
Abstract
Background:
The lymphedema-affected limbs are predisposed to acute and, subsequently, chronic dermato-lymphangio-adenitis (DLA) episodes in around 40%–50% of cases, irrespective of what the primary etiological factor is for the development of this condition. DLA is of bacterial etiology, and it needs antibiotic control and prevention of recurrence. Our aim was to follow the effects of years-long continuous no-break administration of benzathine penicillin on the recurrence of acute DLA episodes.
Methods and Results:
Two hundred thirty-one patients were affected with lymphedema of lower and upper limbs. The mean duration of lymphedema was 10.2 ± 7.3 (range 2–30) years, and the number of DLA attacks/patient was 3.3 ± 3.2 (range 1–10). The total number of DLA episodes was 805. Benzathine penicillin injections 1,200,000 units were given i.m. at 14–21 days intervals (mean 18 ± 9 days) with short accidental breaks only. The period of therapy was 39.2 ± 38.7 (median 32) months. Recurrence occurred in 23 out of 231 (10%) (p < 0.01). There were 42 DLA incidents compared with 805 before introduction of therapy (5.2%) patients (hazard ratio 0.05, 95% confidence interval 0.034–0.079) (p < 0.01). Among patients with recurrence, there was a decrease of DLA episodes from 6.2% ± 3.6% to 1.7% ± 1.0%/patient. There were no differences in effectiveness of penicillin prophylaxis between etiological groups, depending on stages of lymphedema.
Conclusions:
Long-term years-long benzathine penicillin prophylaxis is extremely effective in prevention of DLA recurrence. It can be applied for years with no breaks, without clinical side-effects, and raising resistance to antibiotics. Microbial colonization and evoked inflammatory reaction of hosts should be controlled from the first symptoms of lymph stasis, irrespective of the etiology of lymphedema.
Introduction
Obstruction of the lymphatic pathways in limbs causes formation of edema in the tissue interstitial space. Flow away of proteins, cellular debris, metabolic products, and recirculating cells to the regional lymph nodes, cysterna chyli, and thoracic duct to the blood circulation is compromised. Bacteria and viruses penetrating foot and hand skin are usually flown away with the lymph stream to the lymph nodes. In case of obstruction they are retained in the interstitial space, proliferate, and evoke the inflammatory response. Once they colonize tissues, they remain there as “persisters.”1,2 To compromise their local activity, intensive antibiotic therapy is needed, followed by long-lasting prophylaxis against recurrence of the inflammatory episodes. This inflammatory complication of lymphedema is generally called “cellulitis,” “lymphangitis,” or “erysipelas.” 3 We proposed to use the term “dermato-lymphangio-adenitis” (DLA). 4
There is a general misunderstanding of the differences between the three listed conditions pondering on the type of applied therapy. Cellulitis is a common type of skin and soft tissue infection. It is also a cosmetic term describing accumulation of painful adipose tissue in the thigh and calf. Lymphangitis is a primary local nonsystemic, nonspreading change in the skin and subcutaneous tissue caused by own skin flora, with a mild clinical course. Erysipelas is a primary acute local spreading condition in the skin with a systemic reaction. It is caused by beta-hemolytic group A Streptococcus bacteria. It may be contagious. It either develops in the lymphedematous tissues or it is the primary factor for its development.5,6 All this only partly corresponds to what we observe in the lymphedematous limbs. This is why we proposed for lymphedema inflammatory episodes to use the term “dermato-lymphangio-adenitis,” reflecting the pathophysiological inflammatory events, appearing first in the skin (Fig. 1), then in the subcutis, and, subsequently, in the lymphatics and lymph nodes. 7 This sequence of events can be easily observed on the isotope or ICG lymphograms (Fig. 2).
