
Abstract
Background:
As survival from malignancies continues to improve, a greater emphasis is being placed on the quality of life after cancer treatments. Lymphedema (LE) represents a common and devastating sequela of neoplastic therapies, even if its incidence in patients submitted to lymphadenectomy for prostatic cancer is still poorly documented. The purpose of the current study was to analyze the imaging findings provided by noncontrast magnetic resonance (MR) lymphography in secondary lower limb LE related to prostate cancer therapies.
Methods and Results:
Patients with diagnosed secondary LE related to prostatic cancer treatment who underwent noncontrast MR lymphography (NCMRL) between November 2019 and February 2020 were assessed. Image datasets were retrospectively reviewed for the severity of lymphedema and characteristics of the subcutaneous tissue, muscular compartment appearance, number of iliac and inguinal lymphatics, and number of locoregional lymph nodes. Ten patients with 17 affected lower extremities, nine right extremities, and eight left extremities were included in our analysis. Magnetic resonance imaging grading was classified as one in four extremities, two in five extremities, and three in eight lower extremities. Honeycomb pattern was observed in 15 extremities, without significant correlation with MR grading (p = 0.684); dermal thickening showed correlation with MR grading (p < 0.001), as well as reduction of muscular trophism (p = 0.021). We observed a significant correlation between the number of inguinal lymph nodes and recognizable inguinal lymphatics (p = 0.039).
Conclusion:
NCMRL is able to provide useful information for the management of secondary lower limb LE caused by prostate cancer treatments. Clinical Trials.gov ID: n.2019/ST/187
Introduction
As survival from malignancies continues to improve, a greater emphasis is being placed on the quality of life after cancer treatments. 1 Lymphedema (LE) represents a common and devastating sequela of neoplastic therapies.
LE consists of the accumulation of interstitial fluid into the soft tissues, resulting from a disproportion between lymph production and its transport into the circulatory system, conditioning swelling, chronic inflammation, tissue fibrosis, and progressive anomalous fat deposition. 2 LE can be classified into two types: primary and secondary. The first one is rare, mainly related to a congenital impairment of the lymphatic system, involving the lymphatic vessels and/or lymph nodes, and further divided according to the age of appearance 3 ; the latter is due to the damage of a preexisting normal lymphatic system. In Western countries, secondary LE is mostly caused by malignancies, due to neoplastic infiltration or surgical or radiation cancer-directed treatments. 4
The incidence of postcancer treatment LE varies broadly, according to the extension of the lymphadenectomy and additional treatments. A few old data are available on the incidence of LE postlymphadenectomy for prostatic cancer,5–7 ranging from 0% to 10%, 7 with the extension of lymph nodes removal.
LE is a chronic disabling condition that markedly affects patients' quality of life. Its treatment has traditionally been conservative, involving manual lymphatic drainage and compression therapies. However, in recent times, surgical options have gained a role in LE management: reconstructive treatments (lymphaticovenular anastomosis and vascularized lymph node transfer) and reductive techniques (debulking/excision and liposuction). 8
LE diagnosis is based on patients' history and clinical examination. No consensus about which imaging technique should be used for the diagnosis, staging, and follow-up of LE exists.
Lymphoscintigraphy is the most diffused examination to study LE: It provides functional information, such as the transit time of the tracer and dermal backflow, 9 but it is limited by the ionizing exposure, low spatiotemporal resolution, long acquisition times, and invasiveness due to intradermal or subcutaneous injection of the radiotracer.
Magnetic resonance imaging (MRI) has gained a role in the LE study. In a noninvasive way, MR can provide information about the composition of the swollen limbs 10 and is a useful tool in follow-up after LE treatments. 11 The MRI can be executed with or without contrast medium administration.
Contrast-enhanced magnetic resonance lymphangiography (CEMRL) is performed through subcutaneous injection of gadolinium-based contrast medium in the interdigital web spaces of feet or hands; it has been proved to be a safe technique, with high spatial resolution and is able to provide a good visualization of the lymphatic drainage and nodal uptake.12,13 However, the procedure of injecting contrast medium in the interdigital spaces and the long acquisition times can cause patients discomfort, especially in case of very young patients affected by primary LE.
