
Abstract
Background:
Overweight and obesity are strongly implicated in breast cancer (BC) development and are also a risk factor for BC-related lymphedema (BCRL).
Methods and Results:
An online cross-sectional survey was conducted between November 2017 and January 2018. Analyses were restricted to women with localized BC, who provided information about BCRL (n = 238). Most women were not experiencing BCRL (55.46%). Mean self-reported weight at diagnosis was 68.55 kg for women without BCRL and 74.43 kg for women with BCRL (p = 0.0021). In this study, 50.9% with BCRL were overweight/obese at diagnosis (body mass index [BMI] ≥25) compared with 36.4% of women without BCRL (p = 0.003). For women without BCRL, 12.12% were classified as obese (BMI ≥30) versus 20.75% with BCRL. Women with BCRL were more likely to have gained >5% of body weight (p = 0.03), be currently overweight or obese (p = 0.004), and less active (48.11%) than they were at diagnosis than women without BCRL (33.33%) (p = 0.042). Having a structured exercise program, following a prescribed diet, and being accountable to someone else were identified as the main facilitators to successful weight loss and weight maintenance.
Conclusions:
Clinicians should consider obesity when personalizing axillary treatment and encourage lifestyle interventions and lymphedema screening after BC treatment.
Introduction
With the increase in survivors of breast cancer (BC) due to improved treatments, there has been a corresponding increase in the number of women with BC who are living with long-term side-effects, such as fatigue and cognitive problems, and sexual dysfunction has increased as there are more survivors from better treatments. 1 Another side-effect feared by patients is lymphedema.2,3 The mean interval from BC treatment to the development of arm lymphedema is 8 months. Rates of BC-related lymphedema (BCRL) range from 5% with a sentinel node biopsy to 20%–50% with axillary node dissection and regional node irradiation.4–6
Obesity is considered a risk factor for lymphedema. 7 In one study, patients with a body mass index (BMI) greater than 30 had a twofold risk of developing BCRL related to the increased tissue either acting as a reservoir for lymph, or simply requiring more surgery destructive to the lymphatics. 8 Thus, it is important to explore the association of weight and obesity before and after a diagnosis of BC with or without BCRL.
The prevalence of weight gain after BC has not been adequately quantified for patients with or without BCRL. It is unclear whether weight gain, common after BC treatment, may exacerbate the incidence of lymphedema, or whether lymphedema is simply another factor on a long list of factors exacerbating reduced activity leading to more weight gain.
The aim of this study was to describe the prevalence and potentially complex relationship between self-reported overweight/obesity before and after BC to alert clinicians and their patients about potentially avoiding a catch-22 situation where weight gain is associated with BCRL and BCRL is associated with more weight gain.
Materials and Methods
Study design and inclusion criteria
A cross-sectional survey was conducted in Australia as detailed elsewhere. 9 The sample included members of the Breast Cancer Network Australia (BCNA) Survey and Review Group (n = 1857) who agreed to receive e-mails about research studies. Of the 309 respondents, 273 (95.8%) completed the survey. There were 232 patients with localized early-stage BC (defined in the survey as “where your breast cancer is contained within your breast and/or lymph nodes”) who contributed data on weight at diagnosis or at the time of the survey. Patients with metastatic disease or with only ductal carcinoma in situ (DCIS) were excluded.
Weight
Women were asked to self-report their weight (kg) at diagnosis, current weight and height, and BMI as weight/(height) 2 . This was categorized as underweight (<20), normal weight (≥20 and <25), overweight (≥25 and <30), or obese (≥30) and further dichotomized into overweight/obese and normal weight/underweight. 10 Percentage weight gain was classified as weight loss, 0%–5% weight gain, 5%–10% weight gain, and >10% weight gain. We further dichotomized this into weight maintenance (<5% weight gain) or weight gain (≥5% weight gain). The pattern of weight gain was self-reported as “gained weight overall,” “lost weight overall,” “weight stable,” or “weight has fluctuated a great deal,” and concern about weight was determined by an 11-point Likert scale from 0 (not at all concerned) to 10 (very concerned).
