
Abstract
Background:
Lymphedema is characterized by an accumulation of interstitial fluids due to inefficient lymphatic drainage. Primary lymphedema is a rare condition, including congenital and idiopathic forms. Secondary lymphedema is a common complication of lymph node ablation in cancer treatment. Previous studies on secondary lymphedema lymphatic vessels have shown that after an initial phase of ectasia, worsening of the disease is associated with wall thickening accompanied by a progressive loss of the endothelial marker podoplanin.
Methods and Results:
We enrolled 17 patients with primary and 29 patients with secondary lymphedema who underwent lymphaticovenous anastomoses surgery. Histological sections were stained with Masson's trichrome, and immunohistochemistry was performed with antibodies to podoplanin, smooth muscle α-actin (α-SMA), and myosin heavy chain 11 (MyH11). In secondary lymphedema, we found ectasis, contraction, and sclerosis vessel types. In primary lymphedema, the majority of vessels were of the sclerosis type, with no contraction vessels. In both primary and secondary lymphedema, not all α-SMA-positive cells were also positive for MyH11, suggesting transformation into myofibroblasts. The endothelial marker podoplanin had a variable expression unrelatedly with the morphological vessel type.
Conclusions
: Secondary lymphedema collecting vessels included all the three types described in literature, that is, ectasis, contraction, and sclerosis, whereas in primary lymphedema, we found the ectasis and the sclerosis but not the contraction type. Some cells in the media stained positively for α-SMA but not for MyH11. These cells, possibly myofibroblasts, may contribute to collagen deposition.
Introduction
Lymphedema is a progressive invalidating condition of the lymphatic system characterized by an abnormal accumulation of interstitial fluid with subsequent inflammation, adipose tissue hypertrophy, and fibrosis. The resulting swelling of the affected regions can cause disfigurement as well as functional impairment and invalidity and predisposes to recurring severe infections and the possibility to develop rapidly progressing sarcomas. Overall, lymphedema and its complications have a heavy impact on the patient's quality of life, with great costs for the health care system. 1
Lymphedema (OMIM#53100) may be primary or, more frequently, secondary. Primary lymphedema (PL) is a rare condition mainly affecting the lower limbs. Based on age of onset, primary lymphedemas have long been classified as congenital when present at birth, praecox, with onset around puberty, and tarda, with onset after 35 years. However, since lymphedema may occur with early and late onset also within the same family, a more exact classification should refer to the molecular defect. 2
Several mutations have been identified in different genes such as FLT4 on chromosome 5 (Milroy's disease, by far the most common), FOXC2 on chromosome 16q24 (lymphedema distichiasis syndrome), GJC2 on chromosome 1, VEGFC on chromosome 4 (Milroy-like disease), PIEZO1 on chromosome 16, and EPHB4 on chromosome 7. 2 In all those cases in which no genetic diagnosis is available, lymphedema is called idiopathic. 3 Secondary lymphedema (SL) is more frequent and results from the disruption or obstruction of a normal lymphatic system mainly due to cancer treatment (i.e., surgical removal of lymph nodes); in tropical countries it may also be caused by obstruction of lymphatic collecting vessels by parasites (filariasis). 4
In previous studies on secondary lymphedema,5,6 the lymphatic collecting vessels have been reported to be initially dilated (ectasis type) and subsequently progressively constricted by thickening of their wall, eventually leading to lumen obstruction. Collecting vessels with a thickened wall have been classified as “contraction type” when the wall thickening was due to an increase in smooth muscle cells (SMCs) and as “sclerosis type” when it was caused by collagen fibers. Moreover, while the endothelium of the collecting lymphatic vessels of normal and ectasis types was found to be positive for the endothelial marker podoplanin, the contraction type was found slightly positive and the sclerosis type negative. 5
Management of lymphedema includes manual lymph drainage, exercise, and the use of compression garments. These methods avoid progression of the disease, reduce swelling, and prevent infections, but do not solve the problem. Among the surgical therapeutic approaches, there is a supermicrosurgical technique of creating multiple lymphaticovenous anastomoses (LVA)7–9 between collecting vessels and veins allowing lymph discharge into the blood stream. These anastomoses are preferentially performed distally to the obstruction (i.e., in the hand, wrist, or elbow), where lymphatic vessels are presumably still functioning.