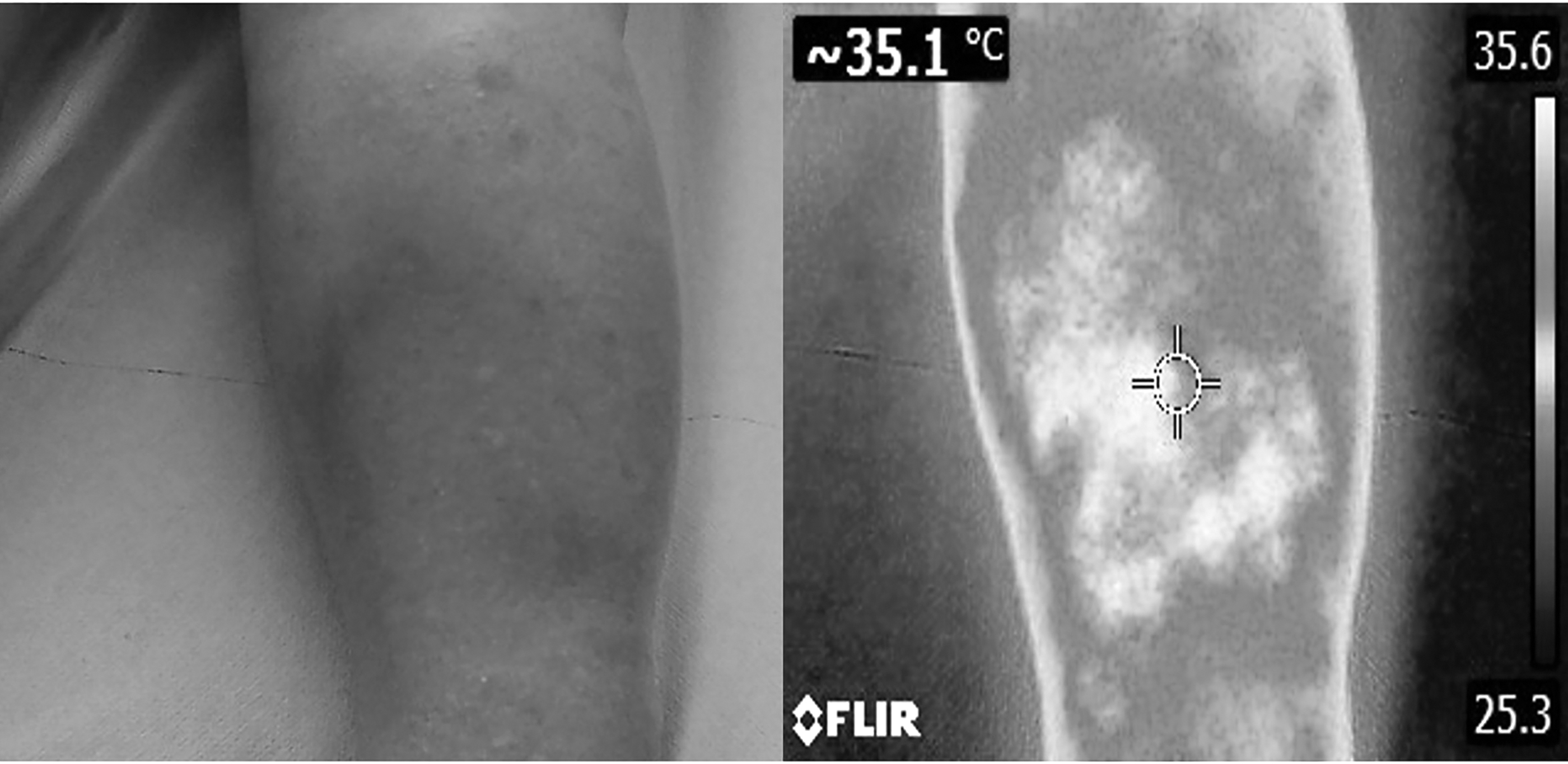
Clinical picture of the lower limb affected by DLA in course of obstructive lymphedema. The erythema is spread in skin of the whole limb. In comparison with circumscribed acute dermatitis, the increased skin temperature is observed on the whole surface. The normal skin surface temperature monitored at stable ambient temperature oscillates around 31°C; whereas in the DLA cases it reaches 35°C. DLA, dermato-lymphangio-adenitis.

Lymphoscintigrams of the three most common types of obstructive lymphedema affected by recurrent attacks of DLA. These are the postmastectomy and posthysterectomy with local lymphadenectomy because of cancer and postdermatitis lymphedema. Sites with most accumulation of the tracer are the reservoirs of the not-transported away scores of Staphylococci responsible for the chronic and acute DLA (arrows).
About 40%–50% of patients with lymphedema, regardless of etiology, develop acute and subsequently chronic DLA. In the lower limbs, patients with secondary lymphedema stage II have around 38% and in stage III 61.7% incidents of acute DLA incidents.8–11 In the upper extremities, after mastectomy and local irradiation, infection of the swollen limb, expressed as acute and later as chronic inflammation, ranges between 20% and 40%.12,13 As the literature review 14 in patients with acute episodes of DLA, the bacteremia is found in a high percentage (21% acute and 26% subacute cases). The mean frequency remains at around 10% 15
The DLA is of bacterial etiology and has, as previously mentioned, a tendency for recurrence. Short-term wide-spectrum antibiotic treatment of DLA episodes does not prevent the recurrence. The prevention should be based on long-term, and in some cases permanent administration of antibiotic in a low dose. This type of therapy requires intramuscular injections of benzathine penicillin 1.2–2.4 million units every 2–3 weeks.16,17
The aim of the current study was to follow the effects of the years-long-benzathine penicillin continuous no-break administration on recurrence of acute DLA episodes. The study began in 1990. Patients with diagnosed postmastectomy, posthysterectomy, and postdermatitis limb lymphedema, experiencing in the past at least 1 episode of DLA, were receiving 1,200,000 units of benzathine penicillin injection at 14 days intervals. All who actively complied with our prophylaxis protocol, and did not choose another medical institution for treatment, were systematically seen in our outpatient clinic in the period from 1990 and 2019, and reports on the lymphedematous limb inflammatory changes were collected.
