
Abstract
Background:
To examine the correlation between lymphedema severity on lymphoscintigraphy and indocyanine green (ICG) lymphography in patients with secondary lower extremity lymphedema.
Methods and Results:
The maximal circumference difference (MCD) between the two legs was recorded. Lymphoscintigraphy and ICG lymphography images were classified into type I to V according to dermal backflow (DB) stage and MD Anderson Cancer Center (MDACC) stage based on lymphatic flow preservation and how DB was extended. Correlation between the scales was analyzed. Forty-four patients attended our hospital for evaluation of secondary lower extremity lymphedema. The most common cause of lymphedema was a postoperative complication of a malignant tumor (32 patients; 72.5%). Correlation analysis showed that lymphoscintigraphy and ICG DB (anterior) stage (r = 0.92), lymphoscintigraphy and ICG DB (posterior) stage (r = 0.94), and lymphoscintigraphy and MDACC stage (r = 0.93) exhibited very strong positive correlations. Intrarater agreement between lymphoscintigraphy and ICG DB (posterior) stage was substantial (κ = 0.65), and moderate between lymphoscintigraphy and ICG DB (anterior) stage (κ = 0.59) and lymphoscintigraphy and MDACC stage (κ = 0.52). Lymphedema severity stages and MCDs exhibited moderate positive correlations.
Conclusion:
Lymphoscintigraphy and ICG lymphography stage were strongly and positively correlated. These studies can work synergistically as complementary studies of lymphedema severity.
Introduction
There are several causes of secondary lymphedema of the lower legs, which is caused by impeded lymphatic vessel blood flow, and these include treatment of malignant tumors, bacterial infections, and chronic venous insufficiency. 1 Lymphoscintigraphy and indocyanine green (ICG) lymphography are the main diagnostic methods for lymphedema,2,3 and these tests are useful for evaluating the severity of lymphedema and determining the most appropriate treatment.4,5 Recently, the International Society of Lymphology emphasized the importance of early diagnosis and severity assessment through lymphoscintigraphy and ICG lymphography when functional lymph vessels are preserved.5,6 The microsurgical approach is used worldwide for the treatment of lymphedema for which conservative treatment is not effective. 7 Both tests commonly diagnose lymphedema and assess severity by looking at the presence of lymph nodes, symmetry of lymphatic pathways, and presence and extension of dermal backflow (DB).7–10 Both tests have specific advantages, so they are not used interchangeably, and neither is considered the gold standard. Therefore, although both tests are performed simultaneously in many cases, there have been no studies conducted to confirm the correlation between the two modalities for the evaluation of lymphedema in the lower extremities.
In this study, we analyzed the correlation between the results of the two tests after confirming the relationship between clinical severity and creating a grading system for lymphoscintigraphy results in patients with lower extremity lymphedema. We also aimed to determine whether it is possible to create a synergistically comprehensive diagnostic test using the two tests.
Materials and Methods
Patients
In this study, 44 patients who underwent lymphoscintigraphy and ICG lymphography between January 2018 and February 2020 were enrolled to evaluate lower extremity lymphedema. This study was approved by our institutional review board, and the requirement for written consent was waived (IRB No. D-1803-012-065). Exclusion criteria were patients who had previous primary lymphedema, history of trauma, metastasis, or infection of both arms, and patients in whom staging was impossible due to poor image quality or atypical findings.
Indocyanine green lymphography
A total of 0.2 mL of ICG (Diagnogreen Inj., Daiichi Pharmaceutical, Tokyo, Japan) (2.5 mg/mL) was injected subcutaneously into the first web space of both feet and the lateral border of the Achilles tendon. To minimize the pain, lidocaine hydrogen chloride 2% with epinephrine 1:100,000 was injected before dye injection. After injection, circumferential images of lymphatic drainage channels were obtained using an infrared camera (Moment K, Gils, Seoul, Korea) to detect 760 nm light-emitting diode and a filter cutting light below 820 nm. Images were taken every hour after injection until the ICG dye spread to the whole leg and sufficient ICG lymphography staging was possible. The images were classified into type I to V according to ICG DB stage 11 and MD Anderson Cancer Center (MDACC) stage 12 (Fig. 1). ICG DB staging was scored using the anterior posterior aspect separately.