The use of heavily T2-weighted acquisitions, which are able to highlight the signal of static or slow-moving fluid-filled structures, such as the lymphatics, with suppression of the background signal, in the MR protocols, allows obtaining information on peripheral and main lymphatic vessels, as described in protocols of noncontrast MR lymphography (NCMRL), without the administration of any contrast media.14,15 This technique does not provide functional information regarding the timing of the lymphatic drainage and has limited spatial resolution for the evaluation of distal lymphatic vessels, but the non-need to administer contrast medium allows its use in allergic and pediatric patients, with lower costs, when compared with CEMRL. 14
The purpose of our study was to describe the characteristics of secondary LE due to prostate cancer therapy on NCMRL.
Materials and Methods
This study received approval from our Institutional Review Board (Comitato Etico Milano Area 1) with protocol number 47437/2019. Patients provided written informed consent.
Consecutive male patients studied were included according to the following criteria: history of prostatic cancer treatment, previously submitted to extended pelvic lymphadenectomy, secondary LE diagnosed according to clinical evaluation, and patients' history by a plastic surgeon and a physician, both experienced in LE, in consensus, execution of NCMRL between November 2019 and February 2020; exclusion criteria were a history of primary lower limb LE, and contraindications for MRI execution.
MR examination
Patients were asked to remove the compressive bandages/stockings 24 hours before the exam, to avoid an underestimation of the LE that could be associated to the compressive treatment removal just before the examination.
All NCMRLs were executed on a 1.5-T MR magnet (MAGNETOM Avantofit; Siemens Medical Systems, Erlangen, Germany), with a 36-channel peripheral angiographic coil and an 8-channel phased-array body coil on the lower abdomen, with patients placed in the supine position with the feet first. 16
Five hundred milliliters of pineapple juice were administered 30 minutes before the examination to decrease bowel content signal intensity, and patients were asked to empty the bladder just before the exam.
The acquisition was performed in different steps to cover the anatomical stations of the lower limbs, the groin, and the pelvis.
The examination consisted of a heavily Fast Spin Echo T2-weighted coronal 3D lymphographic sequence, with the following acquisition parameters: repetition time (TR) 2870 mseconds, echo time (TE) 797 mseconds, and field of view (FOV) 380 × 380 mm; matrix 358 × 384; slice thickness 1 mm, without gap, and a coronal 3D STIR with the following acquisition parameters: TR 3000 mseconds, TE 254 mseconds, inversion time 160 m, and FOV 460 × 504 mm; matrix 315 × 384 pixel; and slice thickness 1 mm, without gap.
The images were postprocessed with multiplanar reconstructions or with a maximum-intensity projection algorithm.
Image analysis
Each dataset including postprocessed MR images was archived and analyzed on our PACS system (Carestream Health, Rochester, NY), by two radiologists in consensus. The agreement was reached by consensus. Imaging analysis was performed for each affected extremity.
According to a previously proposed classification for lower limb primary LE, which was proved to significantly correlate with the clinical staging, 15 LE was staged as grade 1, 2, and 3. 1, if: superior border of subcutaneous infiltration was recognizable below the knee, fluid infiltration of subcutaneous fat was mild, nonconditioning resulted in a dimensional increase of subcutaneous fat, and epifascial fluid collection thickness was <5 mm (Fig. 1). 3, if: subcutaneous infiltration involved the whole lower limb, fluid infiltration was severe and resulted in a dimensional increase of subcutaneous fat, and epifascial fluid collection thickness was >15 mm (Fig. 1). Stage 2 corresponded to an intermediate situation between grade 1 and 3.

Heavily T2-weighted sequence showing mild bilateral fluid infiltration of both legs, without dimensional increase. A thin epifascial fluid collection is visible on the medial aspect of the left leg.