Materials and Methods
Patients
Two hundred thirty-one patients with lymphedema of lower and upper limbs were included in the study (Fig. 3). They enrolled in an order of showing up in the outpatient department in the period 1990–2020. Three groups of patients, according to the etiology of lymphedema, were formed (Fig. 4 and details in Table 1). Group 1, postmastectomy lymphedema stage II–IV, contained 60 females, aged 35–75, after mastectomy with lymphadenectomy, radiotherapy, and chemotherapy. Group 2, posthysterectomy with lymphadenectomy and radiotherapy, lymphedema stage II–IV, contained 40 females, aged 43–68 years. Group 3, postdermatitis, after prior foot or calf skin inflammation (trauma, abrasion, unknown type of skin infection), lymphedema stage II–IV, contained 131 patients (82 females, 49 males), age 35–82 years.

The number of patients with limb lymphedema reporting acute DLA attacks and the total number of DLA attacks over the past 10 years. A mean of lymphedema duration, frequency of DLA per patient and duration of benzathine penicillin therapy (mean values ± SD). SD, standard deviation.
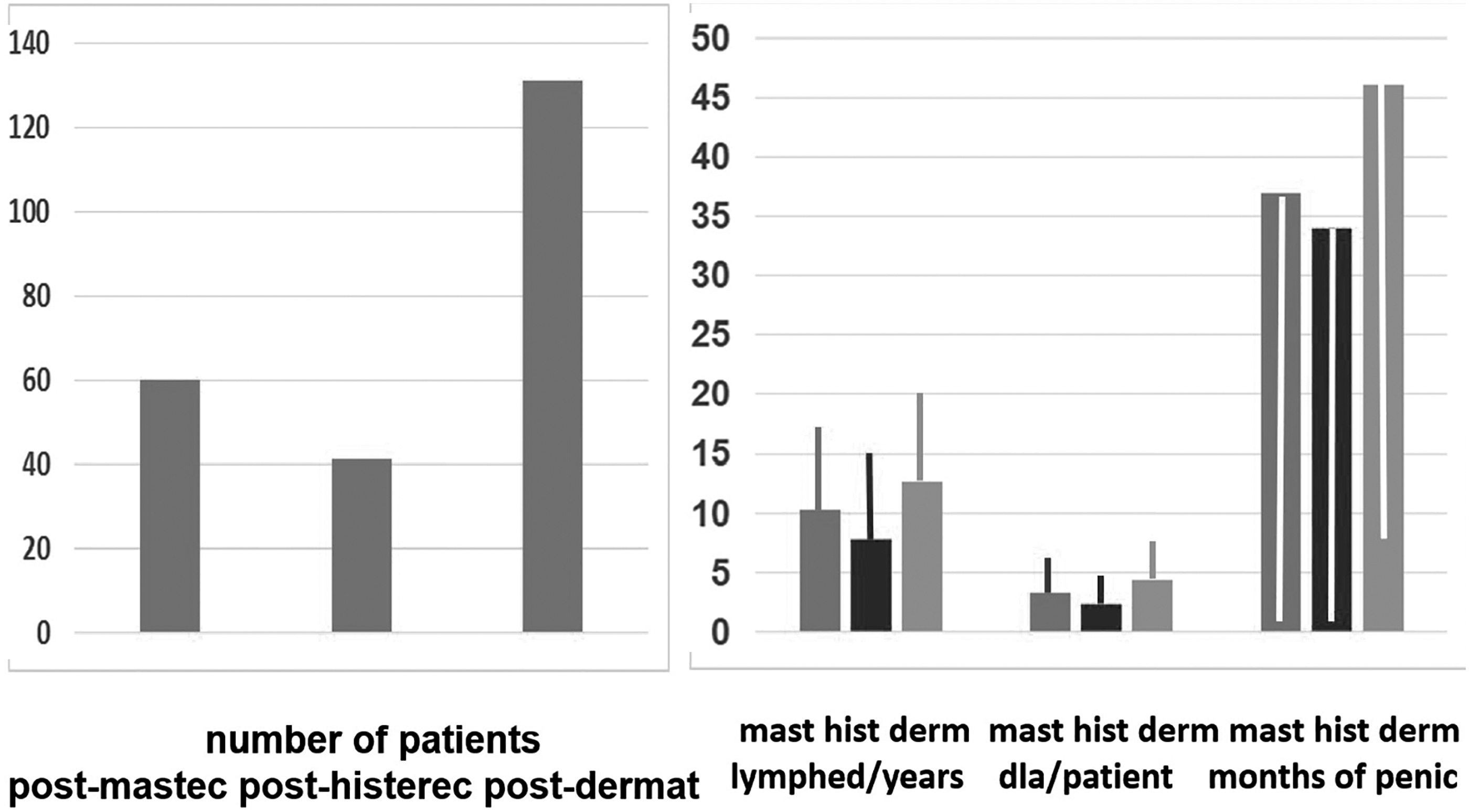
The number of patients with the postmastectomy, posthysterectomy, and postdermatitis DLA attacks. Mean time of lymphedema duration, number of DLA attacks per patient, and duration of benzathine penicillin therapy (mean values ± SD).