The present study was designed to improve understanding of the morphologic changes that occur in the wall of collecting vessels in primary compared with secondary lymphedema. Results showed a marked wall thickening in most of the collecting lymphatic vessels analyzed. In secondary lymphedema collecting vessels, the wall thickening was due to either SMC hyperplasia (contraction type) or to collagen deposition (sclerosis type), whereas most of the primary lymphedema lymphatic collecting vessels were sclerotic. Vessel patency resulted significantly decreased in primary compared with secondary lymphedema. Analysis of the endothelial marker podoplanin revealed that its expression was variable and unrelated with the vessel type or the stage of lymphedema.
Materials and Methods
Patients
We collected lymphatic vessel samples from 17 patients affected by primary lymphedema (13 female, 4 male). Lymphedema onset was at birth in 2 cases (1 male and 1 female), between 10 and 35 years in 10 cases (3 males and 7 females), and after 35 years in 5 cases (5 females) (Table 1). Genetic tests were not available for any of our patients, but the two patients in which lymphedema was present at birth had a brother or a sister affected.
Patients' Background
LVA, lymphaticovenous anastomoses.
We also obtained samples from 29 patients affected by secondary lymphedema (26 female, 3 male). Most of these patients developed secondary lymphedema of the upper limb after oncologic surgery for breast cancer. Lower limb samples were from patients who had developed lymphedema after surgical treatment of endometrial cancer (8 patients), melanoma (2 patients), and Merkel cell carcinoma (1 patient) (Table 1).
Patients currently undergoing radiotherapy and/or chemotherapy were excluded. All the patients were white individuals coming from Italy who received LVA surgery in the local hospital (AOUS Scotte, Siena, Italy). Lymphangiography revealed lymphatic dysfunction in all patients.
The clinical severity of lymphedema was graded according to the International Society of Lymphology (ISL) staging. 10 Briefly, stage 0 corresponds to a latent or subclinical condition with normal appearance; in stage I, lymphedema subsides with limb elevation and pitting may occur; and in stage II, limb elevation alone rarely reduces tissue swelling and pitting is manifest. Late in stage II, pitting may or may not occur as tissue fibrosis develops and limb elevation never reduces swelling; in stage III, lymphostatic elephantiasis occurs, pitting is absent, and there are trophic skin changes, including acanthosis, fat deposits, and warty overgrowth.
Ethics committee approval (Comitato Etico Regionale per la Sperimentazione Clinica della Regione Toscana, Approval number 11048) and written informed consent were obtained for all patients. This study complies with the ethical standards laid down in the 1975 Declaration of Helsinki. The study has been registered at clinical trial.gov (identifier: NCT03465930; unique protocol ID: LVA 2017; title: Histologic Analysis of the Lymphatic Collecting Vessels Used for Minimally Invasive Supermicrosurgical Lymphatico-venous Anastomoses in the Treatment of Lymphedema).
Before the minimally invasive LVA surgery, each patient underwent lymphatic vessel mapping using indocyanine green lymphangiography to identify lymphatic vessels and to determine the site of skin incision. 11 Veins were identified with AccuVein. During surgery, a sample of the collecting vessels to be anastomosed with an adjacent vein was removed and used for morphological and immunohistochemical studies.
Histopathological investigations
Lymphatic collecting vessel segments were fixed in 10% formalin, embedded in paraffin, and cut into 8-μm-thin serial sections. To distinguish collagen fibers from SMCs in the wall of collecting vessels, Masson's trichrome staining was used (Abcam, Cambridge, United Kingdom) following the manufacturer's instructions. With this method, collagen fibers are stained blue by aniline blue and SMCs red by Biebrich scarlet-acid fuchsin. Elastic fibers were stained on different sections with Weigert (Merck KGaA, Darmstadt, Germany) according to the manufacturer's instructions.