Physical activity
Current physical activity (PA) levels were calculated according to the number of 20-minute sessions of less vigorous exercise or more vigorous exercise a week, given a weighting and described in terms of MET (metabolic cost) minutes,9,11 where MET minutes less than 80 were coded as “no physical activity,” 80 to 400 as “low,” 400 to 560 as “moderate,” and more than 560 as “high.” A value of 4 METs was given to moderate PA and 7.5 to vigorous PA. PA was further dichotomized into “none or low levels of physical activity” and “moderate to high levels of physical activity.” Women were asked to self-report any change in PA since diagnosis (more active than before, less active than before, about the same). Perceived barriers and facilitators to successful weight loss and weight maintenance were also explored. A list of potential barriers (e.g., lack of time to exercise, financial barriers, fatigue, lack of willpower/motivation) and facilitators (accountability, informal/formal social support) was presented to women to select, with an option to enter free-text answers.
Lymphedema after diagnosis
Self-reported arm lymphedema severity was defined as “no problem (no noticeable swelling),” “mild (soft swelling i.e, not obvious to others and comes and goes),” “moderate (swelling with occasional hardness in some areas i.e., obvious to others and is always present),” or “severe (profuse swelling with thickened skin, constant hardness, and a very large, heavy arm i.e, extremely obvious to others and is always present).” 2 Presence of lymphedema was classified as “none/no problem” or “mild/moderate/severe.”
Statistical analysis
To explore the relationship between BMI and weight at diagnosis, weight gain, current BMI, and weight and BCRL, we used simple logistic regression and one-way ANOVA for weight, weight gain, and BMI as a continuous outcome, and Pearson's chi-square and odds ratios (ORs) for BMI classification and weight gain (gained >5% of weight or did not gain >5% of weight) as a categorical outcome as previously described. 9 We examined for an association between self-reported change in PA or current levels of PA and development of BCRL using Pearson's chi-square. Pairwise deletion was used to account for missing data.
We specifically explored the following research questions:
Is higher BMI or weight at diagnosis a predictor of lymphedema? Do women with lymphedema gain more weight than women without lymphedema?
Results
Sample characteristics
Selected demographic characteristics are described in Table 1. The majority of women were Caucasian (91.63) with a mean age of 57.40 years. More detailed demographic analysis has been reported elsewhere. 9 Most women were not experiencing current lymphedema (55.46%), 33.61% were experiencing mild BCRL, 8.82% moderate, and 2.10% severe BCRL.
Demographic and Treatment Characteristics
ALND, axillary dissection; BCRL, breast cancer-related lymphedema; N, number; RT, radiotherapy; SNB, sentinel node biopsy.
Clinical characteristics
All respondents indicated they were diagnosed with localized BC (n = 238).
Clinical diagnostic and treatment details are also shown in Table 1. The mean time since diagnosis was 8.24 years and the mean age at diagnosis was 50.2 years. Patients who had BCRL were more likely to have had an axillary dissection, with or without radiation (46.64%), than patients without BCRL (p < 0.0001).
Weight at diagnosis
Table 2 describes weight change for the two groups. Mean self-reported weight at diagnosis was 68.55 kg for women without BCRL and 74.43 kg for women with BCRL (p = 0.0021). Higher BMI and weight at diagnosis were associated with subsequent BCRL (p < 0.001). For each 1 kg increase in weight at diagnosis, there was a 3.2% increase in likelihood of developing subsequent BCRL (OR 1.03, p = 0.004, 95% confidence interval [CI] 1.01–1.05). In this study, 50.9% with BCRL were overweight/obese at diagnosis (BMI ≥25) versus 36.4% of women without BCRL (p = 0.003). When we analyzed according to BCRL categories of severity, women who subsequently developed moderate BCRL were the heaviest at diagnosis with a mean weight of 76.75 kg, standard deviation [SD] 11.80 (p = 0.0186), and this was consistent with the finding that women who were overweight or obese at diagnosis were more likely to develop moderate BCRL [χ 2 (3, n = 218) = 9.5044, p = 0.023]. For women without BCRL, 12.12% were classified as obese (BMI ≥30) versus 20.75% with BCRL (p = 0.07). For mild, moderate, or severe BCRL, the incidence of obesity was 20.0%, 23.81%, and 20%, respectively. For each 1 unit (kg/m2) increase in BMI, the risk of developing BCRL increased by 7.6% (OR 1.08, p = 0.005, 95% CI 1.02–1.14).
Weight and Weight Management Details
Underweight (BMI <20); normal weight (BMI ≥20 and <25); overweight (BMI ≥25 and <30); obese (BMI ≥30).
MET (metabolic cost) minutes.
BMI, body mass index; PA, physical activity; SD, standard deviation.