Duration of Lymphedema, Frequency of Dermato-Lymphangio-Adenitis Episodes, and Duration of Penicillin Administration (Mean, Standard Deviation, Range, Median)
DLA, dermato-lymphangio-adenitis.
DLA criteria
Acute DLA episodes were characterized by suddenly appearing fever, erythema streaks along the lymphedematous limb, sometimes erythema covering the whole limb surface, skin tenderness, and compromised limb movements. Most symptoms subsided after 3 days of oral antibiotic administration. However, local erythema and skin tension remained until the next episode of DLA. This study was approved by the bioethical committee of Warsaw Medical University. Approval number KB/159/2008.
Exclusion from the study
Patients with diabetes, obesity BMI (kg/m2) >30, heart failure, eczema/psoriasis, deep vein thrombosis, interdigital intertrigo, and venous insufficiency were excluded.
Clinical staging of lymphedema
Lower and upper limb
Staging (I, II, III, IV) was based on clinical evaluation described in our previous publications.2,18 Briefly, the advancement of lymphedema was determined according to the level of edema in the upper and lower limbs, and the presence of skin lesions such as hyperkeratosis and papillomatosis.
In stage IV, edema of upper limb swelling involves the hand, forearm, arm, and chest wall.
Lymphoscintigraphic staging
Lower and upper limb
The lymphoscintigraphic images were used to evaluate the lymphatic pathways, as previously described.2,19 Briefly, the severity of the edema (stage I, II, III, IV) was determined on the spreading of the tracer in the limb (foot or hand, foot and calf or hand and forearm, foot or hand and entire lower or upper limb), visualization of lymphatic vessels (interrupted, irregular, or absent), and lymph nodes.
In stage IV of upper limb, the tracer was spread on chest wall and shoulder.
Selection of a scheme for benzathine penicillin therapy for DLA
The protocol of penicillin injections frequency was based on our measurement of serum concentration on days 7, 21, and 28 after 1,200,00 units, i.m. injection. The Alpha Diagnostics Intl, Benzyl penicillin ELISA KIT Cat. #DE-100150 for Qualitative and Quantitative Determination of Benzylpenicillin (San Antonio, TX) was applied. In 50 investigated patients, the serum penicillin level measured 7 days after injection was 34.9 ± 8.7 ng/mL, at 21 days 41.2 ± 17.5 ng/mL (30% below 25 ng/mL), and after 28 days 21.0 ± 3.1 ng/mL. The minimum inhibitory concentration (MIC) of benzathine penicillin is, according to the literature, 60–100 ng/mL. 20 Since we planned to administer the benzathine penicillin for years and to avoid development of resistance, the MIC was set at a low level of 25 ng/mL on an injected dose of 1,200,000 units. This dosage did not create evident resistance to penicillin. 16 The intervals between injections were set at 2 weeks, according to our MIC estimates and literature recommendations.21,22 In our protocol, benzathine penicillin injections of 1,200,000 units were given i.m. at 14–21 days intervals (mean 18 ± 9 days) with short accidental breaks only. Around 5% of patients were receiving injections systematically over 30 years, with only short breaks ending with DLA recurrence.
Statistical evaluation
For evaluation of the effects of prophylaxis before and after administration of penicillin, hazard ratio (HR) was calculated and for the difference between etiological groups Student's t-test was used with <0.05 as statistically significant.