For immunohistochemical studies, the following primary antibodies were used: monoclonal mouse anti-podoplanin clone D2–40 (DakoCytomation, Agilent Santa Clara, CA), monoclonal mouse anti-smooth muscle α-actin (α-SMA) clone 1A4 (Sigma-Aldrich, St Louis, MO), and polyclonal rabbit anti-smooth muscle myosin heavy chain 11 (MyH11; Sigma-Aldrich). The immunohistochemical labeling was performed with the avidin/biotin HRP complex technique (IHC select detection system from Millipore, Burlington, MA). The reaction was revealed with the 3,3′-Diaminobenzidine Substrate Kit for peroxidase (Vector Laboratories, Burlingame, CA). On each slide, the first section was used as a negative control omitting the primary antibody, and counterstaining was performed with Mayer's hematoxylin. Sections were mounted using Immuno-Histomount (Sigma-Aldrich) and viewed under a Nikon Eclipse E600 light microscope equipped with a digital camera. The morphometric software Nis element v3AR (Nikon Instruments, NY) was used to measure areas of the lumen and of the entire vessel tracing the inner and the outer profile of the vessel on Masson's trichrome-stained sections.
Results are reported as mean ± SEM. Statistical significance was assessed by ANOVA and Bonferroni post-test, Student t test with Welch's correction, or one-sample t test, as appropriate (GraphPad Prism version 6.0; GraphPad Software, Inc., San Diego, CA). In all comparisons, values of p < 0.05 were considered significant.
Results
Histological findings
The wall of all lymphatic collecting vessels, similarly to that of blood vessel, is composed of three layers. The internal layer consists of endothelial cells; the media contain extracellular matrix with varying proportions of SMCs arranged in interweaving bundles orientated in many different directions; and finally, a circular layer of SMCs is present at the border with the adventitia. 12
