
Abstract
Background:
The influence of pulsed electromagnetic field therapy (PEMFT) on medium-sized vessels as well as capillary microcirculation is well known. Effects on lymphatic vessels, however, are difficult to visualize and have not been investigated to date. One of the operative treatment options in primary and secondary lymphedemas is lymphovenous anastomoses using supermicrosurgery. To prove patency of the anastomosis, the lymphatic flow is visualized by fluorescence using indocyanine green. The aim of this study was to investigate the influence of PEMFT on the lymphatic microcirculation, and compare it with conventional manual lymphatic drainage (MLD) during supermicrosurgery.
Methods and Results:
Ten patients with lymphedema were included. Indocyanine green was injected before the operation for intraoperative visualization of the lymphatic vessels using a microscope equipped with an integrated near-infrared illumination system (Zeiss). The PEMFT system (Bio-Electro-Magnetic-Energy Regulation [BEMER]) was used as our standard device during a single 2-minute application period (AP) followed by MLD or vice versa.
The mean light intensity in the calibration period (CP) was 46.53 ± 24.3 and 33.41 ± 12.92 for PEMFT and MLD, respectively. During the AP, the mean light intensity changed to 45.61 ± 24.40 for PEMFT and 57.05 ± 18.80 during MLD. This change between CP and AP did not differ significantly for the PEMFT application (p = 0.26), but showed an increase in light intensity during MLD (p < 0.001).
Conclusion:
We found a light intensity enhancement equivalent to a flow increase during MLD of 78.7% ± 45.7% (range 20%–144%) and no significant difference during the PEMFT application. A single period application of PEMFT did not affect the lymphatic flow.
Introduction
Pulsed electromagnetic field therapy (PEMFT) is an established treatment modality used for a variety of indications.1–4 Its mechanism of action is based on the modulation of important cell-repairing cascades, including the CaM complex and nitric oxide (NO) formation.5–8 Thereby, it affects the microcirculation of small capillaries, leading to dilation and increased flow.9–12 These effects have been the basis of many investigations and its clinical use is well described in the literature. In plastic and reconstructive surgeries, however, the characteristics of the lymphatic microcirculation are of similar interest, and due to new treatment modalities, primary and secondary lymphedemas are a topic of growing importance.13–15 Different invasive and noninvasive therapies are available to increase the lymphatic drainage.16–19 With the introduction of supermicrosurgery, lymphovenous shunts (LVSs) can be created to bypass proximally occluded vessels.20,21 In the long term, however, achieving a full remission of lymphedemas is challenging. 22 Therefore, other treatment modalities are in demand and conventional manual lymphatic drainage (MLD) and compression remain important. 23 The influence of PEMFT on the lymphatic system has not been adequately investigated to date. This may be a result of the difficulties involved in noninvasively visualizing and measuring the lymphatic vessels and their drainage. Therefore, the aim of our study was to investigate the influence of PEMFT on lymphatic flow during the surgical procedure of LVSs, and compare its effectiveness with conventional MLD.
Materials and Methods
Patients
This prospective trial was conducted based on ethical approval, and in accordance with the 2010 CONSORT (Consolidated Standards of Reporting Trials) guideline and the Declaration of Helsinki. It was registered in a public German trial registry (DRKS, DRK S000 18800) and approved by the institutional ethics committee (19-1461-101).
One male and nine female patients (mean age: 52 ± 13 years) with compression-refractory lymphedema stadium I–III according to Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) guidelines (I n = 1, II n = 8, III n = 1) were included. 24 Each patient received at least one (range: 1–3) LVS on the distal medial thigh and demonstrated positive indocyanine green (ICG) enhancement during surgery. The cause of lymphedema was primary in four cases and secondary in six cases. Of the six secondary manifestations, five had previously received a Wertheim–Meigs procedure due to uterine cancer, and one patient suffering from rectal cancer received an open abdominoperineal resection. The mean duration of the lymphedema was 11.5 (range 1–26 years), and the mean body mass index of all patients was 26.9 ± 4.7 kg/m2 All participants provided written informed consent for participation in this trial (Table 1).