Results
The whole group
In the entire investigated group with benzathine penicillin administration for 39.2 ± 38.7 (median 32) months, 23 out of 231 (10%) patients revealed DLA recurrence. There were 42 DLA incidents compared with 805 before the initiation of therapy (5.2%) (HR 0.05, 95% confidence interval [CI] 0.034–0.079, p < 0.01) (Fig. 5). In these cases, 2 g of amoxicillin with clavulanic acid was administered orally for 3–5 days. It was followed by the administration of benzathine penicillin in a scheme, as described earlier.
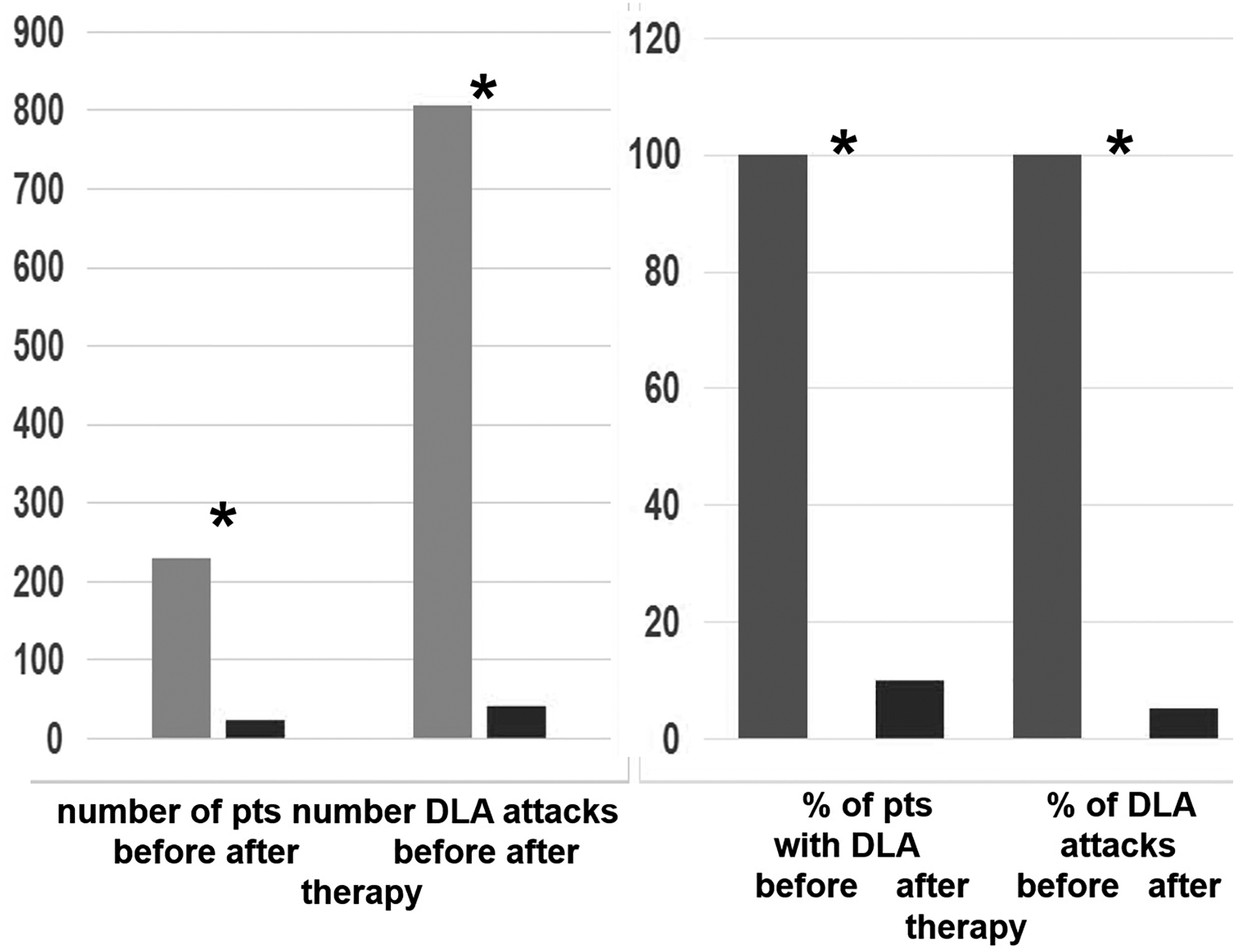
The effects of benzathine penicillin therapy in the whole group. The number of patients reporting the DLA attacks and the total number of DLA attacks significantly decreased (HR 0.05, 95% CI 0.034–0.079) *p < 0.01. CI, confidence interval; HR, hazard ratio.