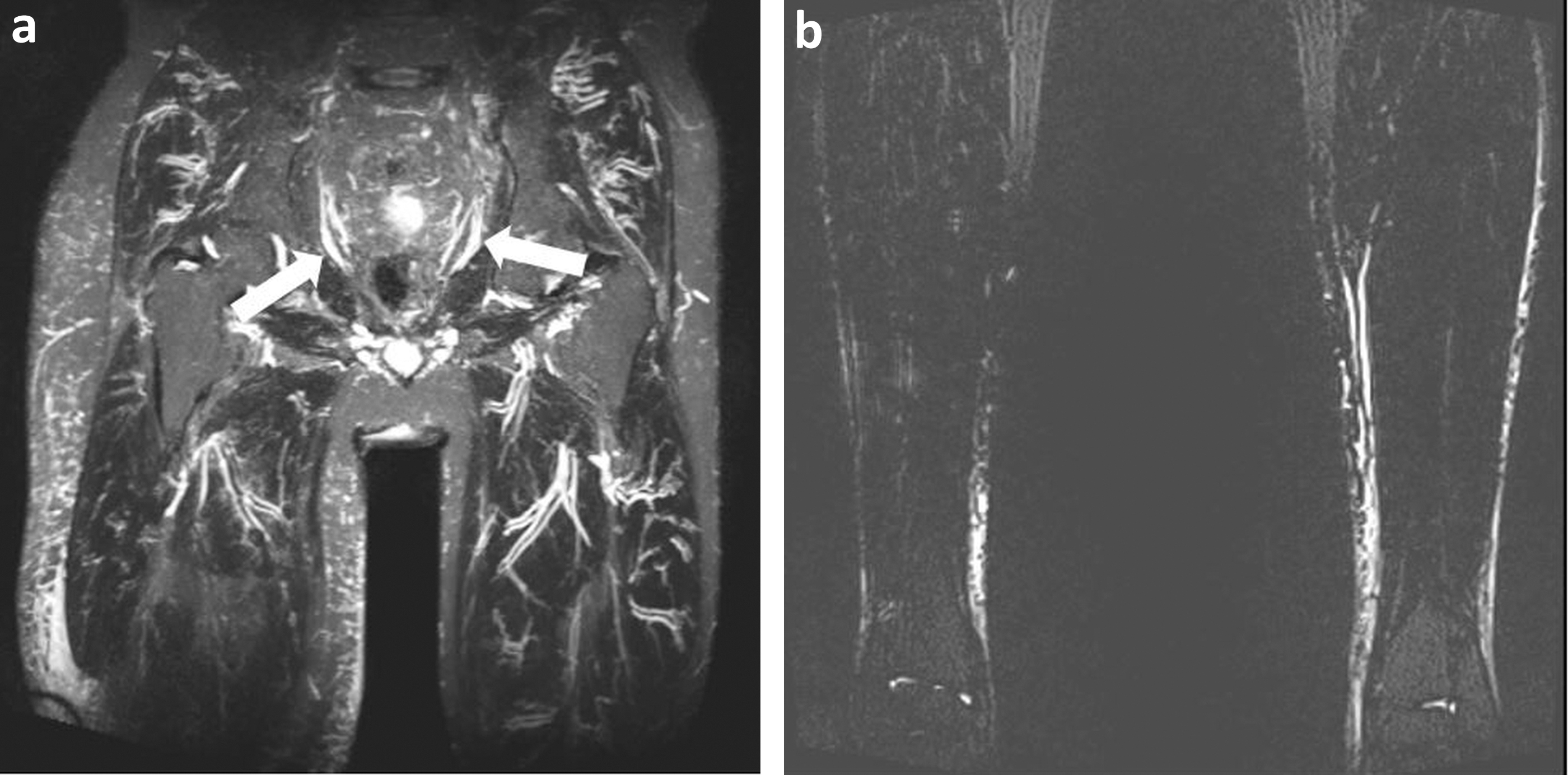
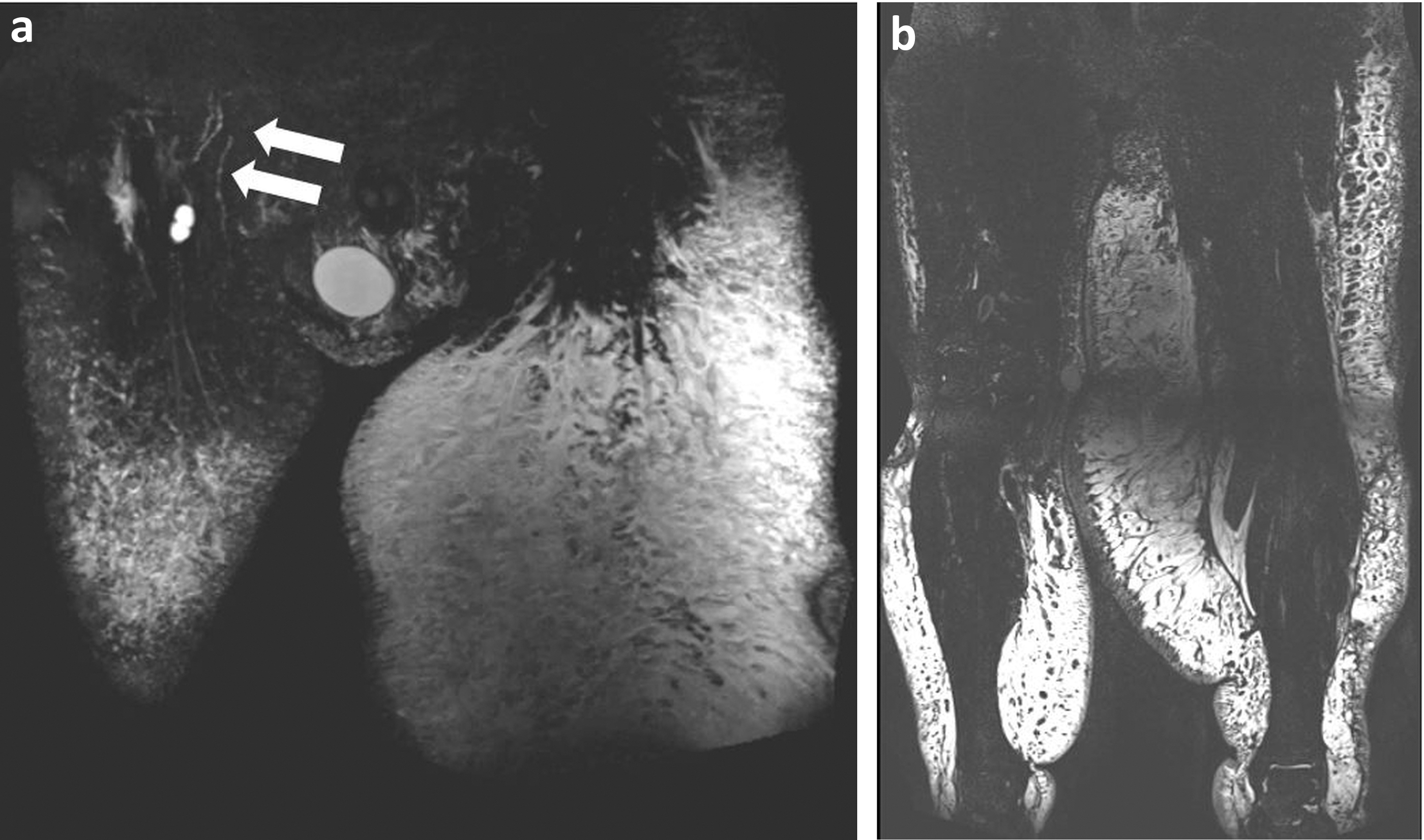
For each examination, we assessed the following imaging findings 15 : the honeycomb pattern of the subcutaneous fat (Figs. 2 and 3), consisting of enlarged fat pockets, bordered by trabecular/reticular structures; the thickening of dermis (>2 mm) (Fig. 4), impaired trophism of the muscular compartment (Fig. 5), the number of inguinal and iliac lymph nodes (Fig. 6), the number of visible inguinal and iliac lymphatic trunks, and the presence of dilated distal lymphatic vessels (>1 mm).
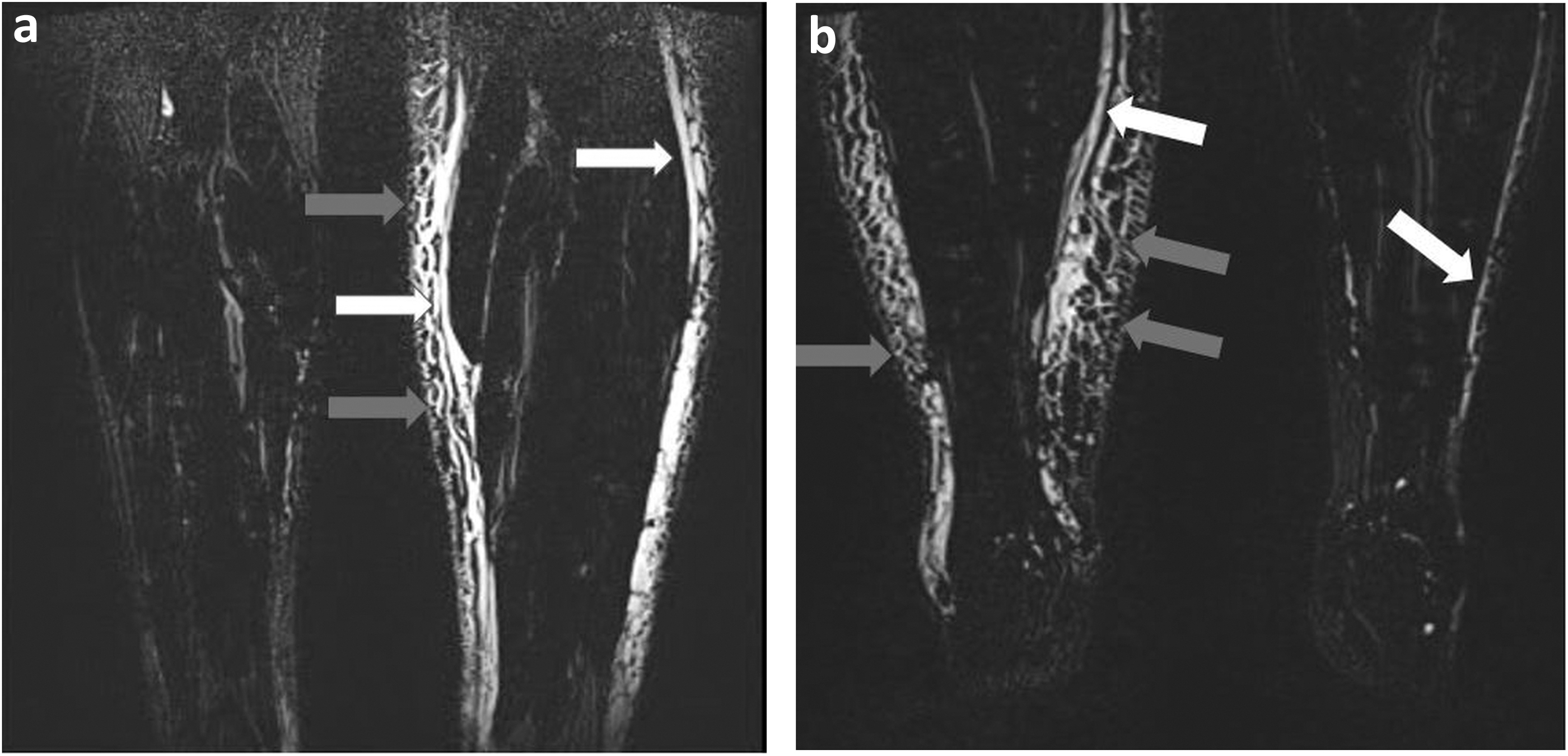

Bilateral evidence of diffused honeycomb pattern, with almost symmetrical distribution and increase of the leg size.