Patient Demographics and Characteristics
AWMF, Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften; BMI, body mass index; LVSs, lymphovenous shunts.
Surgical technique
All operations were performed by the same senior surgeon with the patient in a supine position under general anesthesia and with blood arrest at the proximal thigh. The superior-edge-of-the-knee incision approach was used in all cases.25,26 Before the operation, 0.2 mL of 0.25% indocyanine green (Verdye 25 mg; Diagnostic Green GmbH, Ascheim-Dornbach, Germany) was injected intradermally into the interdigital space 1–2 and 4–5, as well as ∼10 cm below the superior-edge-of-the-knee incision line. 27 Blood arrest lasted for a maximum of 2 hours and was initiated immediately before surgery. The largest lymphatic vessels above or below the superficial fascia were chosen for the end-to-end lymphaticovenular anastomosis and sutured to suitable veins (11.0 Ethilon sutures; Ethicon™, Somerville, NJ). Before incision of the lymphatic vessel for preparing the anastomoses, measurements including PEMFT application and MLD were performed on the intact vessel. For visualization, an operating microscope equipped with an integrated near-infrared illumination system (OPMI Kinevo Infrared 800; Carl Zeiss, Oberkochen, Germany) was used. 28
Treatment regime pulsed electromagnetic field therapy and manual lymphatic drainage
The PEMFT applicator B.PAD, Bio-Electro-Magnetic-Energy Regulation (BEMER; Innomed International, Triesen, Liechtenstein) was used as our standard device. During application, the program with the highest possible intensity (150 μT) and an interval of 2 minutes was chosen. The applicator was placed along the axis of the treated leg beneath the sterile operating cover. PEMFT application was followed by MLD after a 2-minute pause to prevent an overlapping effect. MLD was performed by gentle bimanual compression starting with the dorsal foot and increasing proximally up to the surgical site.
Indocyanine green videoangiography
After a lymphatic vessel was identified, it was centered in the microscope and a contrast background was placed behind it. The ICG lymphangiography using IR800 (OPMI Kinevo Infrared 800; Carl Zeiss) was started. Each patient received both treatment regimens and separate videos were recorded for each application. For the first 10 seconds of each video, no therapy was applied (calibration period [CP]). Afterward the applications were started (application period [AP]). The first seconds of the AP were considered a transition period and not further analyzed. The video clips were saved for further analysis using the FLOW 800 tool (Carl Zeiss).
Analyzation and statistics
Two regions of interest (ROIs) were set manually in the middle of each lymphatic collector. The light intensity at these positions was measured in arbitrary units every 80 milliseconds. The mean intensity of the two ROIs was calculated for the CP (first 10 seconds), the transition period (seconds 10–20), and the AP (seconds 20–90). The reviewer was blinded. Normality distribution was assessed using the Shapiro–Wilk Test.
A paired t-test was used to analyze the difference between the CP and the AP for each application. Furthermore, the means of the AP were standardized to the means of the CP and compared with a paired t-test for PEMFT and the MLD group.
Statistical analysis was carried out in SPSS 25 for Windows (IBM Corp., Armonk, NY).
Results
The mean light intensities in the CP were 46.5 ± 24.3 and 33.41 ± 12.9 for PEMFT and MLD, respectively (Table 2). During the AP, the mean light intensity for PEMFT changed to 45.6 ± 24.4, and that for MLD changed to 57.1 ± 18.8. There was no statistical difference between CP and AP during PEMFT application (p = 0.26) but for the MLD (p < 0.001) (Fig. 1).