The postmastectomy, posthysterectomy, and postdermatitis groups
Analysis of recurrence
There were 6 incidences of DLA out of 189 (4%) (p < 0.01) in the postmastectomy, 4 out of 102 (2%) (p < 0.01) in the posthysterectomy, and 32 out of 514 in the postinflammatory group (6%) (HR 0.031, 95% CI 0.01–0.089), (HR 0.039. 95% CI 0.013–0.122), and (HR 0.06, 95% CI 0.037–0.104), * all p < 0.01, respectively (Fig. 6). Interestingly, among the patients with recurrence there was a decrease in the individual DLA episodes from 6.2% ± 3.6% to 1.7% ± 1.0%/patient (Fig. 7). There were no statistically significant differences in the recurrence rates between groups and depending on the stage of lymphedema (no significant).
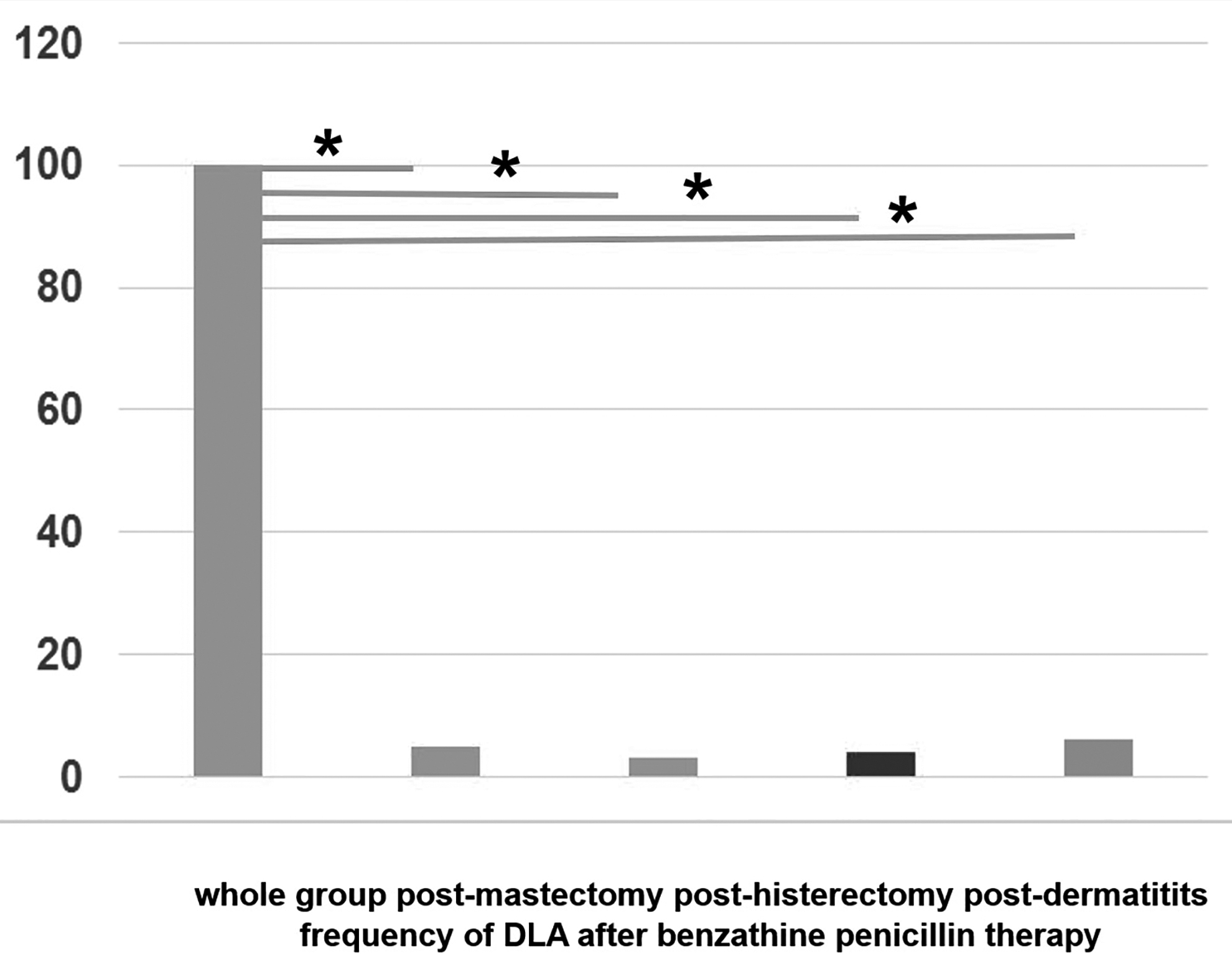
The percent of DLA attacks after benzathine penicillin therapy in the whole group, postmastectomy, posthysterectomy, and postdermatitis, (HR 0.031, 95% CI 0.01–0.089), (HR 0.039, 95% CI 0.013–0.122), and (HR 0.06, 95% CI 0.037–0.104), * all p < 0.01, respectively.