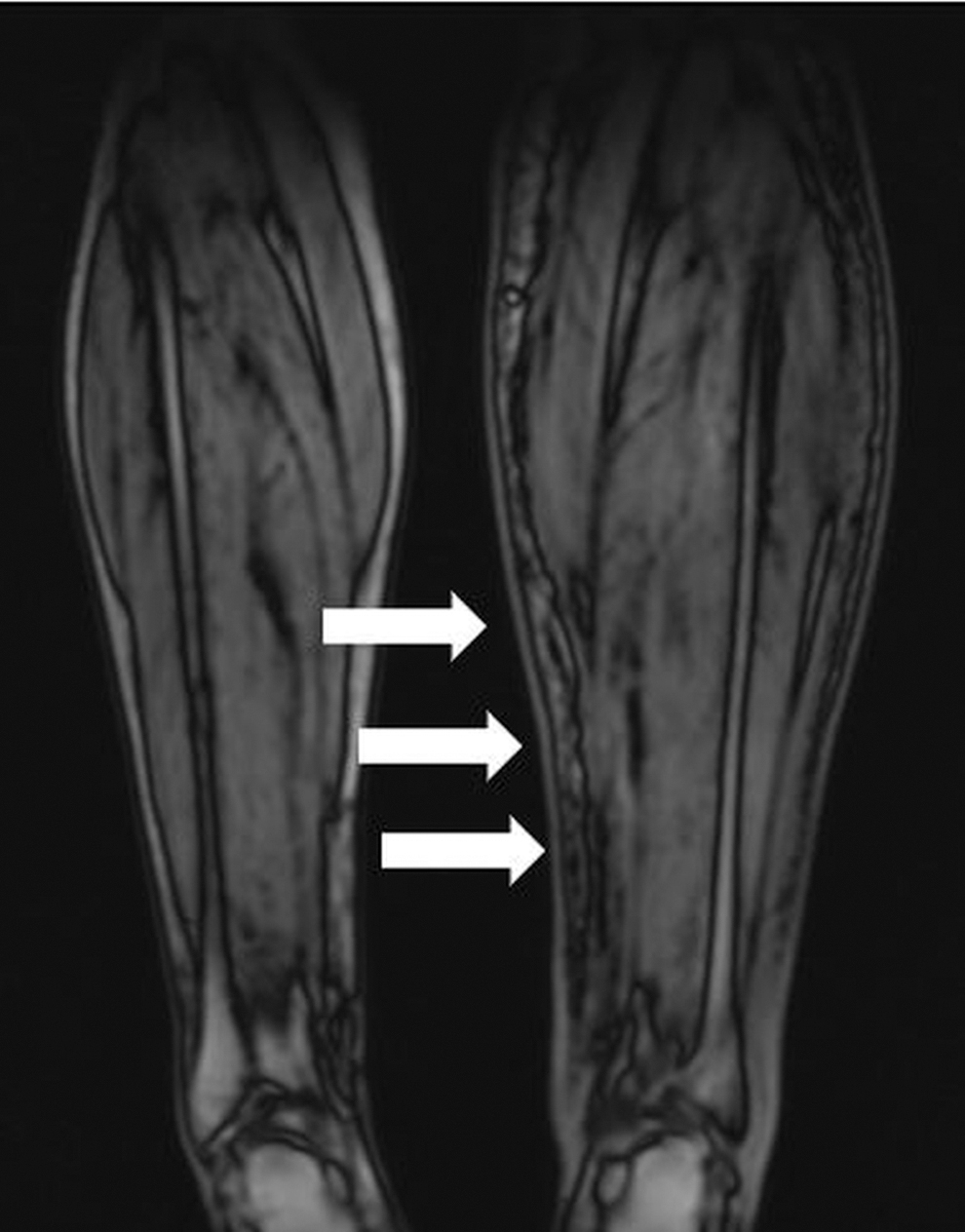
Presence of dermal thickening on the left leg (white arrows).
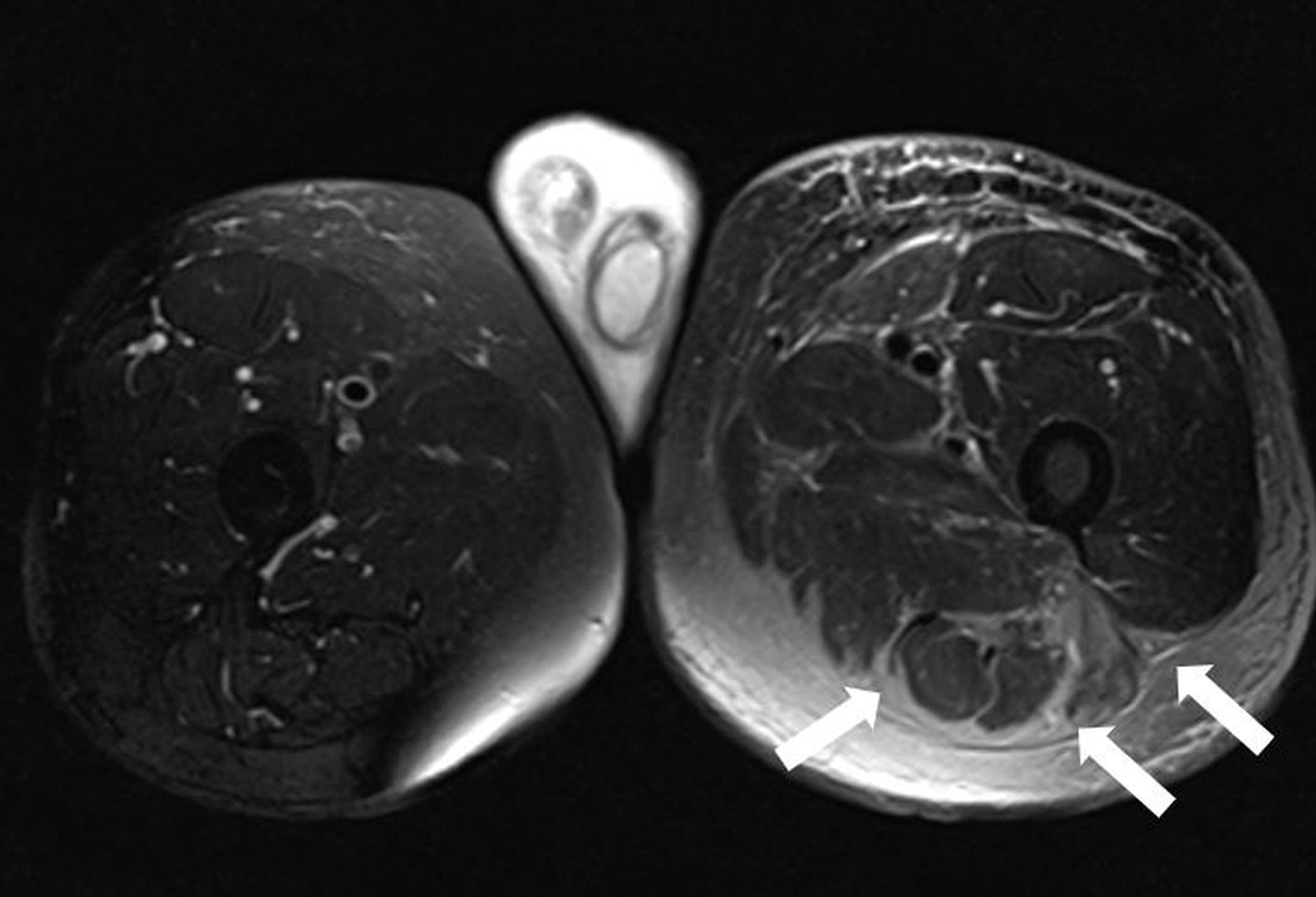
Postprostatic cancer unilateral left LE, with evidence of increased fat representation within the subfascial compartment (white arrows) on the left side.

Bilateral evidence of inguinal lymph nodes (white arrows).
Statistical analysis
MRI grading and MRI characteristics were checked for normality with the one-sample Kolmogorov–Smirnov test. Correlations between values were evaluated through two-tailed Pearson's Correlation Coefficient. Anova test was used to evaluate differences between independent groups. p < 0.05 was regarded as statistically significant. Statistical analysis was performed by using SPSS 20 (IBM, Chicago, IL).
