
Abstract
Background:
Lack of diagnostic awareness of lipedema and frequent confusion with obesity or lymphedema may be an obstacle for treatment. The clinical effects of conservative treatment methods are not clearly known. This study investigated the effects of exercise-based rehabilitation combined with complete decongestive therapy (CDT) or intermittent pneumatic compression therapy (IPCT) or alone in patients with severe lipedema.
Methods:
Thirty-three women with severe (type 3, stage III or IV) lipedema diagnosed according to the revised-Wold criteria were randomized into three groups: Group 1 (CDT plus exercises), Group 2 (IPCT plus exercises), and Group 3 (control—exercises alone). All groups received 30 sessions of combined (aerobic, strengthening, and stretching) exercise program. In addition, there were CDT in Group 1 and IPCT in Group 2 five times a week for 6 weeks. The primary outcome measure was the limb volume measurements. The secondary outcome measures were anthropometric measurements (body weight, body mass index, waist-to-height ratio, waist-to-hip ratio), 6-minute walk test, visual analog scale for pain, fatigue severity scale, Beck Depression Inventory, and Short Form Health Survey-36 (SF-36).
Results:
Thirty-one participants completed the interventions. Limb volumes (p = 0.017, ηp2 = 0.562 for right; p < 0.001, ηp2 = 0.775 for left), pain (p = 0.045, ηp2 = 0.199), and physical functioning subscore of SF-36 (p = 0.040, ηp2 = 0.465) differed significantly between treatments originating from Group 1.
Conclusions:
All programs improved outcome measurements after the intervention. However, when the difference between treatments was investigated, CDT administered in addition to the exercises has been shown to provide significant improvements in reducing limb volumes, pain, and physical function.
Clinical trial registration number:
The study was registered at the US National Institutes of Health (ClinicalTrials.gov) (NCT03924999) and available at https://clinicaltrials.gov/ct2/show/NCT03924999?term=lipedema&draw=2&rank=6
Introduction
Lipedema is a chronic, progressive, and hereditary adipose tissue disorder characterized by an abnormal increase of subcutaneous adipose tissue, especially in the lower extremities. It is thought to affect ∼11% of women in adulthood all over the world.1–3 Lipedema is often seen in female sex, and usually begins in the period of hormonal change in adolescence or after a few years. Bilateral symmetrical swelling, pain spontaneously or with palpation, and easy development of ecchymosis of the legs are the main determinants of lipedema. 4
Lipedema is often not diagnosed due to lack of awareness of the physicians. Furthermore, it can be evaluated as obesity and lymphedema. Patients with lipedema, who are said to be obese, are directed to strict diet and exercise, but weight loss is from the upper extremity and trunk, which are nonlipedematous areas.3,5,6 Although lymphatic dysfunction is a common finding in advanced stages, there are many distinctive features between lymphedema and lipedema.2,4,6
There are accepted clinical diagnostic criteria for the diagnosis. It is divided into five types depending on the fat distribution. In type 1, pelvis and hips; in type 2, from hip to knee; in type 3, from hip to ankle; in type 4, arms; and in type 5, lower limbs are affected. 6 Pain is seen in 70% of patients in the affected areas. Although the cause of the pain is unknown, it has components seen in central sensitization and chronic pain syndrome. 7 It is often accompanied by fatigue and loss of physical condition.5,6
Four morphological stages have been defined. In stage I, the skin surface is normal; the adipose tissue is increased and may contain small nodules. In stage II, a larger fat mass and nodular changes are observed in the subcutaneous tissue. In stage III, there are symmetrical large fat lobules and skin folds around the medial knee, lateral hip, and ankle. In stage IV, lipedema is accompanied by lymphedema (lipolymphedema). 6
Treatment for lipedema includes conservative and surgical options. In conservative treatment, a holistic approach is required, involving patient education, diet, physical activity, manual lymphatic drainage (MLD), compression therapy, methods of coping with pain, and psychological support.5,8
Although there is no definite exercise prescription for lipedema, physical activity with moderate intensity (60% to 70% of age adjusted predicted maximum heart rate) is recommended. It helps maintain weight control and increase mobility as well as mental well-being. 9 Also, staying active in lipedema is important for the movement of lymph fluid. 10 In patients with lipedema, volume reduction may not be associated with exercise in lipedematous areas. 11 In this case, the main component of treatment is complete decongestive therapy (CDT). Especially if lymphedema is accompanied and skin folds are present, MLD and bandaging with multilayered short-stretch bandages before compression clothes can be beneficial in reducing pain, tenderness, and limb volumes. If CDT modalities cannot be applied or are not sufficient, intermittent pneumatic compression therapy (IPCT) can be used. 12
The hypothesis of this study is that exercise-based rehabilitation combined with CDT will lead to greater improvements in limb volumes, anthropometric measurements, functional capacity, pain, fatigue, depression, and quality of life than exercise-based rehabilitation combined with IPCT or alone in patients with severe lipedema. Therefore, the aim of this study was to compare the effects of exercises combined with CDT or IPCT or alone in patients with severe lipedema.