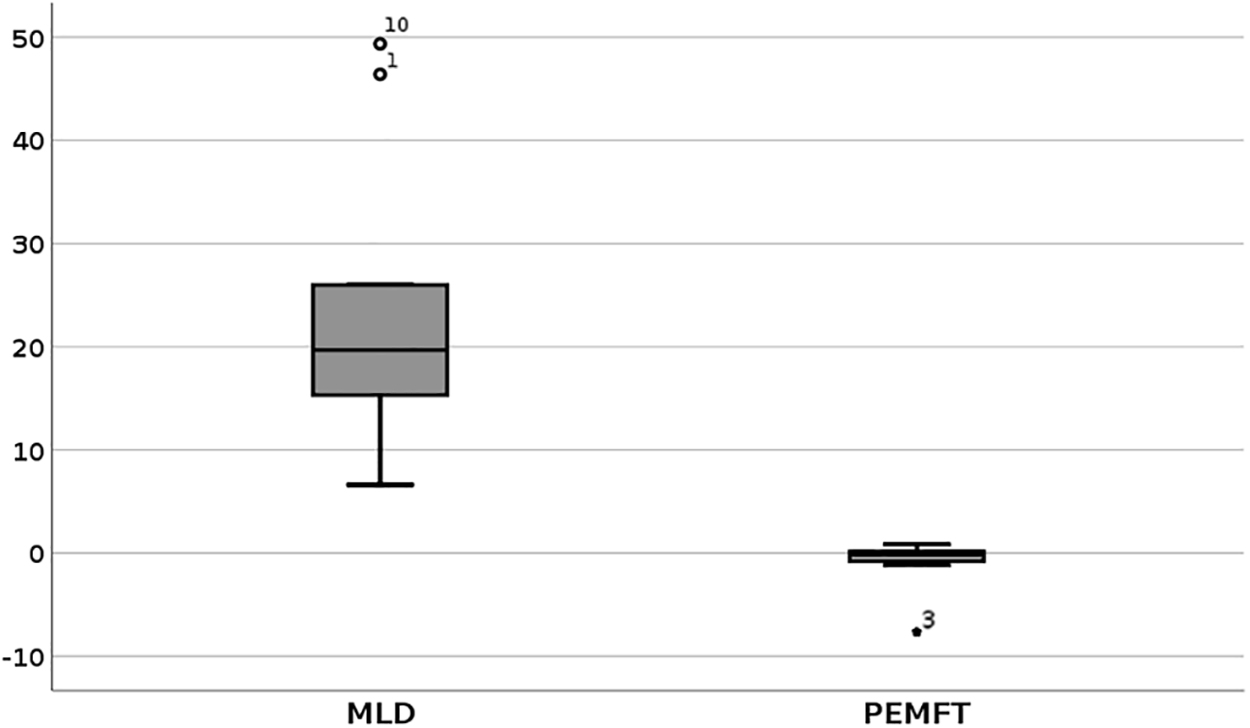
Boxplot showing the absolute change in light intensity in AU between the calibration period and application period for PEMFT and MLD (p < 0.001). Outliers: 1, Patient 1; 3, Patient 3; 10, Patient 10. AU, arbitrary units; MLD, manual lymphatic drainage; PEMFT, pulsed electromagnetic field therapy.
Comparison of Light Intensity in the Calibration Period and Application Period Between Pulsed Electromagnetic Field Therapy and Manual Lymphatic Drainage
AP, application period; CP, calibration period; MLD, manual lymphatic drainage; PEMFT, pulsed electromagnetic field therapy.
The mean absolute difference between CP and AP for MLD and PEMFT was 23.6 ± 14.1 and −0.9 ± 2.5, respectively (p < 0.001) (Fig. 2).
