema, the presence of dermal backflow cannot be excluded. Alternatively, in case of hard edema, the presence of dermal backflow may not be expected. The weak agreement corresponds to what is described in the literature, for example, advanced fibrotic and fatty changes are rare in stage I to IIb lymphedema. 21 Consequently, the lymphatic transport can be disturbed without a positive clinical test for elasticity. Therefore, elasticity is not a suitable parameter to evaluate lymphatic transport in stage I to IIb lymphedema patients.
For the water content, an overall moderate agreement was seen. For the regions hand, ventral forearm, dorsal forearm, and ventral upper arm, the result of the water content correlated with the lymphofluoroscopic image. A high overall sensitivity and a moderate overall specificity could be shown. These results correspond to the hypothesis of Czerniec et al. 22 that patients in the first stages of lymphedema usually show a positive test of water content. In conclusion, patients in stage I to IIb lymphedema who do not have a positive test of water content are likely to have no disturbed lymphatic transport, and if an increased water content is noticed, dermal backflow can be expected.
Lymphedema volume demonstrated a strong agreement with the dorsal forearm and a moderate agreement for the hand and ventral forearm. In these regions, the volume measurement was appropriate to evaluate lymphatic transport. An excellent overall sensitivity for the clinical outcome parameter lymphedema volume was seen. If an increased lymphedema volume is found, presence of dermal backflow can be expected.
In the evaluation of the whole arm, lymphedema excess volume was significantly greater for patients in an advanced stage of dermal backflow (stardust pattern at the upper arm) in comparison with patients in a mild stage of dermal backflow (splash pattern somewhere in the arm).
This study has several strengths. First, all investigators were blinded to the fluoroscopic images. Patients had a wide range of age and BMI, which makes our population representative for all patients with breast cancer-related stage I to IIb lymphedema. A number of six clinical measurements, performed by experienced clinical therapists, were compared to lymphofluoroscopy. Second, each patient completed both the clinical assessment and lymphofluoroscopy, leading to no missing data. Third, the interval between clinical assessment and fluoroscopy had to be a maximum of 3 weeks; however, most examinations were completed in a mean time of only 9.1 days. Fourth, beside the statistical analysis with Cohen's kappa, also, sensitivity and specificity were calculated.
The study has a few limitations. To determine the correlation between lymphofluoroscopy and clinical measurements, dichotomous variables were necessary to make statistics possible. Therefore, cutoff values were installed to be able to formulate the clinical measurements water content and lymphedema volume, which can entail a certain amount of error. Nevertheless, Mayrovitz et al. 23 demonstrated for the water content that a ratio of 1.2 and above could be useful to indicate lymphedema if measured with the MoisterMeterD in women who have previously been surgically treated for breast cancer. For the lymphedema volume, a threshold of 5% was used. Ancukiewicz et al. 24 showed that for the diagnosis of lymphedema, the use of relative arm volume changes (5% or 10%) is preferred. The current study selected a relative arm volume change of 5% as cutoff for the lymphedema volume because an overestimation of lymphedema was more wanted than an underestimation.
The results of the present study indicate that several clinical assessments can be used to assess whether dermal backflow can be expected or not in patients with stage I to IIb lymphedema. The most appropriate clinical measurements to estimate lymphatic transport disturbances are pitting status, skinfold thickness, water content, and lymphedema volume. More specifically, if an increased skinfold thickness, water content, or lymphedema volume is noticed, dermal backflow will most likely be present. If no pitting or increased water content is present, dermal backflow will probably be absent. Assessing the skinfold thickness, pitting status and volume measurements can be performed in clinical practice by the health care provider as an estimation for the disturbance seen on lymphofluoroscopy. Even patients can assess skinfold thickness and pitting status themselves.
For all these clinical assessments, elbow and shoulder region showed a rather bad correlation with the presence or absence of dermal backflow. Therefore, these regions are not appropriate to estimate dermal backflow.
Information about the presence or absence of dermal backflow can be useful in optimization of treatment of BCRL. The lymphatic system is usually damaged by surgery and/or radiotherapy and the lymphatic transport needs to find an alternative pathway. In the treatment of BCRL, it can be necessary to adapt the compression therapy to the patients' specific lymphatic transport. For example, in a patient with dermal backflow of the lower arm and not on the upper arm, an adapted compression garment can be chosen, for example, only compression to the hand and lower arm will be necessary and manual lymph drainage can be adjusted according to the image (fluoroscopy-guided lymph drainage). The remaining lymph vessels will be emptied and a higher pressure will be applied to the area with dermal backflow. When a splash or diffuse pattern is seen, a higher pressure has to be applied than on a splash pattern.
In the current study, only patients with arm lymphedema stage I to IIb were included. Future research should also include patients with lymphedema stage III and patients with lower limb lymphedema. Further, this study only made a difference between dermal backflow or not. Future research should be focused on the gradation of dermal backflow and the clinical assessments of lymphedema.
Conclusions
The study results indicate a correlation between certain clinical assessments and the presence of a dermal backflow pattern visualized during lymphofluoroscopy in patients with BCRL stage I to IIb. Therefore, these clinical measurements can actually be used to obtain more information about dermal backflow in clinical practice. The clinical assessment parameters skinfold thickness, water content, and lymphedema volume seem to be the most appropriate examinations to detect dermal backflow clinically. To confirm the absence of dermal backflow, pitting status is a suitable test.
Footnotes
Acknowledgments
The authors are very grateful to the Universal Hospitals Leuven for collaborating in this study. The authors also extend very grateful thanks to the study participants. All authors critically revised the article for important intellectual content and approved the final article. The study makes part of a double-blind, multicenter, randomized controlled trial (EFforT-BCRL trial), which is registered in ![]() (NCT02609724). CME reference S58689, EudraCT number 2015-004822-33.
(NCT02609724). CME reference S58689, EudraCT number 2015-004822-33.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The EFforT-BCRL trial is financed by the Agency for Innovation by Science and Technology, applied Biomedical Research (IWT 150178).