Histological evaluation of collecting lymphatic vessels was performed on specimens derived from primary and secondary lymphedema patients. Using Masson's trichrome, we evaluated the morphology and composition of the vessel wall (Fig. 1) and observed the same vessel types as previously described 5 : (1) thin-walled vessels with a wide lumen (i.e., normal type); (2) dilated vessels with a very thin wall (i.e., ectasis type); (3) stenotic vessels with a thickened wall due to SMC hyperplasia (contraction type); or (4) stenotic or occluded vessels with a thickened wall due to collagen fiber deposition (sclerotic vessels). In secondary lymphedema, stenotic vessels were either of the contraction or the sclerosis type, whereas in primary lymphedema, we failed to detect any contraction-type vessels; all the stenotic vessels were of the sclerosis type (Fig. 1).
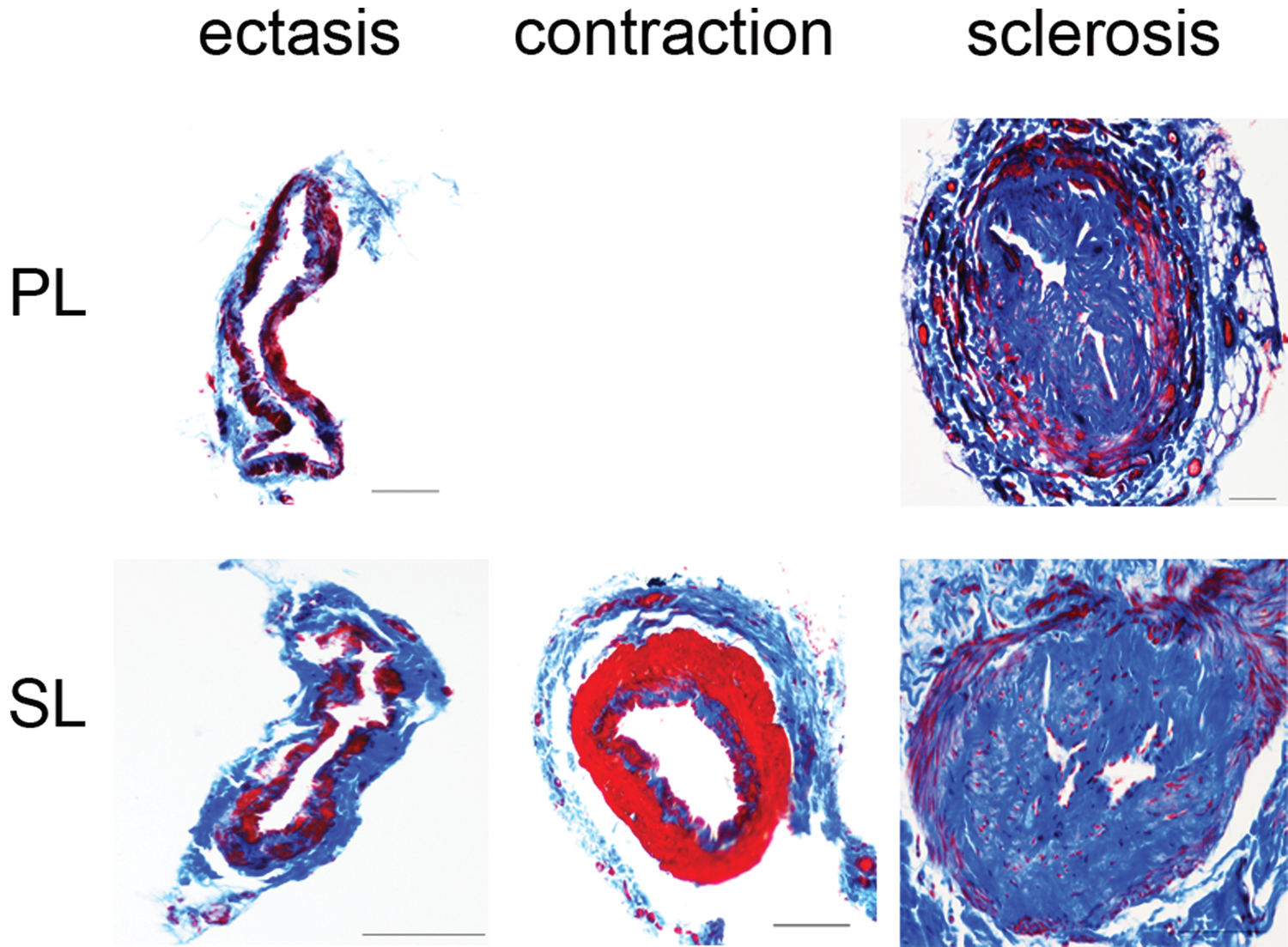
Masson trichrome staining of lymphatic collecting vessels. SL collecting vessels are of three types: ectasis, contraction, and sclerosis, PL is either of the ectasis or of the sclerosis type. Scale bar = 100 μm. PL, primary lymphedema; SL, secondary lymphedema. Color images are available online.
In secondary lymphedema samples, we found normal, ectasis, contraction, and sclerosis vessel types. Surprisingly, out of 17 primary lymphedema samples analyzed, we found that the majority of vessels were of the sclerosis type, and the contraction type was missing (Fig. 2).

Proportions of the different vessel types found in PL and in SL.
To evaluate the degree of luminal narrowing, which has a direct effect on lymph transport, we therefore measured the proportion of the empty lumen area with respect to the entire vessel area, calculated as the ratio between the lumen and the entire vessel cross-sectional areas (referred to as patency). In primary lymphedema, neither the patency nor the vessel type correlated with the clinical stage (Fig. 3A), probably due to the small number of patients at clinical stages II and III. In secondary lymphedema, patency significantly decreased in relation to the stage of disease (Fig. 3B); the majority of vessels with a wide lumen were from patients at clinical stage I, whereas the majority of vessels with a narrow lumen were from patients at stage II and III. Overall (Fig. 3C) patency was significantly greater in secondary than in primary lymphedema.

