
Abstract
Purpose:
To investigate the characteristics of lymphedema in patients treated with mammalian target of rapamycin (mTOR) inhibitors and delineate complex decongestive therapy (CDT) outcomes.
Methods and Results:
We retrospectively analyzed 24 patients with mTOR inhibitor-induced lymphedema and 7 lymphedema patients (control) not treated with mTOR inhibitors, who visited the lymphedema clinic of the department of rehabilitation medicine from March 2016 to December 2019. We comprehensively reviewed clinical features, medication history, associated diseases, lymphoscintigraphy, lower extremity computed tomography venography (LE CTV), and the effect of CDT. By using ImageJ program, we measured the cross-sectional area (CSA) of muscle and subcutaneous fat of mid-thigh image in LE CTV and compared them to a control group not treated with mTOR inhibitors. Seventeen patients on sirolimus and seven patients on everolimus were included, with an approximately equal distribution of stages 2 and 3 lymphedema, and most with pitting edema. Ten patients had breast or gynecological cancer and underwent lymph node dissection. Lymphedema developed after mTOR inhibitor initiation, not postoperatively. Lymphoscintigraphy revealed decreased lymph node uptake and dermal backflow. LE CTV revealed subcutaneous honeycomb-shaped trabecular areas in the affected limbs of seven patients. Patients treated with mTOR inhibitors had a larger mean subcutaneous fat CSA and a smaller mean muscular CSA than controls. Lymphedema improved or remained unchanged after initial CDT. Daily CDT adequately controlled 11 cases, but exacerbation occurred in 5 of 7 poorly compliant patients, and cellulitis occurred in 6 patients.
Conclusion:
Physicians should identify mTOR inhibitor-related lymphedema early and discuss medication alternatives and CDT with patients.
Introduction
Mammalian target of rapamycin (mTOR) inhibitors, including sirolimus (SRL) and everolimus (EVL), is increasingly used as immunosuppressive agents for organ transplant recipients due to their lack of nephrotoxicity. 1 Recently, several mTOR inhibitors have been approved for the treatment of some types of cancers. 2 However, mTOR inhibitors have been reported to be associated with various adverse effects, including, although rare, lymphedema.3–5 Although the clear pathophysiology of mTOR inhibitor-related lymphedema is not understood, mTOR inhibition has been shown to block cytokine-mediated T cell proliferation, and this is related to lymph drainage interference. 1
Lymphedema is characterized by swelling of the affected body part as a result of interstitial accumulation of protein-rich lymph fluid. 6 This leads to fibrosis, hypertrophy of adipose tissue, and recurrent infections, which undermine physical function and cause psychological distress, leading to impaired quality of life. To prevent the progression of the disease and its complications, early detection and management of lymphedema are important.
Because it is a rare complication, previous publications on lymphedema among patients treated with mTOR inhibitors have generally been case reports.1,7–12 The reported patients were diagnosed with mTOR inhibitor-related lymphedema after discontinuation of the medication and observing improvement. Recently, Fourgeaud et al. described the clinical features and outcomes of lymphedema among patients treated with SRL. 13 They reported that patients required complex decongestive therapy (CDT) for the lymphedema, but they did not report CDT outcomes.
The use of mTOR inhibitors is increasing as the frequency of organ transplantation is increasing and more new cancer treatment regimens include mTOR inhibitors. As a result, the incidence of lymphedema among patients treated with mTOR inhibitors is also increasing, although this complication remains rare in absolute terms. Physicians should be aware of the characteristics of lymphedema among patients taking mTOR inhibitors, and the complication should be managed by either stopping the medication or prescribing CDT. This study aimed to investigate the characteristics of lymphedema among patients treated with mTOR inhibitors. In addition, we aimed to delineate CDT outcomes among patients maintained on mTOR inhibitors.