Materials and Methods
Study design
The study was designed as a single-center, prospective, single-blinded, randomized controlled trial. The study protocol was approved by the Institutional Human Research Ethics Committee (approval number: 19-KAEK-062). All the procedures were conducted according to the Declaration of Helsinki. This study was also registered in the ClinicalTrials.gov database (NCT03924999). The reporting was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) and recommendations for randomized trials. Participants were fully informed about the experimental procedures and gave their informed consent.
Participants and assessments
Participants with diagnosis of lipedema were recruited from the physical medicine and rehabilitation outpatient clinic. Patients who were willing to participate in the study were assessed to evaluate their eligibility for the study and to provide detailed information about the study. The inclusion criteria were as follows: (1) ≥18 years, (2) female sex, (3) diagnosed with lipedema according to the criteria of revised Wold. 13 These criteria include disproportionate body fat distribution, no or limited influence of weight loss on fat distribution, limb pain and bruising, increased sensitivity to touch or limb fatigue, nonpitting edema, and no reduction of pain or discomfort with limb lift. (4) Lipedema type 3 and stage III or IV. 6 (5) No participation in a designed sports or exercise training programs within the last 3 months. (6) No pregnancy or breastfeeding. Patients were excluded if they had comorbid inflammatory/connective tissue diseases, cardiovascular or musculoskeletal problems that could prevent them to participate in an exercise program. During the study, patients were not allowed to change the drug doses they used for pain. The study began on April 2019 and ended on November 2019.
The patients were randomized into three groups: Group 1 (CDT plus exercises), Group 2 (IPCT plus exercises), and Group 3 (control—exercises only). Randomization was done by using a computer program that included a randomized table of numbers, which was created by an independent individual who was not involved in the recruitment and treatment of patients. Numbered cards with a random assignment and information about the group allocation in opaque, sealed envelopes were prepared by the independent individual. The certified therapist opened the envelope and applied the procedure according to randomization group.
Interventions
Complete decongestive therapy
Group 1 had 30 sessions of CDT, which consisted of MLD, skin care, and compression bandaging, five times a week for 6 weeks. The MLD technique involved stationary circles, pumping, scooping, and rotary movements with varying degrees of light pressure. After MLD, compression bandaging with multilayered short-stretch bandages was applied. The bandage was kept 23 hours and replaced the next day after exercise program. CDT was provided by a certified lymphedema therapist. 12
Intermittent pneumatic compression therapy
Group 2 had 30 sessions of IPCT, which consisted of applying the device (I-tech lymphopress 4, Martellago (VE), Italy) 30 minutes with a setting of 50 mm Hg pressure, five times a week, for 6 weeks.14,15
Exercise training
All participants followed the same standardized exercise training and intensity protocols 5 days a week, for 6 weeks. Each exercise session consisted of 5–10 minutes active warmup, including flexibility exercises; 20–25 minutes submaximal aerobic exercise with treadmill training; 10–15 minutes of strengthening exercises where major muscle groups were strengthened through shoulder press, dumbbell press, shoulder elevation with resistance, biceps curl, squats, hip flexion and extension, and standing hip exercises using 1–3 kg of weight loads and 1 set of 8–10 repetitions and a 5–10 minute cool-down involving stretching by holding the main muscle-tendon groups for 20–30 seconds, with 4–5 repetitions for each muscle group. Aerobic exercise intensity was adjusted according to 6-minute walk distance (6MWD). Heart rate achieved at the end of the 6-minute walk test (6MWT) was regarded as the target heart rate. This exercise intensity was submaximal, and the heart rate and blood pressure were measured during training sessions, and treadmill speed was tailored to reach the target heart rate. Maintenance of the heart rate during training sessions was important both for providing the similar exercise intensity for each patient.16,17 All exercise sessions were supervised by the same physiotherapist.