Morphometric analysis of the lymphatic collecting vessels in PL and SL. Relationship between lymphedema stage (X axis) and vessel patency (Y axis) in PL
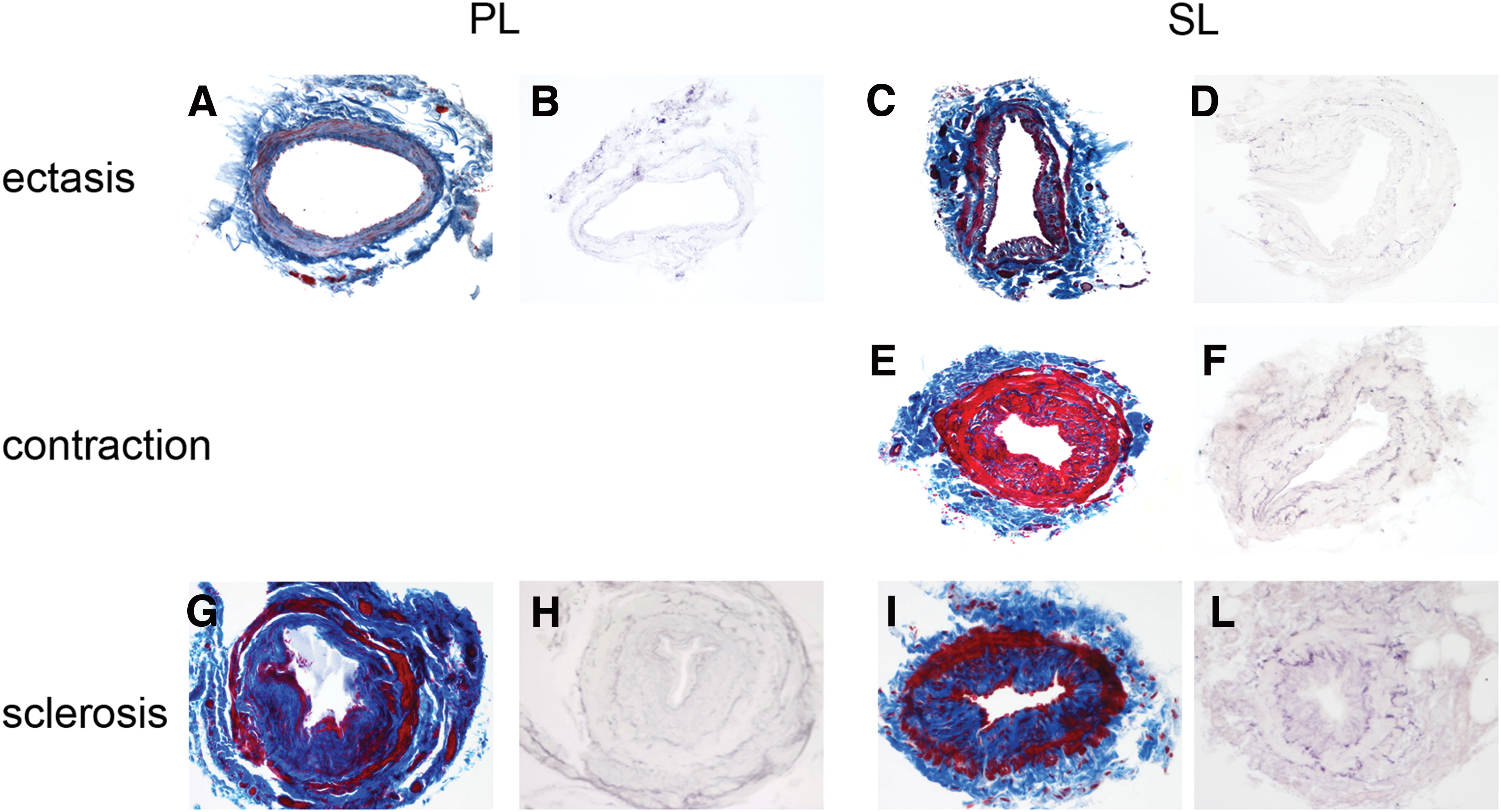
To better analyze the cells stained in red by Masson's trichrome, we performed an immunohistochemical analysis with antibodies to α-SMA (also known as ACTA2) and smooth muscle myosin heavy chain (MyH11). In ectasis (Fig. 4A) and contraction (Fig. 4B) vessel types, we found that all cells stained red by Masson's trichrome staining expressed α-SMA and MyH11. In the sclerosis type, the external circular layer of SMCs, stained red by Masson trichrome, was consistently positive for α-SMA and MyH11 (Fig. 4C, D). Interestingly, most of media cells also expressed α-SMA. In some collecting vessels, all α-SMA-positive cells also expressed MyH11 (Fig. 4D), whereas in others there were α-SMA-positive cells that did not express MyH11 (Fig. 4C).