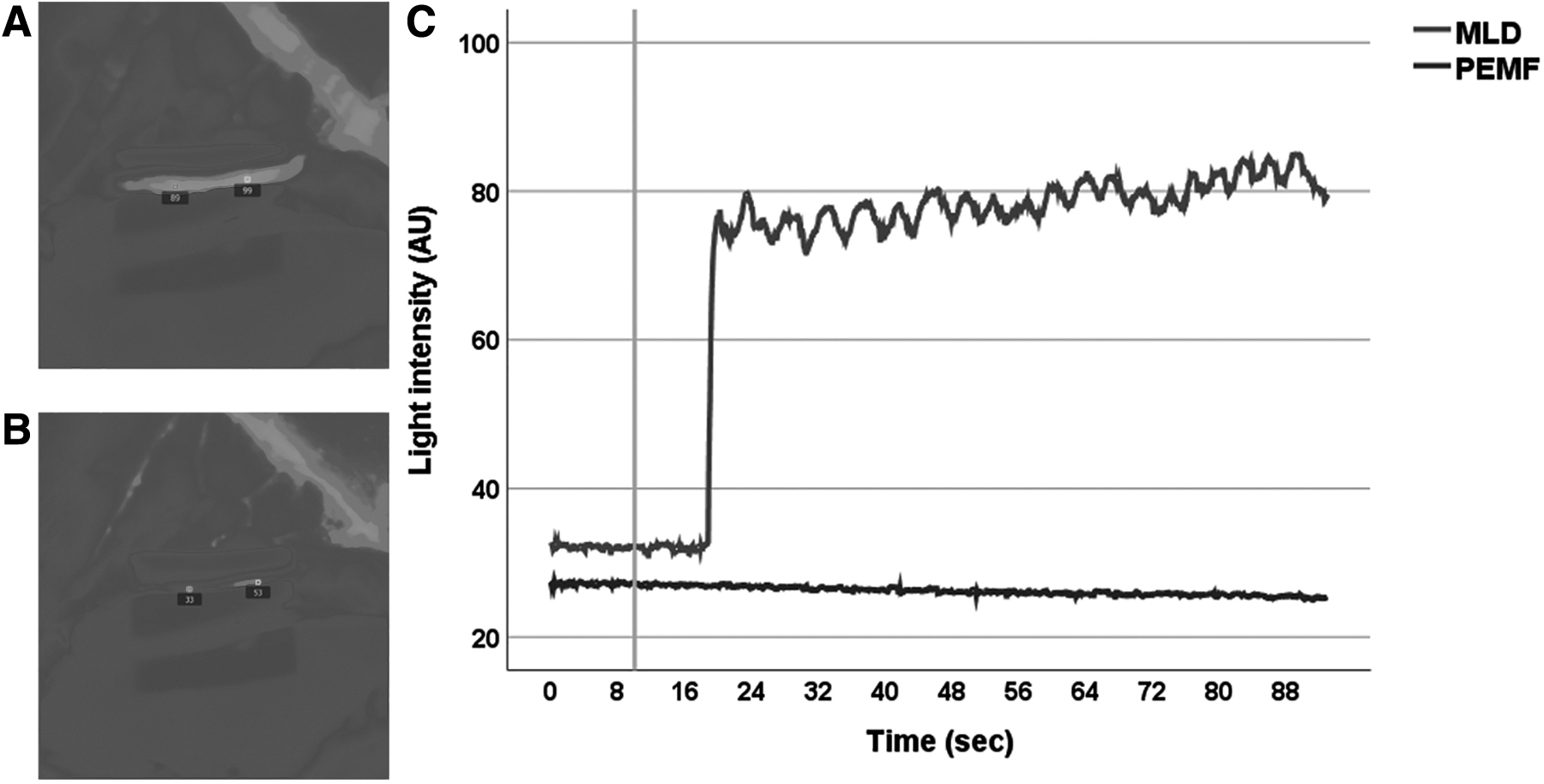
Flow intensity measured on a collecting lymphatic vessel and ROI placement during MLD
The total increase in intensity from the baseline calibration during MLD was 78.7% ± 45.7% (range 20%–144%). During PEMFT application, the intensity decreased by 1.8% ± 5% (range −15% to 3%). The difference was statistically significant (p < 0.001). Individual measuring results and single patient values are displayed in Table 3.
