
Abstract
Background:
Vascular endothelial growth factor (VEGF) C156S is an engineering variant of VEGF-C that has the potential to promote lymphangiogenesis, activating on VEGF receptor (VEGFR) 3, without promoting angiogenesis (i.e., not acting on VEGFR-2). We conducted a systematic review of publications assessing the use of this growth factor in lymphedema treatment. We hypothesized that VEGF-C156S specificity for VEGFR-3 was an important differential for the lymphangiogenesis promoted by it.
Methods and Results:
We conducted a comprehensive systematic review of the published literature on PubMed/Medline, Embase, and Cochrane Clinical Answers. Eligibility criteria included articles reporting data on the use of VEGF-C156S in lymphedema treatment. We excluded articles that investigated physiology action of VEGF-C156S and articles that focused on other therapies. From 304 potential articles found in the literature, four studies fulfilled the study eligibility criteria. To date, all studies about this growth factor have been experimental. The effect of VEGF-C156 on lymph node transfer was investigated in half of the experiments. Interestingly, delivery of VEGF-C156S was mostly performed through viral gene transfer, but injection (subcutaneously or intravenously) of it as a protein (liposomal or nonliposomal) was also investigated by one author to assess drug bioavailability.
Conclusions:
Although authors reported promotion of lymphangiogenesis, VEGF-C156S was correlated with lymphatic hyperplasia or nonstatistically significant lymphangiogenesis compared with controls. Scientific evidence about the use of VEGF-C156S in lymphedema treatment is still limited. However, authors have shown that its lymphangiogenic effect is inferior to VEGF-C.
Introduction
Lymphedema is a chronic condition that affects 140–200 million people in the world.1,2 In developed countries, such as the United States, lymphedema is predominantly caused by cancer treatment, with incidences that could reach one in every six patients. 3 Curiously, not all patients with lymphatic injury develop lymphedema, and for those who develop it, clinical manifestations are often only months after the injury. Hence, it has been demonstrated that lymphedema's physiopathology is highly correlated with dysregulation of inflammatory and lymphangiogenic mechanisms.4–6
Studies aiming to develop targeted therapies for lymphedema have been conducted with the rationale of modulating lymphangiogenesis or inflammation and fibrosis.7–9 Use of vascular endothelial growth factors (VEGF) is the main strategy to promote lymphangiogenesis due to their activation of the VEGF receptor (VEGFR) 3 present on lymphatic endothelial cells. 10 Of the VEGF family in mammals, the two main growth factors with an affinity for VEGFR-3 are VEGF-C and VEGF-D. 10 However, both can also stimulate the VEGF-R2, which is the mediator of angiogenic response, developing new blood vessels. 11
To create a VEGF that exclusively activates VEGFR-3 (lymphangiogenesis), scientists proposed a point mutation on VEGF-C, VEGF-C156S, that has attracted attention due to its use as a targeted therapy for lymphedema. 12 Hence, we conducted a systematic review of publications assessing the use of VEGF-C156S in lymphedema treatment. We hypothesized that VEGF-C156S specificity for VEGFR-3 was an important differential for the lymphangiogenesis promoted by it.
Materials and Methods
Search strategy
Two reviewers (D.B. and M.T.H.) conducted independent searches on PubMed/Medline, Embase, and Cochrane Clinical Answers without timeframe limitations, initially through title and abstract screening and then by full-text review. Disagreements regarding article identification and final selection for inclusion of the literature were resolved by another reviewer (A.J.F.). The search was performed using the following keywords: (((Lymphedema) OR Breast Cancer Lymphedema)) AND ((((Vascular Endothelial Growth Factor C156S) OR VEGF-C156S) OR Vascular Endothelial Growth Factor C) OR VEGF-C).
The bibliographies of the studies that fulfilled the study eligibility criteria were also examined, looking for articles not present in our initial search results. This study followed the guidelines outlined in the preferred reporting items for systematic reviews and meta-analyses (PRISMA flowchart in Fig. 1).