Frequency of recurrence during benzathine penicillin therapy. In the whole group, there were 23 (10%) of patients reporting 42 recurrence. The numbers of DLA attacks, % of DLA, and % DLA/patient in the postmastectomy, posthysterectomy, and postdermatitis groups are shown. The percent of DLA/patient with recurrence decreased compared with the pretherapy data.
Subjective reports of patients on additional effects of long-term benzathine penicillin prophylaxis
Patients report decreased susceptibility to common cold, influenza, sore throat, joint pains, and hemorrhoids.
Discussion
In the current article, we showed that in patients with lymphedema experiencing multiple DLA episodes, administration of benzathine penicillin in a long follow-up of a median 38 months (with time range 5–156 months) decreases the recurrence of attacks by 95%. This study confirms the result reported in the literature; however, our follow-up has been much longer, reaching in some cases a nonstop 30 year-long penicillin administration. Recurrence of DLA episodes in the whole group, irrespective of the etiology of lymphedema, was 5.2%. It was caused in most patients by interruption of treatment for 4–6 weeks, leg trauma, or long-distance running. Interestingly, among the patients experiencing recurrence, despite penicillin administration, there was a decrease in the frequency of DLA episodes from 6.2% ± 3.6% to 1.7% ± 1.0%/patient.
We treated patients with lymphedema of different etiology. In the postmastectomy and posthysterectomy group, obstruction of lymph flow was caused by scars at the site of lymphadenectomy; whereas in the postdermatitis group, damage to lymphatics and nodes was brought about by bacteria penetrating the foot skin. However, the common denominator remained, and it was stasis of the interstitial fluid and lymph. And this is where microbes penetrating skin are accumulating. Interestingly, there were no differences in the effectiveness of penicillin prophylaxis between the etiological groups, neither depending on the stages of lymphedema. This means that microbial colonization and evoked inflammatory reaction of the host should be controlled from the first symptoms of lymph stasis.
In the literature, ∼40%–50% of lymphedema patients, regardless of etiology, demonstrated infection of skin and subcutaneous tissue. There is prevalence of the incidents in the lower limbs in patients ranging between 12% and 80% compared with 10%–50% in upper limbs.8–13 The incidence rate of recurrent “cellulitis” in the prophylaxis period is decreasing from 0.73 episode/patient-year to significantly lower values than that of 1.25 episodes/patient-year in the nonprophylaxis period. 23
In patients with long-lasting lymphedema, relapses of acute DLA are much more frequent. Each incident of DLA is associated with limb enlargement. In the lower extremities, recurrent inflammation affects, as mentioned earlier, around 50% of patients, however, the statistical data vary depending on the demographic and environmental hygiene situations. In Tay et al.'s studies, 16% of patients developed at least one relapse of DLA. In a 3-year observation, the number of recurrences rate increased to 29% and 23%–47% of patients had to be hospitalized for treatment of a recurrence10,11
Relapses of DLA occur most frequently in patients with lower limb lymphedema and among them in postdermatitis type. Skin infections of various origins appear much more often in this area than in other parts of the body. It is caused by close contact of the lower limbs with environmental microbial flora, which is confirmed by bacterial strains isolated from the blood and tissues of lymphedema patients. Damage of the skin's immune barrier in lymphedema leads to the colonization of deep tissues and the spread of bacteria into the blood circulation. In some advanced cases, the course of acute DLA is very severe, requiring hospitalization and intensive antibiotic therapy. According to the literature, about 8%–10% of patients with acute DLA reveal bacteremia.6,14,24–26
Bacteria responsible for colonization of limb deep tissues and causing DLA are mainly those dwelling on our epidermis. Our previous bacteriological studies on lymphedematous legs lymph and nodes conducted on the European population demonstrated the presence of Cocci in 60% of samples and among them Staphylococcus epidermidis and occasionally Staphylococcus aureus.4,14 In the literature, Staphylococcus and Streptococcus are the dominant genera.