The patients in Group 1 were wearing compression bandages during exercise. The patients in the other group did not have anything except the knee brace.
Outcome measures
All participants evaluated pre- and postintervention by a single investigator who was blinded to the allocated intervention. Baseline demographic (age, height, weight, body mass index, education level) and clinical characteristics (duration of disease, stage of disease, level of physical activity according to the International Physical Activity Questionnarie 18 ) of the patients who met the initial screening criteria were recorded. Outcome measurements were made at the same time of the day. The evaluation included anthropometric measurements, limb volume measurements, 6MWT, visual analog scale for pain, fatigue severity scale (FSS), Beck Depression Inventory, and Short Form Health Survey-36 (SF-36).
Number of sessions, total duration of aerobic exercise, and duration of maximum aerobic exercise were also recorded to determine compliance with the training program between the groups.
Primary outcome
Limb volume measurements
Limb volume measurements were chosen as the primary outcome measure. Circumference measurements were taken at 4 cm intervals up the limb, from the ankle to the thigh. Pythagorean theorem in the excel program will automatically calculate limb volume measurements. 19
Secondary outcomes
Six-minute walk test
The 6MWT is a submaximal exercise test usually corresponding to 80% of a subject's maximum heart rate, and is used to assess functional capacity and treatment response. Standard instructions were used, and 6MWD was recorded. 20
Visual analog scale for pain
Pain intensity was measured with visual analog scale for pain (0–10 mm; 0 means no pain, 10 means severe pain), which is used to measure musculoskeletal pain with very good reliability and validity. 21
Fatigue Severity Scale
The FSS assesses the severity of fatigue during the last week in a 9-item questionnaire (1 = strongly disagree, 7 = strongly agree). Total score ranges from 9 to 63, with higher scores representing greater fatigue. 22
Beck Depression Inventory
The BDI is a 21-item self-report questionnaire evaluating the presence and severity of depressive symptoms in the vegetative, emotional, cognitive, and motivational domains. Scores for each item range from 0 to 3; higher scores mean higher risk of depression. 23
Short Form Health Survey-36
SF-36 contains 36 items, which are used to evaluate the quality of life of patients with chronic pain. It measures eight different domains that address physical functioning, physical role limitation, pain, general health, vitality, social functioning, emotional role limitation, and mental health. The score of each domain ranges from 0 (worse quality of life) to 100 (best quality of life). 24
Sample size
The sample size estimation was performed using the G Power software (v 3.1). It was determined that 10 individuals for each group must be recruited to detect a difference at 5% type 1 error level with 80% power for an effect size of 0.467 based on the lower extremity limb volume reported in the previous research conducted by Szolnoky et al., evaluating the CDT alone or combined with IPCT in women with lipedema. 8 However, including ∼10% for possible future losses, 11 individuals were allocated in three groups.
Statistical analysis
Demographic data and clinical features were presented as mean and standard deviation (SD). Categorical variable was presented as number (n) and percentage (%). Visual assessment and Shapiro–Wilk test were used for normality evaluation. All continuous variables were normally distributed. A 3 (group) × 2 (time) mixed factorial analysis of variance with repeated measures was used to assess the study outcomes. Post hoc comparisons were done with the Bonferroni test. The effect size was calculated by the partial eta squared (ηp 2 ) value. Effect size values were interpreted as follows: >0.2, large effect size; >0.1, medium effect size; and >0.05, small effect size. Data analyses were performed using IBM SPSS (Statistical Package for Social Sciences) Statistics for Windows, Version 21.0, and p ≤ 0.05 was considered a statistically significant difference.