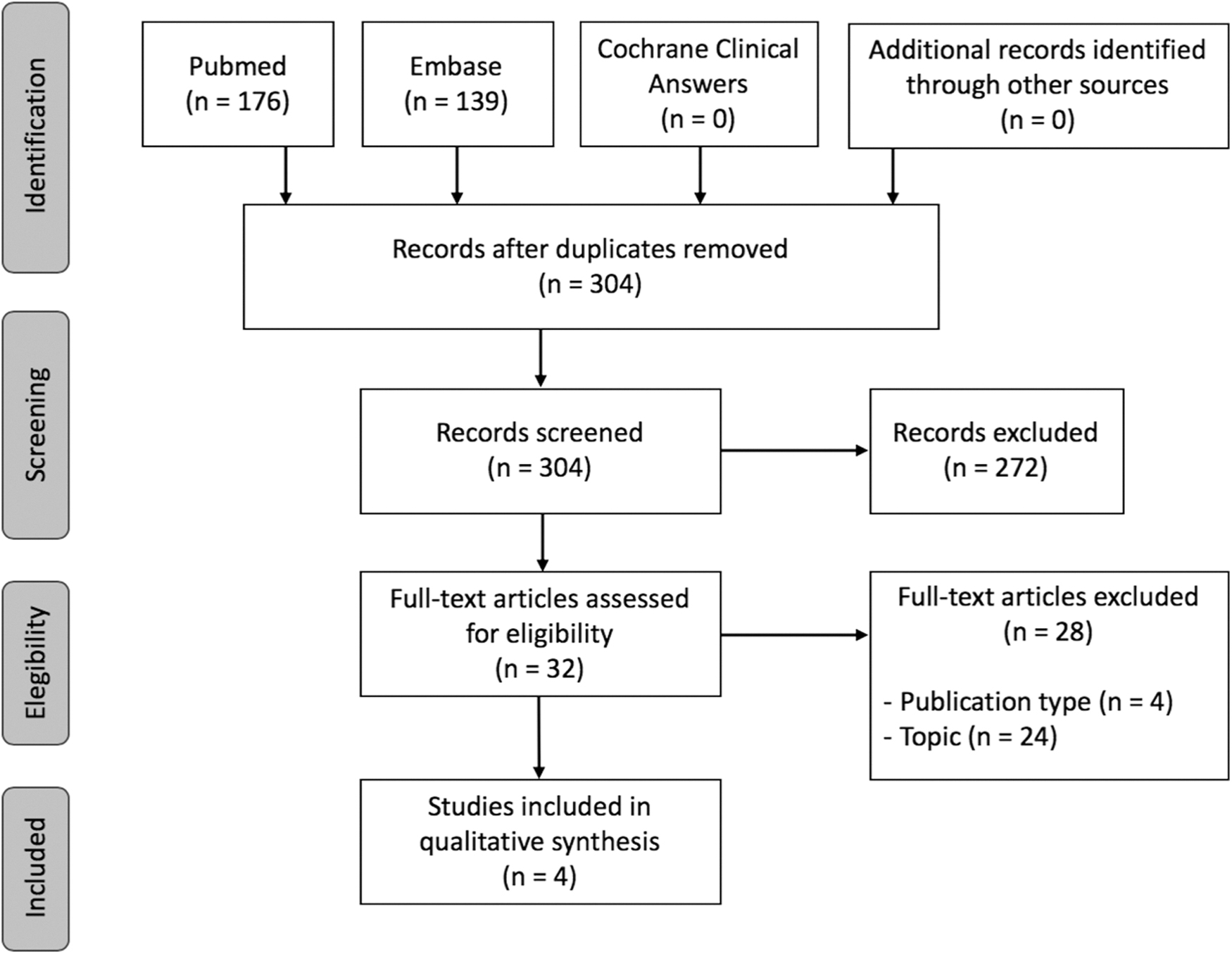
Preferred reporting items for systematic reviews and meta-analyses diagram.