Methods
Study design and participants
We retrospectively reviewed the medical records of patients who visited the lymphedema clinic of the Department of Rehabilitation Medicine of Asan Medical Center from March 2016 to December 2019. This study was approved by the governing institutional review board (IRB) of our hospital (IRB No. 2019-1472). During the period under study, there were 27 patients who underwent organ transplantation before lymphedema developed, among whom, 21 were treated with mTOR inhibitors and included in the study. The remaining six patients were not taking mTOR inhibitors and were, therefore, excluded. We identified an additional three patients with advanced breast cancer who developed lymphedema after an EVL clinical trial. Finally, we enrolled a total of 24 patients with lymphedema after using mTOR inhibitors.
To find out the unique characteristics of mTOR inhibitor-related lymphedema by analyzing lower extremity computed tomography venography (LE CTV), we set up a case group (mTOR inhibitor-related lymphedema, lymphedema patients using mTOR inhibitors) and a control group (cancer-related lymphedema, lymphedema patients not using mTOR inhibitors) for comparison. There were seven patients in the case group, who underwent LE CTV. We enrolled seven age-, gender-, lymphedema site-, and stage-matched patients who were not using mTOR inhibitors, had lower extremity lymphedema, and underwent LE CTV from the same lymphedema clinic in the same period of time as a case group.
Comprehensive review
We comprehensively reviewed clinical characteristics, imaging studies, and CDT outcomes. Captured clinical characteristics included age, gender, body mass index, transplant organ, type of mTOR inhibitor, dose and duration of mTOR inhibitor, lymphedema site, and clinical stage of lymphedema. Lymphedema was diagnosed based on clinical evaluation and lymphoscintigraphy. The clinical stage of lymphedema was determined according to the International Society of Lymphology (ISL) criteria. 14 We also identified accompanying disease and cellulitis history.
We reviewed medical imaging studies for patients who were examined by lymphoscintigraphy or LE CTV. We measured the total cross-sectional area (CSA) of the mid-thigh, along with its muscular and subcutaneous fat components, using ImageJ, version 1.49 K (National Institutes of Health, Bethesda, MD), which distinguished muscle and fat using Hounsfield units15–17 (Fig. 1). The mid-thigh (equidistant from the femoral head and medial femoral condyle) was chosen for the single-slice image because it is the region with the highest muscle mass. 18
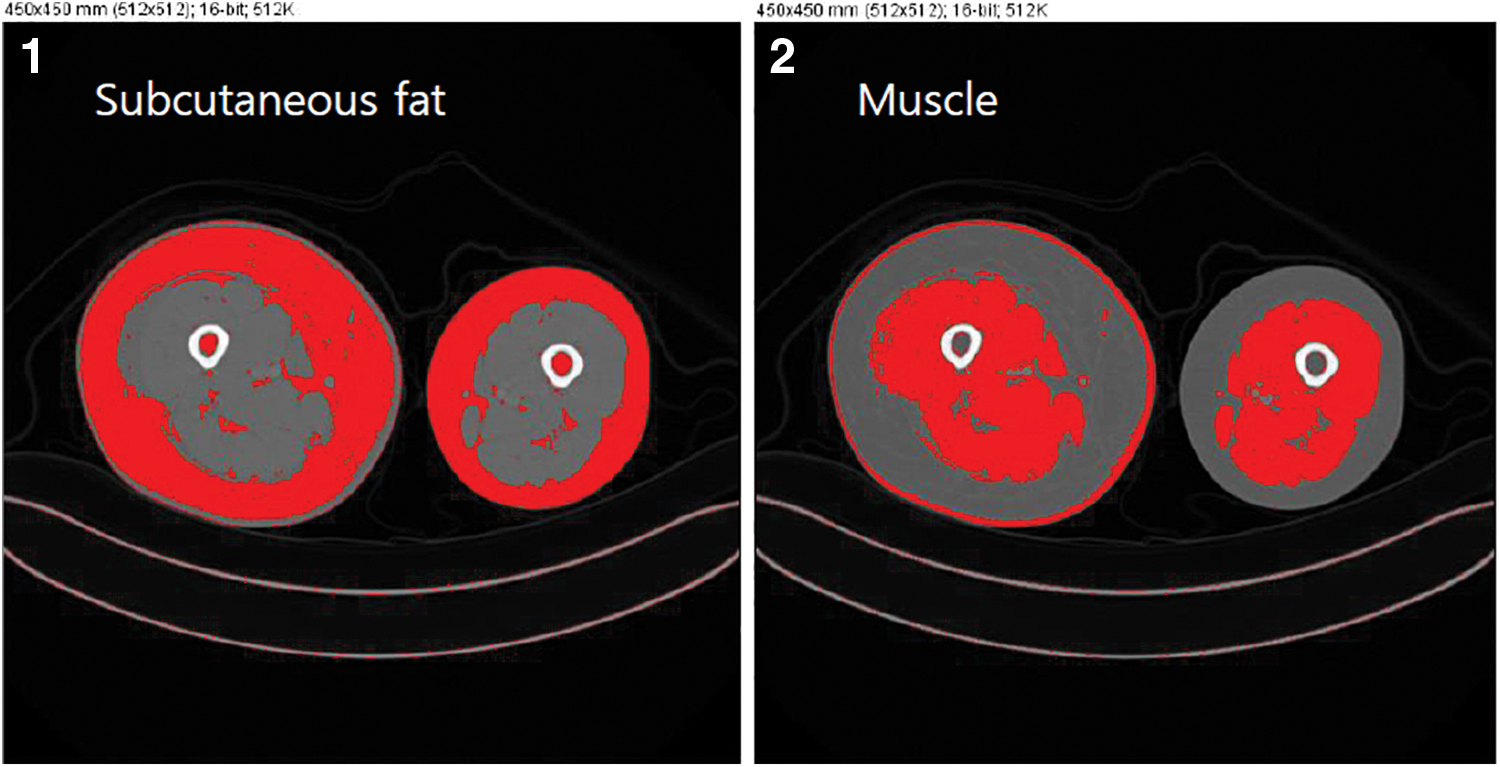
Measuring subcutaneous fat and muscle using mid-thigh computed tomography venography images. (1) Subcutaneous fat in red. HU, 190 to 30. We excluded the red area within muscle and bone marrow. (2) Muscle in red. HU, 0 100. We excluded red area of skin. HU, Hounsfield units. Color images are available online.
The patients underwent 30 minutes of CDT five times per week for 2 weeks. CDT consisted of manual lymphatic drainage, compression of the affected extremity with a low-stretch bandage, exercises to enhance lymphatic drainage, and patient education. The same certified lymphedema therapist, trained by the Dr. Vodder School, performed the treatment. This treatment aimed to achieve substantial lymphedema volume reduction. 19
The volume reduction effects of CDT were estimated based on circumference measurements before and after the 2-week CDT treatment course. Using a tape measure, we checked the circumferences of both legs for patients with lower extremity lymphedema and both arms for patients with upper extremity lymphedema.
Statistical analyses
We conducted descriptive analyses to identify the specific features of lymphedema among patients treated with mTOR inhibitors. For patients who underwent LE CTV, we made between-group comparisons between mTOR inhibitor recipients and controls and within-group comparisons among mTOR inhibitor recipients, using the Mann–Whitney U-test. Data were recorded and analyzed using Predictive Analytics SoftWare Statistics for Windows, version 18.0 (SPSS Inc., Chicago, IL).
Results
A total of 24 lymphedema patients treated with mTOR inhibitors were enrolled; their clinical characteristics are summarized in Table 1. Also, the information of case and control patients who underwent LE CTV is described in Table 2. Seventeen patients were on SRL and seven patients were on EVL. We could not determine the duration of SRL use for two patients who were referred from another hospital without their previous medical records. Therefore, we analyzed the duration of SRL intake for 15 patients. The lymphedema locations varied, and there was an approximately equal distribution of stages 2 and 3 lymphedema. Most patients had pitting edema (Fig. 2). Twelve patients discontinued mTOR inhibitors without significant improvement of their lymphedema. The duration of follow-up after discontinuation was 16.8 ± 14.4 months.

Lower extremity of a 70-year-old woman. She was on sirolimus for 23 months after kidney transplantation. The image shows lymphedema with 3 mm of pitting when compressed with a finger. Color images are available online.
Baseline Characteristics of the Study Subjects
Values are mean ± standard deviation or number, unless otherwise indicated.
BMI, body mass index; mTOR, mammalian target of rapamycin.
Information of the Case and Control Group for Computed Tomography Venography Analysis
F, female; LEx, lower extremity; Lt, left; M, male; Rt, right.
Thirteen patients were diagnosed with cancer. Three patients, who were taking SRL after kidney transplantation without any lymph node dissection, developed Kaposi sarcoma of the limb associated with lymphedema. Among transplant recipients, four developed breast cancer and underwent mastectomy with axillary lymph node dissection. Three of the transplant recipients developed gynecological cancer and underwent pelvic lymph node dissection. These seven patients developed lymphedema after mTOR inhibitor initiation, and five of them had stage 3 lymphedema (Table 3). Three patients using EVL as part of a clinical trial had advanced breast cancer with a history of mastectomy and axillary lymph node dissection; in these patients, lymphedema developed after using EVL, not after surgery. Upper extremity lymphedema developed in two patients and lower extremity lymphedema developed in one patient.
Characteristics of 10 Patients with Cancer and Underwent Lymph Node Dissection
EVL, everolimus; LEx., lower extremity; LND, lymph node dissection; SRL, sirolimus; UEx., upper extremity.
Twenty-three patients were evaluated by lymphoscintigraphy (Fig. 3), 21 exhibiting decreased lymph node uptake in the affected limb and 9 exhibiting dermal backflow. Lymph node uptake was also decreased in patients with mTOR inhibitor-related lymphedema, who had no history of lymph node dissection, as did in patients who underwent lymph node dissection.
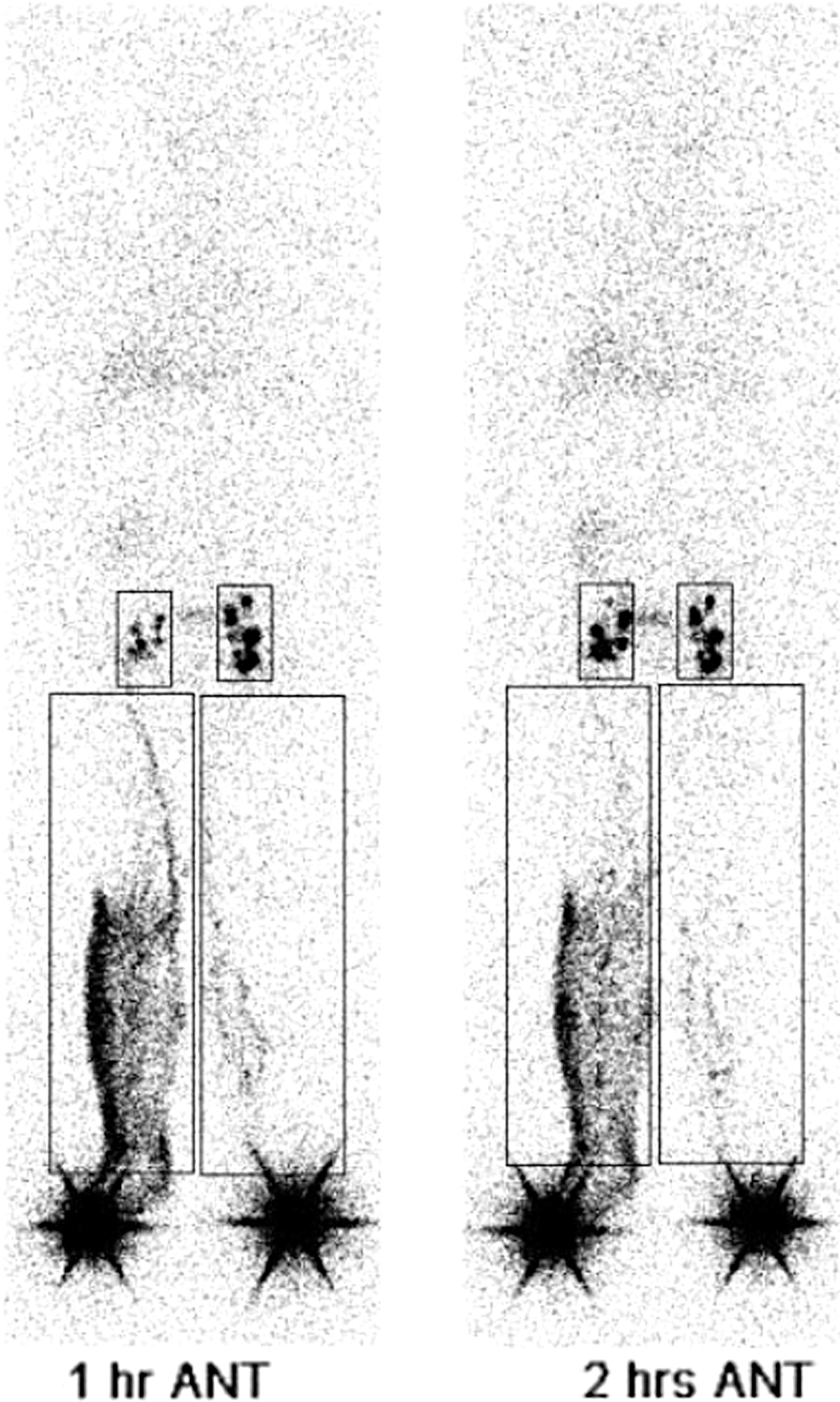
Lower extremity lymphoscintigraphy outputs of a 70-year-old man. He took sirolimus for 10 months after kidney transplantation and had no history of pelvic lymph node dissection. The images show decreased right ilioinguinal lymph node uptake and dermal backflow in the right lower limb.
Seven patients with lower extremity lymphedema underwent LE CTV (Fig. 4). All seven of these patients exhibited peculiar trabecular areas with honeycomb patterns in the subcutaneous fat tissue of the affected limbs.
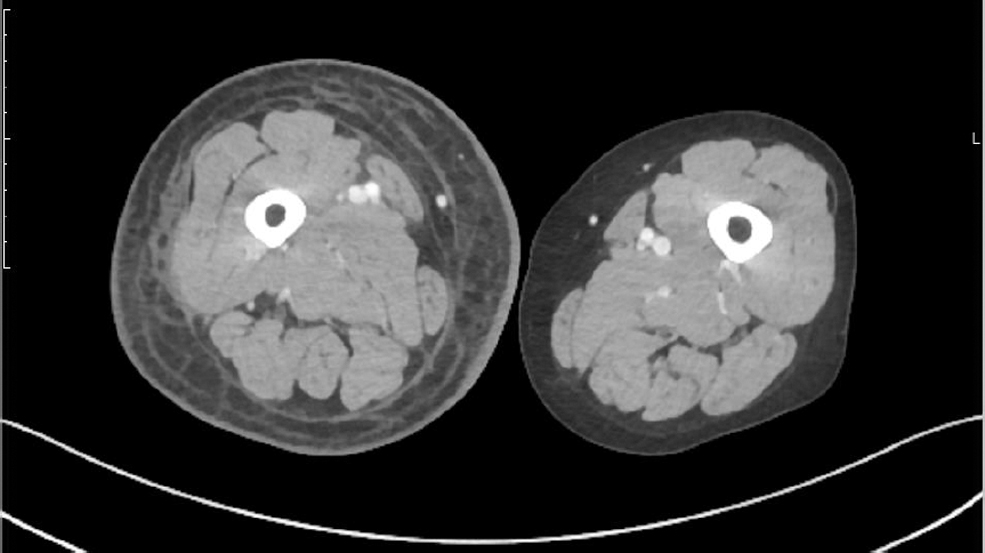
Lower extremity computed tomography venography of a 66-year-old woman. She took everolimus for 22 months after liver transplantation. The image of the right mid-thigh shows a peculiar trabecular area with a honeycomb pattern in the subcutaneous fat, signifying fluid within the subcutaneous fat.
We compared total, muscle, and subcutaneous fat CSA at the mid-thigh between cases and controls using LE CTV (Table 4). Comparison was done between the case and control group, and among the four subgroups; lymphedematous limbs of the case group, normal limbs of the case group, lymphedematous limbs of the control group, and normal limbs of the control group. The total CSA ratio (the ratio of the total CSA of lymphedematous limbs to that of the normal limbs) was higher in a case group. Among the four subgroups, the lymphedematous limbs of the case group had the lowest mean percent contribution to CSA by muscle and the highest mean contribution by subcutaneous fat. The lymphedematous limbs of the case group also had the highest mean fat-to-muscle ratio. However, the Mann–Whitney U-test revealed that these differences were not statistically significant.
Comparison of Total, Muscular, and Subcutaneous Fat Cross-Sectional Area at the Mid-Thigh on Lower Extremity Computed Tomography Venography
Values are mean ± standard deviation unless otherwise indicated. Seven patients in each group—five unilateral and two bilateral lymphedema each.
For treatment, 22 patients needed CDT, including bandaging, and 2 patients were managed with compression stockings. Nineteen patients underwent an initial intensive phase of CDT at the study hospital, and five patients underwent the initial phase at another hospital because of accessibility. After 2 weeks of treatment, the circumference of the affected limbs reduced in 12 patients, but 7 patients showed no definite reduction (Table 5). During the maintenance phase of CDT, 18 patients were followed up at the lymphedema clinic and had the circumferences of their affected and unaffected limbs measured at the same level.
Effects of Complex Decongestive Therapy
Discussion
In this study, we identified distinct characteristics of lymphedema among patients treated with mTOR inhibitors. Our findings were generated from a comprehensive review of clinical features, lymphoscintigraphy findings, and CT findings, derived from a larger sample than previous studies. To our knowledge, this was the first study to analyze muscular and subcutaneous fat components in mTOR inhibitor-related lymphedema patients using LE CTV. We also identified the effects of CDT in such patients for the first time.
The clinical features of lymphedema were similar to a previous study. 13 Lymphedema involved both the upper and lower limbs, without a gender predominance, and the mean interval between lymphedema onset and mTOR inhibitor initiation was 12 months. In addition, we classified the clinical stage of lymphedema based on ISL criteria and identified that most were stage 2 or stage 3. To the best of our knowledge, we were the first to delineate the severity of lymphedema in a subset of patients with mTOR inhibitor-induced lymphedema using the ISL criteria.
In this study, patients who discontinued mTOR inhibitors showed no significant improvement of their lymphedema. In previously reported cases, early withdrawal of mTOR inhibitors led to partial or complete resolution of lymphedema after several months.9,20–24 However, when the medication was continued for a longer period after lymphedema development, cessation had no significant effect on improvement. 10 Therefore, it is important that physicians detect lymphedema and consider cessation of mTOR inhibitors as soon as possible to prevent permanent lymphedema.
Lymphoscintigraphy revealed decreased lymph node uptake and dermal backflow of the affected limbs. Dermal backflow means a dilatation of initial and minor lymphatics and formation of collateral flow pathways along the subdermal and subepidermal lymphatic plexuses. 25 It is noteworthy that mTOR inhibitor-related lymphedema, without lymph node dissection associated with lymphedema limbs, by itself decreases lymph node uptake. These findings indicate lymph drainage interference.
Although the pathophysiologic mechanism of mTOR inhibitor-related lymphedema is not yet clear, there are several hypotheses. Kerjaschki suggested that mTOR inhibitors may disturb vascular endothelial growth factors C and D, which are key elements for lymphatic survival, proliferation, and migration by inactivating phosphatidylinositol-3′-kinase (PI3K). 26 PI3K is also deeply involved in calcium ion channel signaling, an essential mechanism of pacemaker cells in lymphatic contraction. Huber et al. reported that these drugs can reduce both regenerative and malignant lymphangiogenesis through the inhibition of lymphatic endothelial cells. 27
Moreover, Aboujaoude et al. have hypothesized that taking mTOR inhibitors may block cytokine-mediated T cell proliferation, which is the main mechanism of mTOR action, then increase vascular permeability and subsequently trigger the overproduction of interstitial fluid. 28 On the other hand, with a role in lymphangiogenesis, SRL has also been studied for treatment of lymphatic malformation. 29 Further studies about pathophysiologic mechanism of mTOR inhibitor-related lymphedema are needed.
There were 10 patients with cancer, who underwent surgical removal of regional lymph nodes. Lymphedema onset only ever occurred after mTOR inhibitor initiation among the study patients. All, but one patient developed lymphedema on the same side of the lymph node dissection. We hypothesize that, among these patients, latent lymphedema became overt or aggravated by mTOR inhibitor-induced activity.
Lymphedema associated with mTOR inhibitor use seems to have a tendency to promote fluid and fat accumulation. Most patients with mTOR inhibitors-related lymphedema in our study had pitting edema. In addition, on LE CTV images, the lymphedematous limbs of patients taking mTOR inhibitors showed peculiar trabecular areas with honeycomb patterns in the subcutaneous fat, signifying fluid and fibrotic tissue surrounding the adipose tissue accumulation.30,31 LE CTV images demonstrate the alteration in epidermal and subcutaneous tissue. 32
By measuring the muscular, subcutaneous fat, and total mid-thigh CSA, we analyzed not only qualitative but also quantitative LE CTV findings. The case group had a larger mean subcutaneous fat CSA and a smaller mean muscular component than the control group. The nonaffected limbs of both the case and control groups had similar muscle and fat distributions to one another. Although the CSA differences were not statistically significant—likely owing to the small sample size—we should not overlook these differences. Higher proportions of fluid and fat are associated with less fibrosis in lymphedema. Lawrence and Nho 33 suggested a role of mTOR inhibitors in modulating fibrosis and use as a therapeutic agent against pulmonary fibrosis. We hypothesize that mTOR inhibitors may disrupt the fibrosis process in lymphedema. 33
Cellulitis developed in 6 (33.3%) of 18 continuously followed-up patients. This rate was much higher than the known prevalence of cellulitis among patients with lymphedema, 7.95% (Ref. 34 ). Lymphedema itself, along with transplantation and immunosuppressive medications, are known risk factors for cellulitis. 35 Therefore, there is a particularly high risk of cellulitis among patients taking mTOR inhibitors.
CDT is a standard conservative treatment for lymphedema. We verified the effects of CDT against mTOR inhibitor-related lymphedema. The initial intensive phase was helpful for volume reduction or preventing aggravation. In the maintenance phase, compliance was an important factor. When stockings and bandages were applied daily, lymphedema did not worsen. Physicians should advise their patients appropriately to achieve good compliance. These are consistent with the effects of CDT in patients with lymphedema not related to mTOR inhibitors. Yamamoto et al. showed a decrease of about 70% in lymphedema volume within the 1st week of initial intensive phase of CDT. 36 Johnstone et al. identified that more compliant patients maintain the better status of lymphedema than noncompliant patients. 37
This study had several limitations. First, because this was a retrospective study conducted at a single center, selection bias may have existed. Second, since mTOR inhibitor-related lymphedema is a rare complication, the sample size was small. Future multicenter studies with larger sample sizes are warranted.
Conclusion
As the use of mTOR inhibitors is increasing, the chances of encountering patients with mTOR inhibitor-related lymphedema are also increasing. This complication manifests as pitting edema on physical examination, decreased lymph node uptake on lymphoscintigraphy, and a large subcutaneous fat component with a peculiar pattern on LE CTV. Physicians should identify its presence early and discuss medication changes and CDT with their patients. Patients should be aware of the risk of cellulitis and the importance of daily CDT.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.