Results
The CONSORT diagram for participants is shown in Figure 1. Ninety-two individuals were assessed for eligibility, and 33 met the inclusion criteria and enrolled in the study. Two of them lost to follow-up, and 31 participants completed the program. Demographic and clinical variables did not show any significant difference between the three study groups such as age, height, weight, BMI, and education level (all p > 0.05). No significant differences were found in the mean duration of disease, lipedema stage, International Physical Activity Questionnaire total score, right/left limb volume, and volume difference between both limbs between the three groups of patients (all p > 0.05) (Table 1).
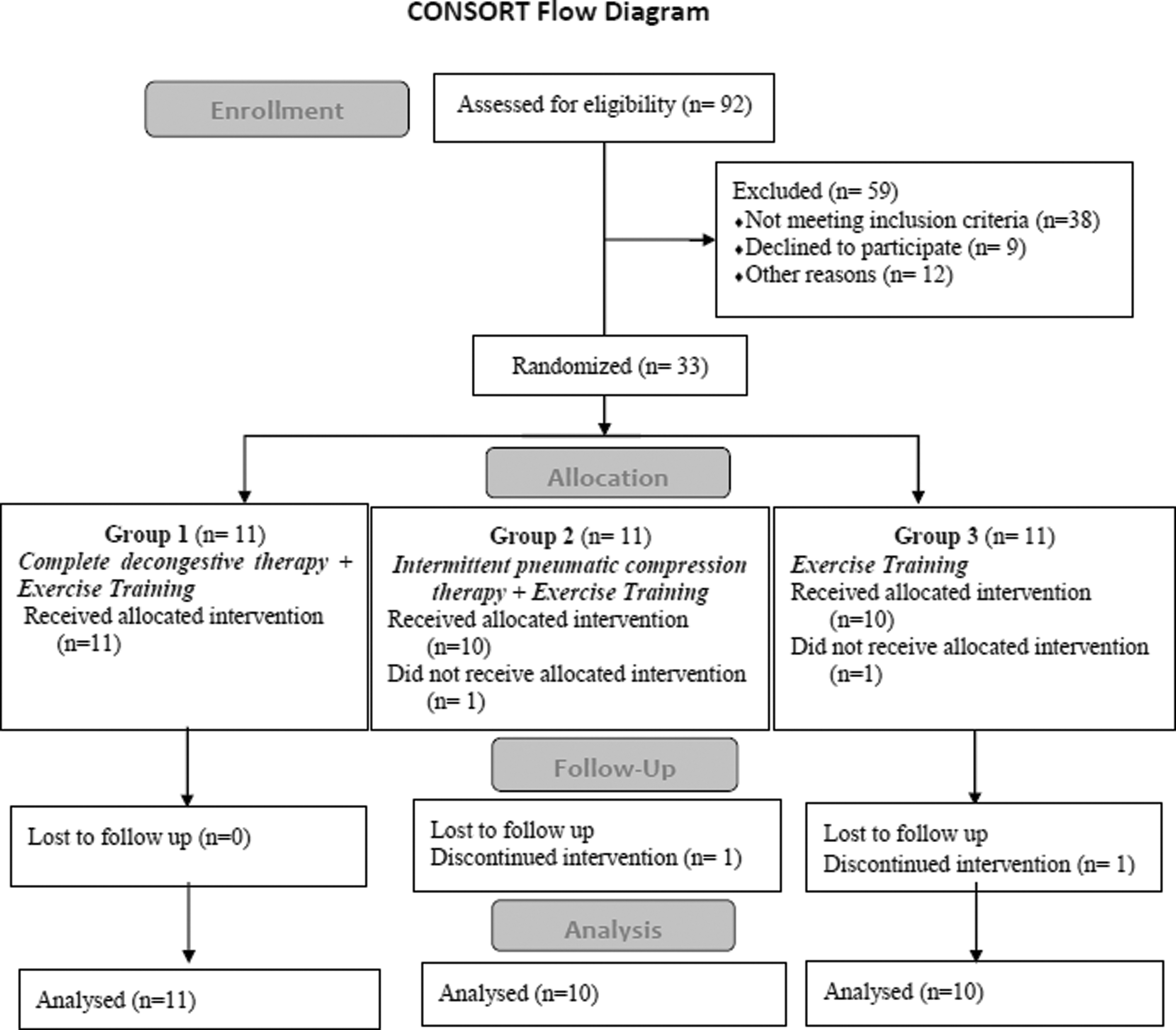
Flow diagram of the study.