Interestingly, the study conducted by Cranendonk et al. on skin microbiota reveals great similarity between affected and unaffected limbs. Generally, the study did not show differences between microbiota composition from the skin of patients with cellulitis and controls. Traditional skin culture compared with skin microbiota analysis revealed no association in patients with cellulitis. No association was found between skin microbiota composition and diversity, and previous histories, clinical severity, and outcomes in patients with cellulitis.5,13,27
Antibiotics treatment kills most of bacterial cells. Still, some of them survive and undergo transformation into “persister” form or small colony variants. In this form, bacteria are nondividing cells, with minimum metabolism. They stay in our tissues for months and years and, under certain circumstances, return to normal function and begin to proliferate.1,2 An understanding of this phenomenon prompts us to search for methods preventing the re-activation of persisters by accidental signals as remote infection, trauma, viral invasion, and pharmacological immuno-suppression in transplantation and oncology.
One possible explanation of this distinct behavior of bacteria is “re-infection” hypothesis. According to this hypothesis, high relapsing risk is caused by tissue modification in the site of previous cellulitis episode. This consequently leads to repeated infections in the same area of the skin. Now, an explanation of recurring cellulitis is based on persistence of bacteria in affected tissues. Bacteria in “persiste” form (a latent infection) present in the tissue may, under certain circumstances, regrow and induce acute infection. It is well known that pathogens causing cellulitis (Streptococcus pyogenes [group A Streptococcus], S. aureus, Escherichia coli, Pseudomonas aeruginosa, Acinetobacter baumannii, etc.) may survive intracellular or in biofilm. This presence of bacteria in the tissue should be taken into account when planning effective antibiotic therapy to prevent recurrences of cellulitis. 28
How should we prevent reactivation of the dormant bacteria? According to our previous experience, it should be a long duration or even permanent antibiotic prophylaxis. Therefore, intramuscular administration of benzathine penicillin at a dose of 1.2–2.4 million units every 2–3 weeks with local anesthetic is the best solution and has proven efficacy greater than other oral protocols. In concert with the views on bacterial dormancy in limb tissues, we investigated the clinical course of lymphedema in terms of prevalence of DLA in patients receiving injections of long-acting penicillin for long periods. Already in 1996, we found that recurrent episodes of DLA in a 1 year penicillin-treated group decreased from 100% to 9% (p < 0.002).
Regarding the reaction of different bacterial strains during penicillin prophylaxis, we observed an increase in the presence of Cocci and gram-positive bacilli while reducing the presence of gram-negative bacilli grown from the food and calf skin surface. At the same time, among the bacteria isolated from lymph, and deep tissues of the lower limbs, a decreasing presence of gram-positive cocci and gram-negative bacilli was noted. No emergence of resistance to both penicillin and other tested antibiotics was observed. Interestingly, all bacteria isolated from the skin, deep tissues, lymph and lymph nodes, both lymphedema patients and healthy individuals, were susceptible to most antibiotics. Unexpectedly, the least susceptible was observed to penicillin, although this antibiotic was very effective in the treatment and prevention of DLA episodes. The high-level sensitivity of most strains suggests their environmental but not hospital origin. 29
Positive results of prophylactic effectiveness of benzathine penicillin on lymphedema DLA episodes are also accumulating from multiple sources. In the pertinent literature, the decrease in the DLA recurrence ranges between 46% and 100% when long-term penicillin is administered over 1 year.23,30–35 None of the studies reported severe adverse effects to antibiotics.16,36
There were some limitations of the study. Included into the evaluation were only patients who voluntarily complied with our protocol and were systematically seen in our outpatient clinic, whereas many patients went to other medical institutions. This being so, the evaluated group does not represent those who eventually had shortened prophylaxis or did not have improvement. The exact estimation of the frequency of DLA episodes per patient may be difficult, as some do not remember these occurring over years. Also, some episodes may have been lasting for 1 day and were neglected. There were major differences in the duration of lymphedema, frequency of DLA episodes per person, and duration of prophylaxis. This made the statistical evaluation limited, and data show a rather unidirectional trend.
In our study, we focused only on the effect of benzathine penicillin prophylactic administration. We did not analyze the influence of other factors such as proper compression. However, because the obstruction of lymphatic pathways brings about tissue fluid/lymph stasis, and subsequently, retention of microorganisms continuously penetrating sol and hand skin, daily evacuation of the accumulating tissue fluid using appropriate compression (intermittent pneumatic compression, bandaging, stockings, or sleeve) should be mandatory.
Taken together, long-term benzathine penicillin prophylaxis is extremely effective in prevention of DLA recurrence. It can be applied for years with no breaks without clinical side-effects and increasing resistance to antibiotics. It should be a means of choice in every case of recurrent DLA, irrespective of the etiology of lymphedema. Slowing down of the progression of morphological changes in lymphedema tissues is expected as hyperkeratosis and fibrosis. This needs further studies. Interestingly, long-term administration of benzathine penicillin decreases, according to the investigated patients, the occurrence of common cold, nose-throat complaints, joint pains, and hemorrhoids.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.