Current weight
Women with BCRL were 2.39 times more likely to be currently overweight/obese (BMI ≥25) compared with women without BCRL (p = 0.004). For women with BCRL, 72.6% were overweight/obese when surveyed versus 57.6% of women without BCRL [χ 2 (1, n = 227) = 8.60, p = 0.003]. Women who had moderate BCRL were more likely to be currently overweight/obese than women in other BCRL severity categories [χ 2 (3, n = 227) = 11.34, p = 0.01].
Weight gain
Of women with BCRL, 62.26% had gained more than 5% weight compared with 53.03% women without BCRL (p = 0.03) [χ 2 (1, n = 222) = 4.72, p = 0.03] (Table 2). This correlated with the finding that women with BCRL were 1.79 times more likely to have gained weight since diagnosis, compared with women without BCRL (p = 0.042).
Women with BCRL gained an average of 6.00 kg, while women without BCRL gained an average of 4.31 kg (p = 0.17). There was no difference in absolute weight gain according to BCRL severity (p = 0.50) (Table 2).
Physical activity
A significantly greater proportion of women with BCRL (48.11%) reported that they were less active than at diagnosis compared with women without BCRL (33.33%) [χ 2 (2, n = 233) = 6.83, p = 0.03]. However, there was no difference in self-reported change in PA across different severities of BCRL [χ 2 (6, n = 233) = 10.73, p = 0.10] (Table 2).
There was no difference in current levels of moderate-high PA between women with BCRL (55.8%) and women without BCRL (60.77%) (p = 0.45) [χ 2 (1, n = 232) = 0.56, p = 0.45], including no difference when the analysis was expanded to categories of BCRL severity [χ 2 (3, n = 232) = 3.61, p = 0.31] and different levels of PA (none, low, moderate, high) [χ 2 (9, n = 232) = 13.63, p = 0.14].
Barriers and facilitators of weight loss
Figures 1 and 2 describe the perceived barriers and facilitators to weight loss for women with or without BCRL. There was no statistically significant difference between the proportion of women with or without BCRL who named structured exercise as a facilitator (p = 0.102).
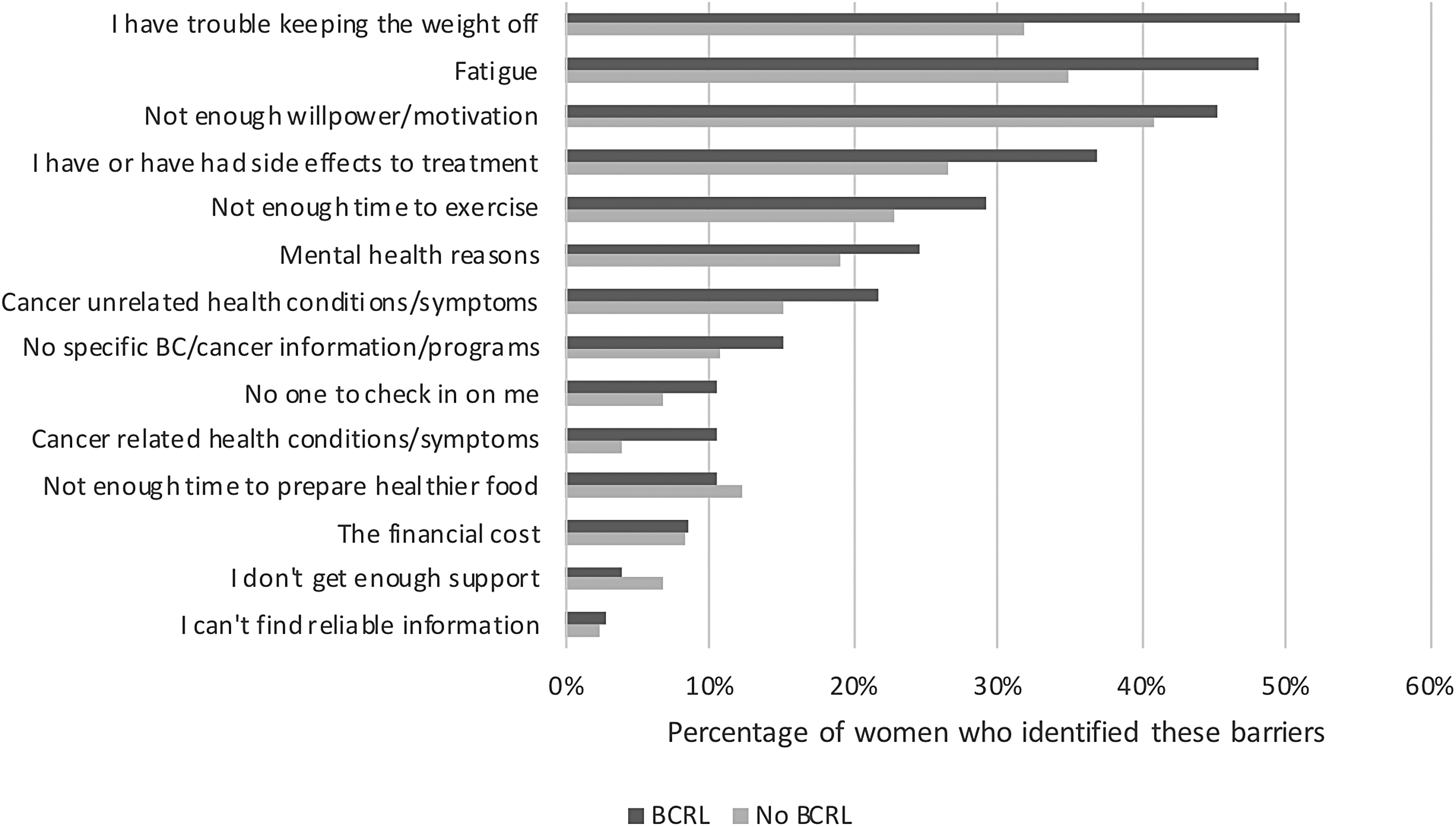
Barriers to weight management/weight loss. BCRL, breast cancer-related lymphedema.

Facilitators of weight management/weight loss.
Discussion
Women who were obese or overweight at diagnosis were not only more likely to develop BCRL but also more likely to gain weight after treatment. Patients and their clinicians need to be aware of this catch-22 situation when planning treatments to the axilla and to develop follow-up strategies.
Women with BCRL were 2.22 times more likely to be overweight or obese at time of diagnosis (50.9%) compared with women without BCRL (36.4%) (p = 0.024). Furthermore, a greater proportion of women with BCRL reported that they were less active (48.11%) than they were at the time of their diagnosis compared with women without BCRL (33.3%) (p = 0.042). As a result, women with BCRL were twice as likely to currently be obese compared with women without BCRL (p = 0.04), and 1.85 times more likely to have gained >5% of their body weight since diagnosis (p = 0.03).