Selection criteria
Eligibility criteria included studies reporting data from the use of VEGF-C156S in lymphedema treatment. Therefore, we excluded articles that investigated the physiological action of VEGF-C156S and those that focused on other therapies. Abstracts, presentations, reviews, and meta-analyses were also excluded.
Data extraction and processing
Extracted data included the year and type of study, country of origin, lymphedema model, mechanism of delivery, targeted tissue, investigated growth factors, and key findings on lymphangiogenic response. Data extraction from articles, tables, and figures was performed by two reviewers (D.B. and M.T.H.), with the accuracy of data entry confirmed by an additional reviewer (A.J.F.).
Results
Study characteristics
Four studies fulfilled the study eligibility criteria from 304 potential articles found in the literature (Fig. 1; Table 1). In 2002, Saaristo et al. 12 were the first to publish on the use of VEGF-C156S as a potential candidate for therapeutic lymphangiogenesis. To date, all studies about this growth factor have been experimental. Most studies were conducted in Finland (3/4) and on mice (3/4). The effect of VEGF-C156 on lymph node transfer was investigated in half of the experiments (2/4). Interestingly, delivery of VEGF-C156S was mostly performed through viral gene transfer (3/4),11–13 but injection (subcutaneously or intravenously) of it as a protein (liposomal or nonliposomal) was also investigated by one author. 14
Summary of the Studies
AAV, adeno-associated virus; IV, intravenous; LNT, lymph node transfer; SC, subcutaneous; VEGF, vascular endothelial growth factor; VEGFR, VEGF receptor.
Viral gene transfer of VEGF-C156S
Saaristo et al. 12 conducted an experiment on mice using viral vectors that they developed to deliver VEGF-C156S, described as a “VEGFR-3–specific mutant form of VEGF-C.” Both adenovirus (i.e., short-term gene expression) and adeno-associated virus (AAV; i.e., long-term gene expression) were used in the study. The authors reported that VEGF-C156S induced lymphangiogenesis in the setting of mouse embryos, normal tissue, and lymphedema tissue.
Lymphatic vessels of normal morphology were notably observed in their lymphedema mice who received AAV, promoting weaker but stable gene expression. As hypothesized, VEGF-C156S did not promote the angiogenic effects observed for VEGF-C. However, VEGF-C156S induced lymphangiogenesis mainly in pre-existing lymphatic vessels (i.e., hyperplasia), whereas VEGF-C promoted the growth of new lymphatic vessels. 12
Two studies assessed the effect of VEGF-C156S on lymph node transfer. Tervala et al. 13 conducted an experiment on mice, investigating the potential of diverse growth factors (VEGF-A, -C, -C156S, and -D) on lymph node transfer using adenoviral vectors. In their experiment, VEGF-C156 improved lymph node survival compared with controls, but its lymphangiogenesis was moderate and not statistically significant. In contrast, VEGF-C promoted lymph node survival, growth of new lymphatic vessels, and improvement of lymphatic vessel function, and, therefore, was considered the better VEGF therapy. 13
Visuri et al. 11 conducted their experiment on a pig model of secondary lymphedema, where they assessed the effect of adenoviral delivery of VEGF-C156S and VEGF-C on lymph node transfer. In their study, both growth factors promoted the growth of new lymphatic vessels; however, VEGF-C156S lymphangiogenesis was not statistically significant compared with the control group (LacZ). In contrast, VEGF-C promoted significantly stronger lymphangiogenesis and increased the number of vessels connected to the transferred lymph nodes. Importantly, although VEGF-C promoted enlargement of the blood vasculature, adverse effects such as wound exudate (increased vascular permeability) were not noted. 11
Delivery of VEGF-C156S as a protein