Patient Characteristics of the Study Groups
Group 1: CDT plus exercises group, Group 2: IPCT plus exercises group, and Group 3: control, exercises-only group.
BMI, body mass index; CDT, complete decongestive therapy; IPAQ, International Physical Activity Questionnaire; IPCT, intermittent pneumatic compression therapy; SD, standard deviation.
The anthropometric measurements of body weight, body mass index, waist-to-height ratio, and waist-to-hip ratio did not differ between treatments (all p > 0.05) but changed over time (all p < 0.001), except for waist-to-hip ratio (p = 0.980) (Table 2).
Within- and Between-Group Changes (Group, Time, and Interaction Effects) for Primary and Secondary Outcome Measurements
Group 1: CDT plus exercises group, Group 2: IPCT plus exercises group, and Group 3: control, exercises-only group.
Data expressed as mean (standard deviation), ηp 2 = partial eta-squared, effect size.
p-Value for basal measurements among the three groups.
p-Value for pre- and postintervention measurements for each group.
Significant p-values (p < 0.05) are indicated in bold and adjusted for Bonferroni correction.
6MWD, 6-minute walk distance; BMI, body mass index; SF-36, Short Form Health Survey-36; VAS, visual analog scale.
A significant group effect, time effect, and interaction effect were found for the right and left limb volumes as our primary outcome measurement (group effect: p = 0.017, p < 0.001, respectively; time effect: p < 0.001 for both; interaction effect: p = 0.001, p < 0.001, respectively). Effect sizes were large regarding treatments, time, and interaction. The difference between treatments was originating from Group 1 (p < 0.001 for both) (Figs. 2 and 3).

The difference between treatments for the right limb volume.

The difference between treatments for the left limb volume.
The 6MWD did not differ between treatments (p = 0.943) but changed over time (p < 0.001). There were no significant changes regarding the interactions between groups (p = 0.554). Effect sizes were small regarding treatments and interaction, but large for time.
A significant group effect (p = 0.045), time effect (p < 0.001), and interaction effect (p = 0.029) were found for the pain. Effect sizes were large regarding time and interaction, but medium for treatments. The difference between treatments was originating from Group 1 (p = 0.05, Fig. 4).

The difference between treatments for the pain measured by VAS. VAS, visual analog scale.
The FSS and beck depression inventory (BDI) did not differ between treatments (p = 0.118, p = 0.341, respectively) but changed over time (p < 0.001 for both). There were no significant changes regarding the interactions between groups (p = 0.622, p = 0.243, respectively). Effect size was small regarding interaction, but large for time.
The SF-36 subgroups did not differ between treatments except for physical functioning (p = 0.040) but changed over time usually. Effect sizes were large regarding treatments and time for physical functioning and pain subscores. A significant interaction effect was found for only role limitations due to physical health (p = 0.028).
Training sessions were well tolerated, and no adverse events were observed except mild pain in the lower extremities. The compliance with the training program determined by mean number of sessions, mean duration of aerobic exercise, and mean duration of maximal aerobic exercise was similar among the groups (all p > 0.05) (Table 3).
Features of Completed Training Sessions
Group 1: CDT plus exercises group, Group 2: IPCT plus exercises group and Group 3: control, exercises-only group.
Discussion
The main findings from this study reinforce the recommendations that lipedema patients should perform structured exercises, particularly performed at a moderate intensity, to improve anthropometric measurements including limb volumes, functional capacity, pain, fatigue, depression, and quality of life. All of the groups showed improvements over time in most outcome measures. One of the findings supported the hypothesis that the limb volume measurements showed more significant decrease for CDT group compared with other two groups. Similar findings were observed for pain and SF-36 subgroup of physical functioning.