One of the first reports linking obesity to a higher incidence of BCRL studied patients, largely treated by mastectomy and axillary dissection, found that although patients who were overweight at diagnosis had an increased risk of developing lymphedema, weight gain post-treatment was a stronger predictor. Twenty-year results found that women who gained more than 10 pounds (4.54 kg) had a 60% incidence of BCRL compared with 40% for those patients who gained less weight (p = 0.02). 12 High BMI (≥25 or 30) as a risk factor for BCRL was also found by other investigators.13–15 In our study, 12.12% of patients without BCRL were classified as obese (BMI ≥30) versus 20.75% without BCRL, confirming our hypothesis that obesity at diagnosis is associated with a higher risk of subsequent BCRL. Potential physical, vascular, metabolic, and hormonal explanations of this link between overweight and obesity to an increased incidence of lymphedema have been reviewed elsewhere. 16
An important question whether treatment to axilla in obese women could be de-escalated given the increased risk of BCRL. The AMAROS randomized trial compared axillary and supraclavicular fossa radiation after a positive sentinel node to an axillary dissection and found no difference in outcome except for less arm edema (11% vs. 23%; p < 0.0001) in the RT group at a median follow-up of 6.1 years. This approach would avoid an axillary dissection for selected patients with limited isolated tumor cells or micrometastases. 17
An unresolved issue is whether strategies to reduce weight improve BCRL once it develops. A randomized clinical trial of 351 obese patients with BCRL found that a 12-month home-based exercise or weight loss intervention, alone or in combination, had no effect on the percentage of interlimb difference. 18 These findings contradict a previous small observational study suggesting that lymphedema symptoms may improve with weight loss.19,20 Weight loss has been shown to reduce levels of leptin with favorable modulation of inflammatory cytokines known to be increased for patients with BCRL.21–23
Our second research question was whether patients with established BCRL gain more weight perhaps due to less activity brought on by physical limitations of an enlarged arm or self-esteem or comfort issues. It is difficult to answer this question particularly as weight gain is not uncommon after treatment for many reasons. In our study, a greater proportion of women with BCRL reported that they were less active and 62.26% gained more than 5% of their body weight compared with 53.03% for patients without BCRL (p = 0.03). However, there was no difference in current PA levels between women with or without BCRL, suggesting that factors other than PA such as diet or metabolic factors may be contributing.