Immunohistochemical analysis of α-SMA and MyH11 in PL and SL. Masson trichrome staining and immunohistochemical staining with antibodies to α-SMA and MyH11 of normal
Weigert staining evidenced that elastic fibers were present but scarce in the wall of collecting vessels, with no striking differences between the wall of collecting vessels from secondary and primary lymphedema. Sometimes these fibers appeared condensed in an inner and an outer layer (Fig. 5).
Elastic fiber detection in collecting vessels. Weigert staining evidenced few elastic fibers in the wall of collecting vessels from PL and SL.
Immunohistochemical analysis of podoplanin expression
To examine the endothelial layer, we analyzed the expression of the lymphatic endothelial marker podoplanin. At variance with Mihara et al. 5 who reported that the endothelium of the collecting lymphatic vessels progressively loses podoplanin expression in relation to vessel-type progression from ectasia to contraction and eventually sclerosis types, we found that in some collecting vessels, podoplanin was uniformly and intensely present, in others, its expression was markedly reduced regardless of any clinical correlate (ISL stage, duration of disease, morphologic type of vessel) and of patency of the lumen.
In those cases in which two lymphatic collecting vessels ran side by side, we sometimes found that one of them was intensely positive and the other negative. Unexpectedly, we also found vessels with a sclerosis morphology and a podoplanin-positive endothelium (Fig. 6). We failed to detect any difference between primary and secondary lymphedema samples.
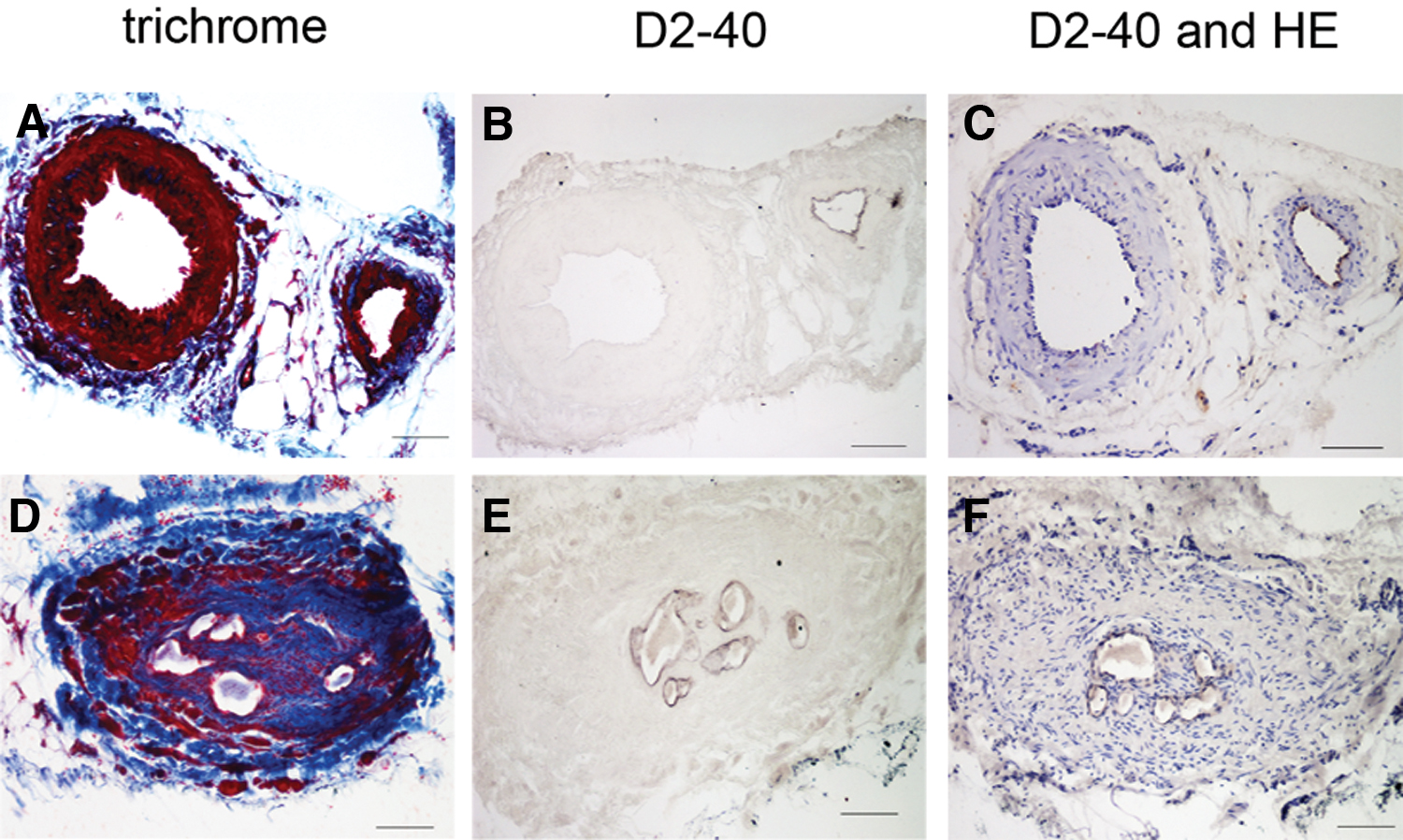
Immunohistochemical analysis of podoplanin expression. Masson trichrome
Discussion and Conclusions
Secondary lymphedema in industrialized countries is mainly due to lymphatic injury and lymph flow interruption following oncologic surgery and radiotherapy. This leads to stagnation of lymphatic fluid and extravasation of proteins that exert osmotic pressure in the interstitial spaces causing a high-protein edema that favors inflammation, which in turn stimulates fibrosis. 13
The surgical treatment of LVA has proven to be effective in ameliorating the conditions of the affected limb.13–15 During this mini-invasive surgery, it is easy to obtain a short segment of the lymphatic vessel chosen for the anastomosis with no extra discomfort or complication for the patient. The obtained samples may provide useful information on the extent of lymphatic alterations, thus helping to determine selection criteria of patients, and, based on the expected progression speed, to predict chances of reversibility or improvement of lymphedema.
Previous work on secondary lymphedema of the lower limb 5 classified the collecting lymphatic vessels into four types: normal, ectasis, contraction, and sclerosis, based on histological changes of the lymphatic collecting vessel. In particular, the vessel lumen was dilated in the ectasis type, while an increase in SMCs and collagen fibers was reported to be the cause of wall thickening of the contraction and sclerosis types, respectively. The four types of collecting lymphatic vessels were associated with different clinical stages of lymphedema, with a prevalence of normal and ectasis types at early stages, while the contraction and sclerosis types gradually increased in number with the progression of the disease, suggesting that collecting lymphatic vessels gradually transformed from one type into the next.
Our data on secondary lymphedema of the upper and lower limb confirmed that disease progression inversely correlates with lumen patency, as already reported, 5 for lower limbs. Interestingly, we found that vessels with muscular hyperplasia, corresponding to the contraction type, may have both intermediate and reduced patency, just as vessels with a prevalence of collagen, corresponding to the sclerosis type. We also found contraction and sclerosis vessel types with an almost completely occluded lumen, suggesting that both types may hamper lymph flow and thus account for lymphedema worsening. Most of the vessels found in primary lymphedema samples had instead a very narrow lumen and were of the sclerosis type, regardless of the clinical stage.
A possible explanation for this difference between primary and secondary lymphedema may be differences in age of onset and duration of disease before LVA: on average, 14.8 years in primary and 6.9 years in secondary lymphedema patients. Furthermore, patients with prolonged disease and early onset might establish compensatory physiological mechanisms and keep swelling under control through manual lymph drainage and compression garments. These methods, avoiding progression of the disease, might also explain why the majority of primary lymphedema patients in this study were at clinical stage I and II (13 out of 17).
Our data on the absence of contraction-type vessels in primary lymphedema are at variance with those of Asano et al. who, using hematoxylin/eosin and α-SMA immunostaining, reported their presence not only in secondary but also in primary lymphedema. 16
We found that most of the α-SMA-positive cells of the media layer were not stained red by Masson's trichrome and were MyH11 negative, suggesting that they were not typical SMCs. Moreover, different durations of disease between lymphedema onset and LVA may also account for this discrepancy. On average, in our casuistry, duration of disease in primary lymphedema was 14.8 years. Asano's patients underwent LVA much earlier, on average 7 years after disease onset, a time in which the contraction type might still be present. This discrepancy, if confirmed, may therefore bring further support to the hypothesis of transformation of contraction- to sclerosis-type vessels with time.
We also performed an immunohistochemical characterization of the lymphatic collecting vessel wall, evaluating podoplanin expression in the endothelium. In agreement with previous reports, 5 we observed that some lymphatic collecting vessels were positive for podoplanin and others negative, but, at variance with them, we failed to find any correlation between podoplanin expression and vessel morphology, clinical stage of disease, or time elapsed from lymphedema onset.
We found podoplanin-positive lymphatic collecting vessels running side by side with negative ones. This heterogeneity of expression might explain why literature on podoplanin expression in lymphatic collecting vessels is controversial. Some articles reported podoplanin-positive collecting lymphatic vessels,5,17–19 while others found that expression of podoplanin correlated with the caliber of lymphatic vessels: lymphatic capillaries were positive and larger lymphatic vessels negative.12,20
Literature is controversial also for other lymphatic markers, Prox-1 and VEGFR3. Some authors found Prox-1-expressing collecting vessels, 12 others reported that these markers are expressed at lower levels in collecting vessels. 4 The reason and functional implications of podoplanin variable expression in different collecting vessels even of the same patient and district are beyond the scope of this study.
From several studies on the role of SMC in vascular remodeling emerged the concept of SMC phenotypic switching, a model in which SMCs shift between a differentiated contractile phenotype and a dedifferentiated synthetic phenotype (i.e., myofibroblast) characterized by increased extracellular matrix synthesis and increased cell proliferation and migration. 21 Typically, myofibroblasts are identified by the expression of α-SMA; however, some myofibroblasts also express MyHC. 22
To characterize the cellular population of the media, we used antibodies to α-SMA and to MyH11. The former has been extensively used as an SMC marker, although it is known to be expressed in a wide variety of non-SMC types, including myofibroblasts. 23 Expression of smooth muscle myosin heavy chain (MyH11) has been reported to be more restricted to fully differentiated SMCs. 24
We found a diffuse staining for α-SMA in most cases. However, not all α-SMA+ cells also stained for MyH11: the outer circular SMC layer was consistently positive, whereas the α-SMA+ cells in the inner layers were sometimes positive and sometimes negative for MyH11. The α-SMA+-MHy11− cells might be interpreted as modulated SMCs whose presence has been reported to be often associated with vascular disease development. 24 These cells might therefore be interpreted as a stage of differentiation of SMCs of the inner longitudinal layer into myofibroblasts.
This hypothesis is supported by the finding that in chronic lymphedema, α-SMA+-MHy11+ SMCs are present not only in the tunica media but also in the subendothelial region, that is, in the tunica intima. 6 However, it is worth to consider that these cells might also originate from endothelial cells via the endothelial/mesenchymal transition. 25 Their transformation into myofibroblasts might be triggered by inflammation. 26 Interestingly, Asano et al. 16 recently reported an increase in inflammatory cytokines, namely tumor necrosis factor-α and interleukin 1β, in the wall of collecting vessels of primary and secondary lymphedema.
Taken together, our results confirm that the wall thickening of lymphatic vessels is associated with disease progression not only in lower limbs, as previously reported, but also in upper limb secondary lymphedema and in primary lymphedema. With disease progression, the patency is reduced and the vessel wall becomes thick due to hyperplasia of SMCs or due to collagen deposition. Hyperplasia of SMCs may be a compensatory mechanism, often occurring in secondary lymphedema, aimed to force the interrupted routes of lymph, but, restricting the lumen, it may increase the resistance to lymph flow decompensating the system similarly to what happens in arterial hypertension. 27 SMC switch to the synthetic state may lead to increased collagen deposition contributing to restrict the vessel lumen and thus hampering lymph flow. Myofibroblasts may also account for collagen deposition.
Further studies are needed to unravel the factors involved in these changes.
Footnotes
Author Disclosure Statement
No competing financial interests.
Funding Information
This work was supported by PSR Piano di Sostegno alla Ricerca 2017–2018 to VB and EW from the University of Siena.