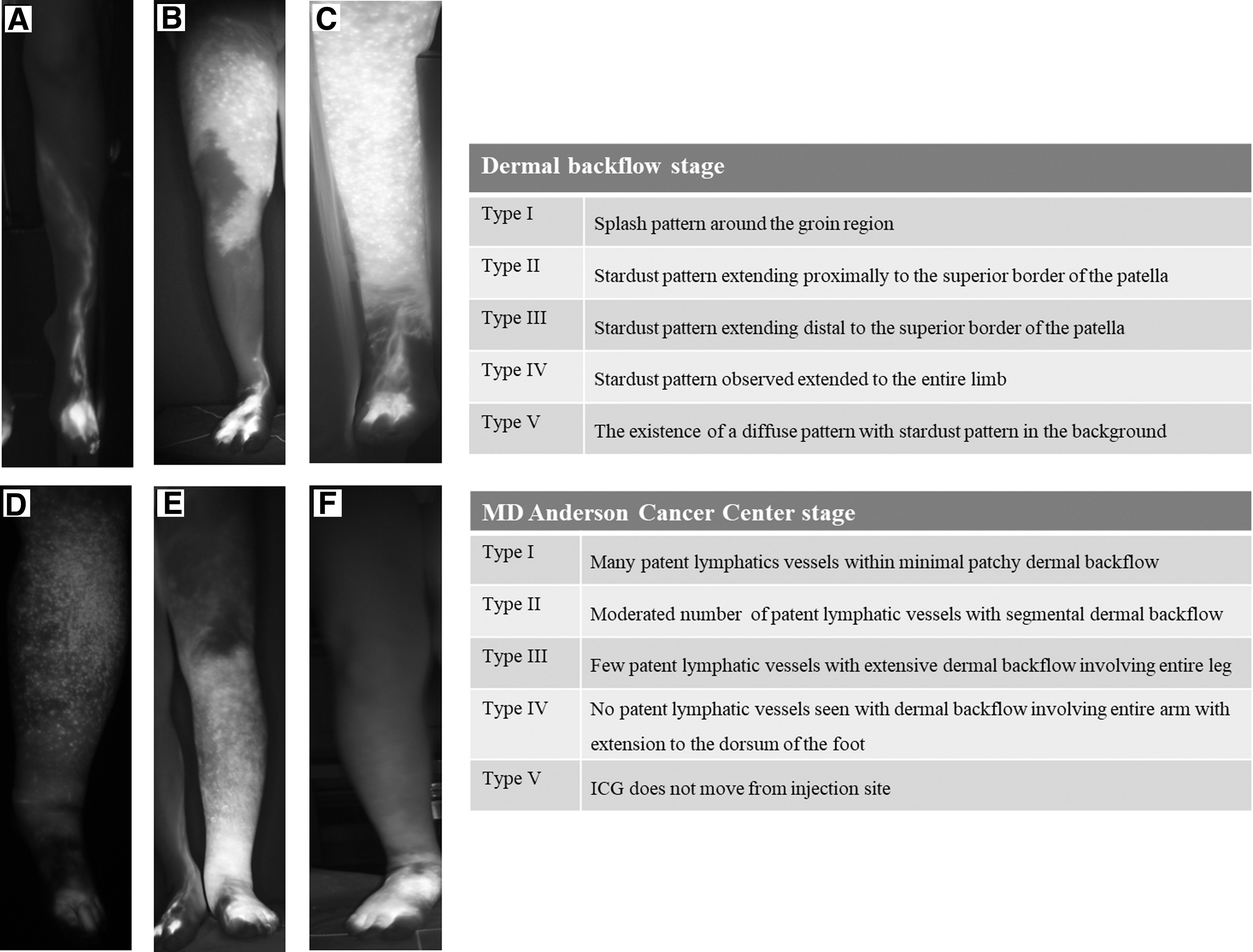
ICG lymphography images of cases of ICG DB stage and MDACC stage type I to V.