Bhansali et al. 14 conducted an experimental study on mice to investigate whether the route of administration of VEGF-C156S protein (subcutaneous vs. intravenous) and protein liposomal encapsulation would impact lymph node exposure to this growth factor. Analysis of lymphangiogenesis was not reported in the study. Using a radiolabeled VEGF-C156S with iodine-125, they demonstrated that, compared with the intravenous route, the subcutaneous route promoted a prolonged exposure of the lymph node to the growth factor, regardless of its encapsulation into liposomes. Therefore, the use of liposomal VEGF-C156 did not improve bioavailability compared with its nonliposomal form. 14
Discussion
To our knowledge, our study is the first systematic literature review investigating the use of VEGF-C156S in lymphedema treatment. In this study, we demonstrated that, to date, only four experimental studies have shed light on the use of VEGF-C156S in lymphedema treatment. Delivery of this growth factor was mainly proposed through viral gene transfer that varied among study protocols, using adenovirus or AAV.11–13 Only one study used a proteic form of VEGF-C156S for delivery, investigating the impact of different routes of administration and liposomal packing on the bioavailability of the growth factor. 14
Although VEGF-C156S has the potential to exclusively induce lymphangiogenesis without activating angiogenic receptors (e.g., VEGFR-2), the in vivo lymphangiogenesis induced by this factor was correlated only with lymphatic hyperplasia or presented nonstatistically significant results compared with controls. Tervala et al. 13 compared the effect of VEGF-C, VEGF-D, VEGF-C156S, and VEGF-A on lymph node transfers using the mice secondary lymphedema model.
It was observed in their study that VEGF-C–treated animals had the greatest results. 13 Visuri et al. 11 reported that its lymphangiogenesis induced by VEGF-C156S was not statistically significant compared with the control group on lymph node transfers in a pig model of secondary lymphedema. In the same study, VEGF-C-treated pigs presented the strongest lymphangiogenesis and an increase of the vasculature supply of the transferred lymph nodes. 11
Additional studies investigated the lymphangiogenic effect of VEGF-C and other lymphatic growth factors. A study performed by Anisimov et al. 15 aimed to investigate the long-term effects of VEGF-C and VEGF-D in skeletal muscle cells on mice. They determined that VEGF-C has a stronger activation of the lymphangiogenesis receptors VEGFR-2 and VEGFR-3 in comparison with VEGF-D. 15 Lahteenvuo et al. 16 investigated the utilization of VEGF-D and VEGF-C on transplanted lymph nodes in pigs. It was demonstrated that VEGF-C has a higher lymphangiogenesis potential compared with VEGF-D.
Of note, VEGF-C did not induce seroma as initially expected because of its activity on angiogenic receptors. 16 A similar result was found in the study performed by Visuri et al. 11 wherein the enlargement of the blood vasculature promoted by VEGF-C through activation of VEGFR-2 was not enough to cause adverse effects such as wound exudate on pigs. Hence, VEGF-C is still considered the ideal growth factor candidate to therapeutic lymphangiogenesis.11–13
Our study has limitations typical to systematic reviews, such as the possibility of bias in interpreting the data presented in each article. Nonetheless, our systematic review reports a high-yield summary of the scientific evidence related to the use of VEGF-C156S in lymphedema treatment that may guide future studies. Even though current data pointed out that VEGF-C seems to have a stronger lymphangiogenic potential, we encourage further studies investigating the efficacy and safety of using VEGF-C156S in lymphedema treatment.
Conclusions
Scientific evidence for the use of VEGF-C156S in lymphedema treatment, to date, is based on experimental studies with heterogeneous protocols. Although authors reported that VEGF-C156S promoted lymphangiogenesis, it was correlated with lymphatic hyperplasia or nonstatistically significant lymphangiogenesis compared with controls. Thus, although VEGF-C is still the ideal growth factor candidate to induce lymphangiogenesis, further studies are needed to elucidate the benefits and safety of VEGF-C156S on patients with lymphedema.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Mayo Clinic Center of Individualized Medicine and Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery.