
Abstract
Background:
Lymphedema (LE) is a chronic condition of swelling due to lymphatic impairment and is characterized by edema and fibro-adipose tissue deposition. LE may be caused by an anomalous development of the lymphatic system, known as primary LE, or may develop secondary to traumatic, infectious, or other external events. Knowledge is increasing about the plural and bidirectional relationship between LE and obesity. The rate of obesity is increasing worldwide, and bariatric surgery offers the most effective and durable treatment, as this surgery exhibits positive effects on many obesity-related diseases. We explored whether bariatric surgery could improve leg volumes in morbidly obese LE patients.
Methods and Results:
Between 2013 and 2019, 829 patients were hospitalized in our Center of Expertise for Lymphovascular Medicine for intensive treatment of their LE. Nine patients with end-stage primary, secondary, or obesity-induced LE underwent a bariatric procedure related to their morbid obesity. Data concerning age, gender, medical diagnosis, LE stage, type of bariatric treatment, body weight, body mass index (BMI), and limb volumes were retrospectively collected from the patient files. At the individual patient level, body weight, BMI, leg volumes, and their percent reduction between presurgery and postsurgery were calculated. At the group level, paired sample t-tests were conducted to compare the mean body weight, BMI, and volumes of both legs between postsurgery and presurgery. The data demonstrate a significant decrease in body weight, BMI, and leg volumes in morbidly obese end-stage primary, secondary, and obesity-induced LE patients following bariatric surgery.
Conclusions:
Our multiple case study indicates that bariatric surgery provides a good indication for concomitant treatment of morbid obesity and LE.
Introduction
Lymphedema (LE) is a chronic condition of swelling due to lymphatic impairment and is characterized by edema and fibro-adipose tissue deposition. LE may derive from an anomalous development of the lymphatic system, known as primary LE, or may develop secondary to traumatic, infectious, or other external events. 13 In addition, a normal lymphatic system confronted with an overwhelming amount of fluid also leads to LE, as in cases of immobility, disuse, orthostasis, or obesity. If left untreated, LE usually progresses through a series of stages, from stage 0 (subclinical), to a soft pitting state (stage 1), and to finally an irreversible fatty and fibrotic state (stage 3). 4 The condition has major physical, psychological, and social implications for quality of life. 5 Evidence about chronic edema prevalence, including LE, suggests an incidence ranging from 1.33 per thousand to 1.44 per thousand. 6
The worldwide prevalence of overweight and obesity is high and increasing, resulting in increased morbidity risks and mortality. Between 1980 and 2013, the proportion of adults with a body mass index (BMI) higher than 25 kg/m2 increased from 28.8% to 36.9% and from 29.8% to 38.0% in men and women, respectively.7,8 The relationship between obesity and LE is plural and bidirectional. Studies have provided evidence that obesity and postoperative weight gain are significant risk factors for the development and aggravation of secondary LE.9–12 A study concerning the subjective control of chronic edema, including LE, identified obesity as an important factor for poor control of arm and leg swelling. 13 Several other studies described the negative effects of morbid obesity on the lymphatic system and suggested extreme obesity as a novel cause of LE, so-called “obesity-induced LE.”14,15 Finally, several intervention studies targeting LE by weight management and dieting demonstrated positive results.16–20
Bariatric surgery offers the most effective and durable treatment for obesity and exhibits positive effects on obesity-related diseases, such as type 2 diabetes and cardiovascular risk factors. 21 Based on an increasing amount of evidence about the bidirectional interactions between LE and obesity, we explore whether bariatric surgery could improve leg volumes in morbidly obese patients with secondary, primary, and obesity-induced LE. To date, a small number of studies have described the observed and potential benefits of bariatric surgery for the treatment of LE in superobese patients with a BMI above 50 kg/m2.22–26 Less is known about the effects of bariatric surgery in morbidly obese LE patients.
The purpose of this study is to describe changes in leg volumes after bariatric surgery in nine end-stage morbidly obese LE patients.
Methods
Between 2013 and 2019, 829 patients were hospitalized in our Center of Expertise for Lymphovascular Medicine for intensive treatment of their LE. Over this period of time, we identified nine patients who underwent a bariatric procedure related to their morbid obesity. The study was approved by the local Medical Ethics Committee (no. 10/20) and all patients provided written informed consent. Data concerning age, gender, medical diagnosis, LE stage, type of bariatric treatment, body weight, BMI, and limb volumes were retrospectively collected from the patient files. The medical diagnosis was made by the dermatologist according to the prevailing standards of care. Opto-electrical volumetry (Pero-system Messgeräte GmbH, Germany) was used to assess the volume of the legs.
“T0” was defined as the moment of bariatric surgery, “T postop” was defined as the moment with the lowest body weight after the bariatric surgery, and “T last follow-up” was defined as the moment of the last check in our center. At the individual patient level, body weight, BMI, percent total weight loss (%TWL), leg volumes, and their percent reduction at T postop and T last follow-up in comparison to T0 were calculated. At the group level, paired sample t-tests were conducted to compare the mean body weight, BMI, and leg volumes between presurgery and postsurgery. A p-value ≤0.05 was considered to be statistically significant. The data were analyzed with IBM SPSS Statistics for Apple, Version 25.0 (Armonk, NY: IBM Corp, 2017).
Results
At the time of bariatric surgery, all patients had end-stage LE (stage 3) and were morbidly obese. Patients 1 and 2 were diagnosed with cancer treatment-related secondary LE, patients 3–6 were diagnosed with late-onset nonhereditary (primary) LE, and patients 7–9 were diagnosed with obesity-induced LE. All patients were in the stable maintenance phase of treatment, which consisted of therapeutic compression garments and self-management. No further improvement was to be expected from conservative treatment. Presurgery and postsurgery, the patients visited our center for regular follow-up for their LE and for adjustment of the garments. The characteristics of the nine patients at the time of bariatric surgery are shown in Table 1.
Patient Characteristics at the Time of Bariatric Surgery
BMI, body mass index; LE, lymphoedema; ORPHA, nomenclature and coding system.
Table 2 shows the patients' body weight, BMI, and volumes of both legs at the moment of bariatric surgery, at the moment of the lowest postsurgery body weight, and at the moment of the last follow-up in our center. The table also shows the %TWL and the percent reduction of the leg volumes postsurgery in comparison to the moment of bariatric surgery. Patients 5 and 9 had short follow-ups (14 and 12 months, respectively), resulting in an absence of changes between T postop and T last follow-up.
Body Weight, Body Mass Index, Percent Total Weight Loss, Leg Volumes, and Percent Reductions in Comparison to T0
Percentual reductions of Total Weight Loss and Leg Volumes are in comparison to T0.
%TWL, percent total weight loss.
Figure 1 shows the graph of the individual patients during the complete treatment period in our center. The x-axis shows the various time points presurgery and postsurgery with T0 as the moment of surgery. The primary y-axis shows the leg volumes in centiliters, and the secondary y-axis shows the BMI in kg/m2. The blue line represents the volume of the left leg, the green line represents the volume of the right leg, and the yellow line represents BMI. The other patients show the same trends in the graphs
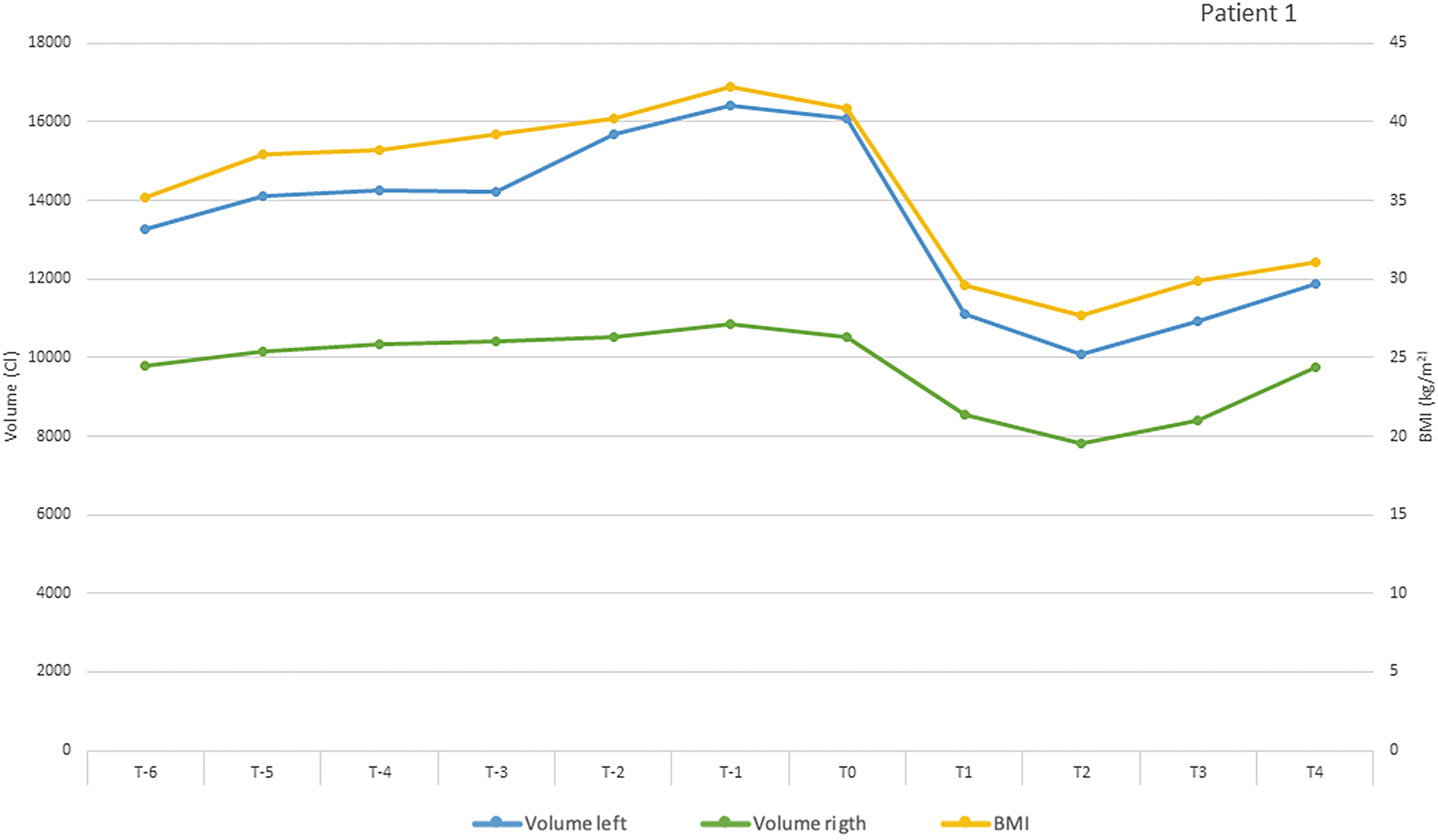
Graph of patient 1 with secondary cancer treatment-related LE. BMI, body mass index; LE, lymphedema.
Table 3 shows the group-level data for mean body weight, BMI, and accompanying leg volumes at the moment of bariatric surgery and postsurgery and the results of the paired sample t-tests.
Group-Level Data for Mean Body Weight, Body Mass Index, and Leg Volumes
T post-op and T last follow-up data are compared with data at T0.
Significant at p < 0.05.
Postsurgery, all patients, irrespective of the etiology of their LE, demonstrated a reduction in body weight, BMI, and the volumes of both legs. The paired sample t-tests showed a significant decrease in body weight, BMI, and leg volumes. In most patients, the volumes of both legs decreased by approximately equal percentages. However, in patients 1 and 6, who had a large volume difference between their left and right leg before surgery, the leg most affected by LE demonstrated higher percent volume reductions, respectively, 37% versus 26% and 51% versus 30%.
Figure 2 shows the photos of patient 1, illustrating the higher percent reduction of the most affected left leg. Patient 8 also showed a large difference between the volumes of the left and right legs at both presurgery and postsurgery, but this was due to a large lump in his right leg. Surgical removal was necessary to treat this lump. During follow-up, all patients remained in a stable situation for body weight, BMI, and leg volumes, taking into account that a small increase in body weight is normal in bariatric patients after a couple of years. The mean length of the follow-up period was 37.4 (standard deviation 17.3) months.

Photos of patient 1, presurgery and postsurgery.
Discussion
Our data demonstrate a significant decrease in body weight, BMI, and leg volumes in morbidly obese end-stage primary, secondary, and obesity-induced LE patients following bariatric surgery. Failing of the lymphatic system can be caused by increased filtration of fluid with an overloaded, initially normal lymphatic system (preload raised) or by “real” lymphatic impairment and/or dysfunction (afterload impairment), or due to a combination of both conditions.
Several mechanisms to explain the negative impact of obesity on lymphatics have been suggested in the literature. 1 First, obesity can raise the preload by an enhanced production of lymph, overwhelming the lymphatic system and leading to lymph stasis. Second, lymphatics can be damaged by long-lasting overload. 27 This reason is supported by a study by Vasileiou et al., 28 who showed that in edematous obese patients, lymphoscintigrams show abnormalities in 35% of the patients. However, they conclude that lymphatic damage is not uncommon; it usually causes delayed drainage at most. Direct mechanical compression by the fatty tissues causing obstruction of the lymphatics may also explain the negative impact of obesity on lymphatics, as well as a decrease in overall mobility and daily activities.
The negative interaction between obesity and LE can be explained by a model developed by Mehrara and Greene 1 in 2014. This model shows the process of impaired lymphatic function leading to chronic interstitial fluid stasis, thereby promoting the activation of inflammatory pathways, which leads to increased fibro-adipose deposition. In turn, fibrosis and adipose deposition further impair lymphatic function, resulting in a feedforward loop and disease progression.
In our patients with late-onset nonhereditary primary LE and cancer treatment-related secondary LE, obesity will probably aggravate the situation by adding a preload component to the already existing and irreversibly impaired afterload. Obesity itself has most likely been the cause of fluid accumulation in the obesity-induced LE group. We speculate that the reduction of the preload and the improved opportunities to exercise and to increase the overall level of daily activities played an important role in the positive results of our patients. Objective monitoring of the daily activity level and assessment of lymph transport capacity could be helpful in understanding the underlying mechanisms of the beneficial effects of weight loss.
Our results also suggest that even part of the stage 3 adipose tissue formation in the legs can be reduced by this weight loss. Future studies should include the description of the LE stage, as this could help to answer questions about the reversibility of the tissue changes in the different stages of LE.
The literature describing weight loss by bariatric surgery as an intervention for LE is currently somewhat scarce. A small number of publications have described these results or have hypothesized about the potential benefits of weight loss by bariatric surgery in LE patients. Greene et al. 15 described the negative effects of morbid obesity on the lymphatic system, based on lymphoscintigrams. They suggested that extreme obesity could be a novel cause of LE, so-called “obesity-induced LE,” with the existence of a BMI threshold between 50 and 60 kg/m2, at which point lymphatic dysfunction could occur for the lower extremities. They speculate that although LE is progressive, the disease might be treated by major weight loss (e.g., bariatric procedure), which might reverse lymphatic insufficiency.
In 2019, Pereira de Godoy et al. 26 published a case report about a 52-year-old female patient with bilateral edema of the feet, corresponding to clinical stage 2 LE. Bariatric surgery decreased her BMI from 51.2 to 37.1 kg/m2, and her clinical LE resolved and remained absent. Conference abstracts by Ratnasingham et al. 22 and Khan et al. 23 described positive results regarding leg volumes after bariatric surgery in obesity-related LE patients with a mean BMI of 74 kg/m2.
Our positive results are in line with these previous observations and expected benefits. To the best of our knowledge, our study is the first to describe the results of bariatric surgery in a population of primary, cancer treatment-related secondary, and obesity-induced LE patients with less extreme BMI levels. The mean BMI of our population was 44.1 kg/m2. Although this multiple case report is limited by its nature, we consider it of importance as it underlines the chances for new treatment options for morbidly obese patients with end-stage LE, irrespective of the etiology.
Conclusions
Our multiple case study indicates that bariatric surgery provides a good indication for concomitant treatment of morbid obesity and LE. The observed positive effects were present in primary, secondary, and obesity-induced LE.
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
The authors received no financial support for the research, authorship, and publication of this article.