Lymphoscintigraphy
Phytate containing a 37-MBq (1-mCi) dose of Tc-99m in a 0.2-mL syringe was injected subcutaneously into the first or second interdigital dorsum web spaces of both feet. All images were obtained as planar images using a dual-head gamma camera (Infinia; GE Medical Systems, Milwaukee, WI, USA) at a rate of 300 sec/frame, with a matrix size of 256 pixels × 256 pixels and a zoom factor of 1.0. The energy discriminator was centered on the 140-keV photopeak of Tc-99m using a symmetric 20% window. Early lymphatic flow images were obtained in both lower extremities at 5 and 15 minutes to avoid missing the 10 minute flow record, as previously recommended. 13 Delayed images were acquired at 30 minutes and 1 hour postinjection, and images were classified into type I to V based on how lymphatic flow was preserved and how the DB was extended (Fig. 2). 5

Lymphoscintigraphy images of cases of type I to V.
Circumference differences in the lower extremities
The circumference of the affected and unaffected legs at four sites, including the ankle, 10 cm below knee, and 10 and 25 cm above knee, was measured using flexible tape. The maximal circumference differences (MCDs) between both legs at each site were recorded. 2
Statistical analysis
The data were presented as mean and standard deviation. Spearman correlation was applied for the analysis of the degree of association between the variables. A Kappa analysis was calculated between scales. p values of <0.05 were considered statistically significant. All data were analyzed with the use of R 3.6.0. IRR package (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 44 patients were recruited for this study. Two patients were excluded from the analysis due to poor imaging quality or atypical findings. The mean age of the patients was 52.92 ± 15.13 years, with 30 women and 14 men. The most common cause of lymphedema was a complication of malignant tumor treatment (32 patients; 72.5%). In the other three patients, two cases of lymphedema occurred after tumor removal in the inguinal area and one case occurred as a result of intestinal tuberculosis (Table 1). The mean and median maximal circumference lymphoscintigraphy severity stage, ICG DB stage, and MDACC stage are shown in Table 2. In the correlation analysis, lymphoscintigraphy and ICG DB (anterior) stage (r = 0.92), lymphoscintigraphy and ICG DB (posterior) stage (r = 0.94), and lymphoscintigraphy and MDACC stage (r = 0.93) exhibited very strong positive correlations (Table 3 and Fig. 3). Intrarater agreement between lymphoscintigraphy and ICG DB (posterior) stage was substantial (κ = 0.65), and it was moderate between lymphoscintigraphy and ICG DB (anterior) stage (κ = 0.59) and lymphoscintigraphy and MDACC stage (κ = 0.52). The lymphedema severity stages and MCDs exhibited a moderate positive correlation (Table 4).
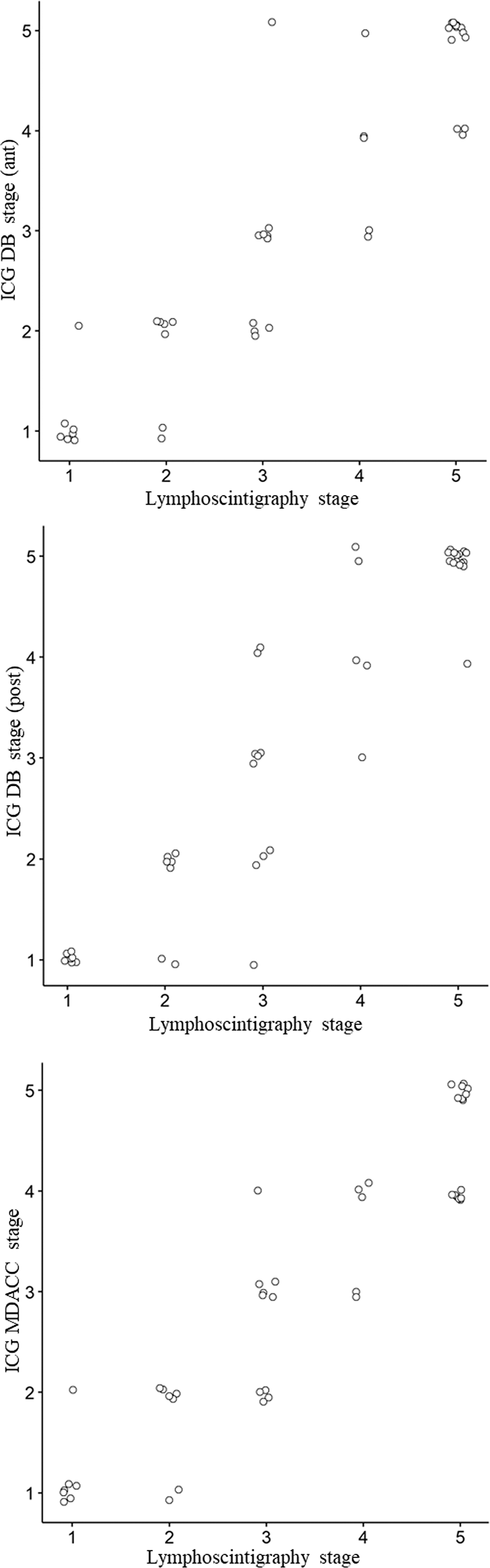
Scattered plot according to correlation coefficient between lymphoscintigraphy and ICG stage.
Primary Disease Causing Lymphedema
Clinical and Image-Based Lymphedema Severity Degree of the Patients
DB, dermal backflow; ICG, indocyanine green; MCD, maximal circumference difference; MDACC, MD Anderson Cancer Center; SD, standard deviation.
Correlation Analysis Between Lymphedema Severity Stages
A: Lymphoscintigraphy stage versus ICG DB stage (anterior).
B: Lymphoscintigraphy stage versus ICG DB stage (posterior).