The implications of this study are that patients who are overweight or obese face a catch-22 situation. These patients have more BCRL and people with BCRL may reduce PA and gain more weight. This situation could be addressed by health interventions that can improve both weight and lymphedema although both are difficult to manage and treat and BCRL can be hard to detect particularly in overweight patients. In related research, we found almost 80% of patients gained weight in the first 18 months after treatment. 9 Similarly, although BCRL can occur at any time, most patients present within the first 12–24 months. 24 Therefore, there is a critical window for potential “survivorship” intervention within the first 18 months after treatment where lifestyle changes lymphedema screening with bioimpedance spectroscopy (BIS), associated with less long-term problems as reported elsewhere. 25 In that study, patients who were screened with BIS had a lower rate of detection of subclinical BCRL than those screened by tape-measure (TM) (15.8% vs. 28.5%, p < 0.001). All patients who triggered had an intervention with a compression sleeve and gauntlet for 4 weeks and were then reassessed. Twelve triggering patients progressed to complex decongestive physiotherapy (10 in the TM group [14.7%] and two in the BIS group [4.9%]), representing a 67% relative reduction and a 9.8% absolute reduction (p = 0.130). These interim results demonstrated that post-treatment surveillance with BIS may be a more sensitive screening measure particularly for obese or overweight patients where measurement error with TM is likely to be increased.
The strengths of this study include the high response rate from the BCNA survey as reported elsewhere and that we achieved a broadly nationally representative sample according to location. This study has some limitations. We were not able to fully understand the BC stage for our patients except that the disease was localized to the breast ± axilla. This could have included some patients with stage 3 disease, but we excluded patients with stage 4 disease or with only DCIS. Similarly, we did not have information on specific chemotherapy drugs such as taxanes known to increase the risk of BCRL. Although using self-reported weight and height is a simple way to obtain data, studies suggest that people tend to underestimate their weight and overestimate their height. 26 This may be, in part, due to social desirability and response bias. Recall bias may also lead to inaccuracies in self-reported weight. Change in PA was also self-reported and may be influenced by response bias. Furthermore, our sample was limited mostly to members of the Review and Survey Group from BCNA, and although the response rate was 50% higher than what is typically expected from this group, the generalizability of our findings may be limited. Another potential weakness is the lack of ethnic and cultural diversity in our sample, and future research should seek to understand the impact of ethnic and cultural origin on weight and lifestyle habits in an Australian setting. 27 Larger studies would also be required to further analyze our research questions by the extent of BCRL as the numbers of women with severe BCRL were small. Finally, the measurement of lymphedema was self-reported and was higher than in a general BC population. 2
Conclusions
Most women with BC gain weight after treatment. Women with lymphedema have a higher BMI before treatment, are less active, and gain more weight after treatment. This catch-22 must be addressed by ensuring treating clinicians are mindful of this problem and recommend post-treatment exercise and attention to healthy nutrition, as well as to advise screening to detect BCRL before it becomes clinically apparent.
Acknowledgments
We thank the consumer representatives from Breast Cancer Network Australia who provided feedback on the survey instrument used in this study; Natalie Zakhary who assisted with formatting the online survey; Kellie Stalgis-Bilinski who provided early feedback on the survey; and Karen Monaghan who assisted with data cleaning.
Footnotes
Authors' Contributions
C.C.L.E. conceived the study and led the data collection. J.B. conceived the lymphedema substudy. C.C.L.E. and J.B. contributed to the design of the study. A.E.C., C.C.L.E., and D.N. contributed to data analysis. All authors contributed to the interpretation of the findings. C.C.L.E. and J.B. cowrote the article's full draft. All authors reviewed the article and approved it for publication.
Author Disclosure Statement
J.B. is a stockholder in ImpediMed Limited. The remaining authors have no financial interests to disclose.
Ethical Statement
The procedures followed were in accordance with the Ethical Standards of the Responsible Committee on Human Experimentation (Institutional and National) and with the Helsinki Declaration of 1975, as revised in 2008. Ethics approval for this study was provided by the Human Research Ethics Committee, Western Sydney University (H12444, Oct 2017). Catch-22: The American Heritage Dictionary defines Catch-22 as a situation in which a desired outcome or solution is impossible to attain because of a set of inherently illogical rules or conditions (![]() ).
).
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. As a medical research institute, the NICM Health Research Institute receives research grants and donations from foundations, universities, government agencies, individuals, and industry. Sponsors and donors also provide untied funding for work to advance the vision and mission of the institute.