There is no targeted therapeutic treatment for patients with lipedema, since etiological factors have not been fully established. 25 The goal of the treatment is to improve psychosocial status, quality of life with regression of symptoms, and prevent secondary complications such as lymphedema.2,3 Treatment options should be arranged according to the severity of the disease, the patient's complaints and expectations in the light of current guidelines. 26
The main treatment methods are CDT and surgical interventions. CDT is necessary and useful, especially in cases of lipolymphedema. It is not surprising to use CDT and IPCT treatments based on the link between lymphatic dysfunction and adipose hypertrophy.8,27 CDT in lipedema consists of MLD and compression treatments. MLD has been reported to reduce pain and discomfort in pure lipedema patients. 8 In an uncontrolled study, a 10% reduction in leg circumference was achieved with compressive therapy in lipedema women.8,12
In this study, when the limb volumes were compared between three groups after treatment, CDT plus exercises were found superior. However, when the pre- and postintervention measurements were compared, a significant improvement was found also in IPCT plus exercises and exercises-only groups.
Pneumatic compression devices do not reduce adipose tissue alone, but they can increase mobility by reducing edema and pressure in lipedema. Nevertheless, they can also increase pain due to the sensitivity of patients with lipedema. However, in this study, not an increase in pain, but rather a significant reduction was achieved in the IPTC plus exercises group. In addition, when the treatments for pain relief were compared, the CDT plus exercises group was superior.
In a study by Szolnoky et al., no additional benefit of IPCT added to CDT was found in women with lipedema. IPCT has not been shown to be superior to MLD, but it may benefit in cases where MLD is not applicable. 8 According to the results of this study, IPCT applied in addition to exercises was not superior to the exercises-only group in patients with severe lipedema.
Lipedema is a chronic condition, and decreased activity in patients results in loss of muscle strength. Daily activities can be highly affected in advanced stages. 28 Decreased physical activity leads to an increase in body mass index and lipedema. In this study, when the characteristics of the patients were examined, the body mass index of the patients in all groups was similarly high, and their physical activity levels were low. In a study, quadriceps muscle strength was found to be less in individuals with lipedema than in obese.29,30 Moderate-intensity physical activity is aimed at preventing or reducing these conditions.31–34 In addition, exercise programs that increase muscle strength should be designed. Flexibility exercises are also designed to increase the reduced range of motion. 29
To the best of our knowledge, this is the first single-blinded randomized controlled trial that analyzes the effects of supervised exercise sessions combined with CDT or IPCT in patients with severe lipedema. When the outcome measures determined for this study were examined, improvements were achieved in all three groups in terms of weight control, limb volumes, functional capacity, pain, fatigue, depression, and quality of life. Importantly, interventions were well tolerated, and participants reported few adverse events such as muscle or joint pain. Although participants had severe lipedema, adherence to the treatments was high in all groups.
Study limitations
As a limitation of this study, the follow-up period was short for understanding the maintenance of the long-term effects of interventions. Further studies are necessary to determine the long-term effects of interventions in subjects with lipedema. Another limitation of the study is that the target group only included stages III and IV. In future studies, it can be investigated whether the treatments will have an effect on early stage (stages I and II) patients. In addition, only clinical diagnostic criteria for lipedema were used in this study. Stage 4 lipedema was detected with a positive “stemmer sign.” In future studies, some delayed lymphatic flow and increase in lymphatic pooling can be detected with lymphoscintigraphy due to the mass effect of adipose tissue.
Conclusions
As a result, 30 sessions of CDT plus exercises, IPCT plus exercises, and exercises only were found beneficial in severe lipedema treatment; among them CDT was found to be superior to others. CDT improved limb volumes, pain, and physical functioning more than other treatment methods. Planning the appropriate treatment by predicting the needs of the patient should be the main target in this patient group.
Footnotes
Acknowledgments
The authors thank all participants of this study and lymphedema therapist Esin Çatakkaya for providing treatments for the participants.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.