C: Lymphoscintigraphy stage versus ICG MDACC stage.
Significant difference (p < 0.05).
CI, confidence interval.
Correlation Analysis Between Lymphedema Severity Stages and Circumferential Measurements
Significant difference (p < 0.05).
Discussion
In this study, because lymphedema severity stage showed a significant positive correlation with MCD—a clinical indicator of lymphedema—the severity stages of the two tests are appropriate to assess the severity of lower extremity lymphedema. All three stages performed in both tests showed very strong positive correlations and moderate to substantial agreement.
Lymphedema is a chronic, progressive pathologic condition that results from impaired lymphatic transportation as a result of injury, infection, or congenital or unknown abnormality of the lymphatic system. 14 Because of the recent advances in microscopic surgical procedures for lymphedema, clinico-imaging staging based on functional lymphatic vessels has become an important factor in evaluating surgical indications and postoperative prognosis as an alternative to conventional clinical staging. 15 Over the last decade, lymphoscintigraphy and ICG lymphography have been widely considered as primary investigations to confirm the diagnosis and visualize functional lymphatic vessels. Significant correlations between the two tests and clinical findings in lymphedema have been demonstrated in previous studies,14,16 and the association between the clinical findings has offered the possibility of identifying patients who may benefit from a microsurgical approach.
In cases of secondary lymphedema, it is not difficult to diagnose lymphedema through medical history and clinical findings. Therefore, the main purpose of conducting an imaging study is to establish a treatment plan by evaluating severity rather than to diagnose. Lymphoscintigraphy and ICG lymphography have their advantages. In particular, ICG lymphography, which can be used for sensitive assessment of whether shallow lymphatic vessels are preserved, has been reported to improve surgical results because anastomosis is performed by visual confirmation of the preserved functional lymphatic vessels rather than by random incision. 12 However, because deep lymphatics cannot be identified, when combined with lymphoscintigraphy, more information can be obtained to predict treatment plan outcomes and response to treatment. Cutoff points for surgical treatment of ICG lymphography stage II 17 and lymphoscintigraphy stage II 5 have been reported in previous studies, but to judge the direction and prognosis of the treatment by combining the results of the two tests, correlation between the results of the two tests is needed. In this study, although the degree of agreement was relatively low because the criteria for dividing the type by extension of DB were somewhat different between the two tests, the correlation between lymphoscintigraphy and ICG DB stages was high. DB flow is the phenomenon of lymph backflow from the collecting lymph duct to the dermis. 18 Therefore, since DB is located in a shallow region, there is no significant difference in the confirmation of DB between ICG lymphography, which mainly detects superficial lymphatics, and lymphoscintigraphy, which mainly detects deep lymphatics. There may be limitations in both tests for discriminating the part of the lymphatic vessel that is partially preserved and covered under the DB.