Results
Ten patients (mean age: 66.1 ± 5.2 years; age range: 56–75 years) were enrolled. All patients had a history of prostatic cancer with the American Joint Committee on Cancer (AJCC) stage IV A. 17
Seven out of 10 patients (70%) were affected by bilateral LE, two patients had right LE (20%), and one patient had left LE (10%).
Mean swelling duration was: 3.8 ± 2.2 years; mean timing of post-treatment LE development was: 6.0 ± 3.0 months.
Seventeen lower extremities were included in our analysis, nine right extremities and eight left extremities.
In 6 out of 7 (85.7%) patients with bilateral LE, the swelling included the groin and the genital regions. In 5 out of 7 (71.4%) patients, the limb swelling was asymmetrical.
The mean examination duration was 38 minutes. MRI grading was classified as one in four extremities, two in five extremities, and three in eight lower extremities.
Honeycomb pattern was observed in 15 out of 17 (88.2%) extremities; 10 out of 17 (58.8%) limbs showed dermal thickening; and in 6 out of 17 (35.2%) extremities, a mild reduction of muscular trophism was found.
The observations of honeycomb pattern of the subcutaneous fat, of dermal thickening, and of reduced muscular trophism divided for MRI grades are reported in Table 1.
Number of Imaging Features Divided for Different Magnetic Resonance Imaging Grades
MRI, magnetic resonance imaging.
The statistical correlations between the different MRI findings and MRI grading are listed in Table 2.
Statistical Correlation Between Imaging Findings and Magnetic Resonance Imaging Grading
No statistically significant difference was found between MRI grading and the number of iliac lymphatics (Fig. 7) (p = 0.369) or inguinal lymphatics (Fig. 8) (p = 0.395).
Inguinal lymph nodes were: 3.1 ± 2.8 for each side. We observed a significant correlation between the number of inguinal lymph nodes and recognizable inguinal lymphatics (p = 0.039).
No iliac lymph node was observed; therefore, the correlation with the number of iliac vessels was not performed.
No correlation was found between the honeycomb appearance of the fat tissue and swelling duration (p = 0.612).
We did not observe dilated distal lymphatic vessels in this group of patients.