Individual Measuring Results of All 10 Patients During Pulsed Electromagnetic Field Therapy and Manual Lymphatic Drainage
Discussion
Despite the addition of supermicrosurgery to the invasive therapy of lymphedemas, receiving a full remission is challenging and other treatment modalities are of growing interest. PEMFT is used to stimulate the vasomotion by inducing NO formation. We, therefore, investigated the influence of PEMFT on the lymphatic flow during the surgical procedure of LVSs using a fluoroscopic microscope. We found no alteration of the lymphatic flow during the PEMFT application, but a significant difference when compared with conventional MLD. We can, therefore, state that a single use of PEMFT has no significant influence on the lymphatic circulation.
Interpatient variability was assessed by individually comparing the measuring results, but there was no change of conclusion or significance as to the influence of both treatments on the lymphatic flow.
NO is a free radical synthetized by the endothelial NO synthase (NOS) of many vessels and is a major regulator of (micro)vascular function. It exerts a number of pathophysiological actions, including dilation of the capillary smooth vasculature. In the lymphatic network, the endothelial NOS (eNOS) affects the lymphatic fluid velocity mediated by the collecting lymphatics as shown by eNOS inhibition in mice. 29 Therefore, the collecting lymphatics play a physiologically crucial role when evaluating PEMF therapy. However, little is known about the influence of PEMFT-induced NO formation in lymphatics, and many authors focused on the arteriolar and venous capillary system.
Klopp et al. investigated the effects of physical stimulation by PEMFT of arteriolar vasomotion on microcirculation in patients with diabetic wounds. After 27 days of intermitted application with ≤100 μT, they found an increased arteriolar diameter and number of capillary vessels when compared with their control group. 30
Kim et al. focused their research on the systemic influence of PEMFT rather than investigating microcirculatory effects. After 12 weeks of intermitted PEMF therapy (0.22 mT and 30 Hz) to the hands and feet, they found an increased plasma NO availability and a decrease in systemic blood pressure at rest and during exercise in patients with pre-existing hypertension. 31
Bragin et al. measured the microvascular tone and flow velocity in capillaries, arterioles, and venules on the parietal cortex of rats. After 30 minutes of PEMFT (27.12 MHz) application, the tissue oxygenation as well as flow velocity and arteriole diameter increased significantly. Interestingly, vessels with a diameter ranging between 3 and 50 μm were investigated. 32
Thus, PEMF therapy seems to reliably affect NO levels and influences vessels of various diameters. Anatomically, collecting lymphatic vessels show a three-layered wall structure similar to the wall of veins. 33 A smooth muscle layer and intraluminal valves account for the pacemaking activity and lymphatic propulsion. 34 With respect to the undirected application of PEMFT, it seems likely that lymphatic vessels are influenced as well.
However, this finding could not be confirmed by our results since no influence on the lymphatic flow was detected during the application of PEMFT in lymphovenous bypass surgery. A possible limitation of our study might arise from the short and singular application interval of the PEMFT. Nevertheless, Bragin et al. reported an influence of PEMFT on the microcirculation after just 30 minutes of application and no prior exposure. Another possible limitation of our study is the unstandardized MLD. However, the aim of our study was not to analyze the extent of MLD, but to focus on PEMFT application in contrast to a control. As to the significant differences between the groups, the unstandardized MLD seems to be of no consequence for our results.
Conclusion
We attempted to investigate the influence of PEMFT on the microcirculation of collecting lymphatic vessels by direct visualization during lymphovenous bypass surgery. We found a fluorescence intensity enhancement equivalent to a flow increase during MLD, and no significant difference during the PEMFT application. Therefore, short time application of PEMFT has no significant influence on the lymphatic microcirculation. Further studies with prolonged application intervals of PEMFT are thus needed to evaluate the significance of PEMFT as a possible treatment modality.
Footnotes
Author Disclosure Statement
Dr. Taeger and Marc Ruewe are consultants for Carl Zeiss, Germany. Dr. Taeger received compensation for a presentation by BEMER. The BEMER device was provided by the BEMER company free of charge. No competing financial interests exist for the other authors.
Funding Information
No funding was received for this study.