In the two tests, the severity was evaluated by five grading systems based on the presence of functional lymph vessels and lymph nodes and the extent of DB involvement. 5 For ICG lymphography, one of two different grading systems can be used depending on whether the focus is on the pattern and range of DB (ICG DB stage) or on visible lymphatic vessels (MDACC stage).12,18 Both staging systems of ICG showed a similarly high correlation with lymphoscintigraphy staging. In addition, because ICG lymphography has the advantage of being able to identify superficial lymphatics in various ways, the separate analysis was performed by randomly dividing ICG DB stage into anterior and posterior aspects in this study. In ICG lymphography, the interpretation of the test was based on the identification of the vessel passing through medial aspects of the foot dorsum, anterior tibia, and thigh for the anterior part and the lymphatic trunks running with small saphenous veins for the posterior part. 19 These lymphatic vessels may not be identified as identical on lymphoscintigraphy, but when the type is divided based on the DB extension, where the functional lymphatic vessels are not visible at the dermis level, both stages of anterior and posterior aspects showed very high correlation with lymphoscintigraphy grading. This shows that these image-based stages of lymphatic function could be interpreted comprehensively and used to evaluate severity of lymphedema.
In terms of concordance, ICG DB stage showed a somewhat higher kappa value than ICG MDACC stage. This may be because the lymphoscintigraphy stage and the ICG DB stage coincide with the disease progression generally occurring in the proximal to distal direction in secondary lower extremity lymphedema and the grading in terms of resulting extension of the DB. However, in MDACC, types are divided according to preserved lymphatic vessels, which can be easier to use as a prognostic tool through lymphatic mapping during microsurgery. In the case of ADB stages III to V, which are divided based on stardust and diffuse DB patterns, it is easy to determine postoperative improvement. However, it is excluded from the criteria determining possibility of lymphaticovenous anastomosis, because precise evaluation is easier with the MDACC stage. In the interpretation of the two test results, the former showed a higher degree of agreement, but neither could be judged as the superior grading system.
The limitation of this study was that both stages used in this study could have some limitation of inter-rater and intrarater unreliability and possibility of unclassifiable cases, which are excluded in our study. Recently, there are several reports of modified ICG lymphography stages that allow better clear-cut classification.20–23 Especially, lymphatic duct mapping is also an important part in surgical planning, and ICG lymphography is often able to identify finer lymphatic ducts. Thus, if more specified lymphoscintigraphy stages appear at a later period, an additional correlation analysis could be possible. Second, it was not possible to conduct quantitative analysis of both tests. Recent studies have reported a significant association between quantitative analysis of lymphoscintigraphy and clinical severity, 15 and the importance of precise evaluation through quantitative analysis has been emphasized in the case of ICG lymphography. Therefore, further research on the correlation between the quantitative evaluation values of the two tests will be meaningful. In addition, the number of patients in this study was relatively small with diverse causative diseases; however, this study was the first to analyze the correlation between the two most frequently used tests for evaluation of patients with secondary lower extremity lymphedema. Because we excluded patients whose primary lymphedema or regional traumatic lymphatic injuries may differ in terms of the anatomy of the lymphatic vessels—which may cause confusion in dividing types—this does not limit the interpretation and the clinical meaningfulness of our findings.
Conclusions
In conclusion, lymphoscintigraphy severity stage and ICG lymphography stage showed a very strong positive correlation with moderate to substantial agreement. Both studies can work synergistically and may be used as complementary studies of lymphedema severity evaluation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (Nos. 2019M3A9E8068533 and NRF-2016M3A9E8942061).