Discussion
We reported the information obtained from the NCMRL study of secondary LE related to prostate cancer treatment.
To the best of our knowledge, there is no study in the literature regarding the imaging features in patients previously treated for this kind of tumor.
On NCMRL, lower limb LE is characterized by fluid infiltration of subcutaneous fat and epifascial fluid collection: These aspects allow the differential diagnosis from adipose infiltration due to lipoedema and obesity. 15
Honeycomb pattern represents one of the typical imaging features of LE15,18: This aspect has been explained as trabecular structures with enlarged fat pockets surrounded by lines corresponding to fluid or fibrous tissue or both, 19 or as the accumulation of fluid between fat surrounded by fibrotic tissue. 20 The possible role of both fluid infiltration and fibrosis can explain its presence in all MR grades, without a statistically significant difference.
We observed a honeycomb pattern, regardless of the duration of the limb swelling, unlike the study of Haaverstad et al., who described this finding only in LE lasting more than 1 year. 21 According to our experience, the honeycomb pattern mostly related to fluid can explain its presence in the early phase of the disease; whereas the development of inflammatory cells in the dermis and proliferation of collagen fibers that progressively increase as the LE worsens can explain the honeycomb in long-lasting LE.
The thickening of the dermis is another imaging feature of LE and can be explained by local inflammatory cells appearance with progressive fibrotic changes. In our case series, the dermal thickening correlated with the MR grading.
The reduced trophism of the muscular compartment was slight, without any signal abnormalities of the muscle, and correlated with MRI grading. This evidence can be explained by the reduced mobility of the affected extremity. The study by Hoffner et al. instead described the presence of subfascial fat in the lymphedematous limbs that were not changed by liposuction. 11
We did not observe any statistical correlations between the number of lymphatic iliac and inguinal vessels and imaging grading.
In the study on primary lower limb LE by Arrivé et al., LE was observed in 46% of aplastic lymphatics patterns, defined as absent visualization of main lymphatic truncks, 37% in hyperplasic lymphatics pattern, when more than 6 lymphatic trunks or when lymphatic trunks with caliber ≥3 mm were visible, and in 15% in hypoplasic patterns (visibility of fewer than three lymphatic trunks). Therefore, also in this study, there was no evident correlation with the number of lymphatics: Both in the absence and in anomalous increase of the lymphatic vessels number, the disorder manifested. 15
To the best of our knowledge, no study analyzed a possible correlation between the number of recognizable lymphatics trunks at MR and the grading of LE.
The absence of dilated peripheral vessels may be related to the limited case series analyzed, as they were observed in other case series of patients affected by lower limb secondary LE. 22
The diagnosis of LE is usually based on the clinical examination and patient's history, especially when dealing with secondary LE, and can result in unrecognition of mild LE. 18 The best imaging technique for LE evaluation has not yet been established. In comparison to other imaging techniques used for LE assessment, such as lymphoscintigraphy, NCMRL has the advantage of noninvasiveness, as no injection of any contrast media is required, and no radiation exposure is involved in the acquisition. As a single examination, this recently introduced imaging technique can provide information about the enlargement and the appearance of the subcutaneous fat, the grade of the epifascial fluid collections, the trophism of the muscular compartment, the number of inguinal and pelvic lymph nodes, and the characteristics of the lymphatic vessels. This information is useful in the patient's management and follow-up.
Even if the most diffused LE therapeutic approach is still conservative, including bandages and compressive techniques, new surgical options have been gaining importance: the lymph node transplantation for lymphatic reconstruction and lymphatics-venous anastomoses. The first one could be more appropriate for aplastic or hypoplasic LE, whereas the latter is appropriate in case of hyperplasic LE. An assessment of lymphatics number is needed for the right treatment planning.
In clinical settings, the evolution of LE and the response to treatment is still determined by limb circumference measurements, without any evaluation of the composition of the enlarged extremities.
Therefore, NCMRL could be useful for establishing the best management and could represent a noninvasive objective technique to assess the therapeutic efficacy.
This is a preliminary study including a limited number of patients. Further studies with wider case series are needed to confirm our results. Moreover, we have to consider the intrinsic limitation of NCMRL, which is limited spatial resolution. 15 The continuous evolution of MR equipment will contribute to a progressive improvement of this technique.
In conclusion, we described imaging data that can be provided by NCMRL in a noninvasive way and that can be useful for the management of secondary LE related to prostate cancer.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.