
Abstract
Background:
Bioimpedance spectroscopy (BIS) devices are routinely used in the assessment of breast cancer-related lymphedema (BCRL). The equipotential electrode placement is a commonly used protocol for the assessment of BCRL. However, the sternal notch electrode placement protocol is also in use. Whether these two protocols are interchangeable is not known.
Methods and Results:
Ethical approval was received from the institutional ethics committee at Tata Memorial Hospital, India. BIS measurements (whole-body right side and affected and unaffected arms) of 100 women with or at risk of BCRL were measured using equipotential and sternal notch protocols. Resistance at zero frequency (R0) was determined, and agreement of the absolute R0 values and the R0 ratio (unaffected/affected) between protocols was evaluated (Bland–Altman analysis and Passing–Bablok regression analysis). Mean absolute differences between protocols were very small for whole-body right side, affected arm, unaffected arm, and the interarm ratio at 0.23 ohms (95% confidence interval [CI]: −3.8 to 4.3), −5.7 ohms (95% CI: −7.5 to −3.9), −9.09 ohms (95% CI: −11.4 to −6.8), and −0.008 ohms (95% CI: −0.02 to 0.001), respectively. Limits of agreement (two standard deviation) between protocols were narrow for whole-body right side, affected arm, unaffected arm, and interarm ratio without any systematic or proportional differences for whole-body right side and the interarm ratio (5.8% to −5.6%, 3.7% to −7.4%, 3.5% to −8.2%, and 5.8% to −5.6%, respectively).
Conclusion:
The equipotential and sternal notch protocols could be used interchangeably in BCRL assessment.
The Clinical Trial Registration number: CTRI/2017/12/010762.
Introduction
Breast cancer-related lymphedema (BCRL) commences as an accumulation of protein-rich fluid in the extracellular space of the arm on the side of breast cancer. 1 Prevention of tissue changes and the associated poor quality of life that occur with chronic BCRL require timely diagnosis and early intervention.2–4 Bioimpedance spectroscopy (BIS) has the potential to detect early changes in the extracellular fluid (ECF), including lymph, hence it is widely used for early detection and intervention of BCRL.3,5–7 BIS has been demonstrated to be both reliable and valid in BCRL assessment.8–10
BIS devices measure the impedance (opposition) of tissues to a harmless, low-voltage, alternating electric current passed through a body segment by electrodes attached to the skin.11,12 For measuring impedance, two pairs of electrodes are used; a pair of current drive electrodes and a pair of measurement electrodes spanning the region of interest. To assess BCRL, the impedance of the unaffected and affected arms is measured; the interarm ratio of impedance values (unaffected to affected arm) is compared with a normatively determined threshold or with the preoperative interarm ratio.13–15 Absolute impedance and the interarm ratio of impedance may potentially be altered if the distance between the current drive electrodes and the space between the current drive electrode and the measurement electrode are not consistent.12,15,16 Electrode placement in both arms, therefore, must be consistent and reliable.
The equipotential electrode placement protocol has been widely adopted for measurement of arm impedance.12,16 Normative thresholds of the interarm ratio used for detecting BCRL have been determined using this electrode placement protocol.17–20 However, an alternative electrode placement protocol, the sternal notch protocol, is also used by some commercially available BIS devices. These two electrode placement protocols differ in two respects: (1) the interelectrode distance between the measurement electrodes and (2) the current drive electrode position in relation to the measurement electrodes. Since both these differences may potentially alter the impedance measured, it is imperative to evaluate the interchangeability of these two protocols for assessment of BCRL.
The aim of this study was, therefore, to determine whether the equipotential and sternal notch electrode placement protocols are interchangeable in the assessment of BCRL by evaluating the agreement and the systematic and proportional differences between the impedance of the whole-body right side, unaffected arm, and affected arm and the interarm ratio of impedance.
Materials and Methods
A cross-sectional study was conducted at Tata Memorial Hospital, a tertiary cancer care center in Mumbai, India. Ethical approval for this study was obtained from the institutional ethics committee, and the protocol was registered prospectively at the Clinical Trials Registry of India. All participants provided voluntary, written informed consent before enrollment into the study. A purposive sample of women who had or were at risk of unilateral lymphedema following completion of breast cancer treatment participated in this study. Women were excluded if they were pregnant, had a pacemaker, had a recurrent or metastatic disease, or were under the age of 18 years. Data on 100 women were collected.
Participant demographics
The participants' characteristics, including date of birth, hand dominance, menopausal status, and history of lymphedema treatment, were collected through structured interviews. Details of breast cancer treatment were obtained from electronic medical records and case files. The height of the participants was measured using a wall-mounted stadiometer (Libra, India) to the nearest 0.5 cm. Weight, while wearing light clothing, was measured using a digital weighing scale (Sknol, model number 7281) to the nearest 0.1 kg. Ninety percent of women had more than five axillary lymph nodes excised as part of their breast cancer treatment. Seventy-nine percent of participants were diagnostically identified to have BCRL, determined by the increase in circumference at any single site greater than the normative cutoff values (Table 1). 21
Participant Characteristics
Determined by the increase in circumference at any single site greater than normative values. 21
SD, standard deviation.
BIS measurements
Device reliability
Two different BIS devices, SFB7 (ImpediMed Ltd., Australia) and MS5000 (Bodystat Ltd., United Kingdom) for equipotential and sternal notch electrode placement protocols, respectively, were used to measure impedance values. The device reliability and interdevice electronic comparability were assessed with test artifacts, otherwise known as test cells, supplied by each manufacturer. The SFB7 device was provided with a resistor–resistor/capacitor (RRC) circuit, whereas the MS5000 device was supplied with a simple resistor. Both test artifacts were measured three times with each BIS device according to the manufacturers' instructions.
Comparison of measurement protocols—in vivo
Participants emptied their bladders and removed any metal jewelry before the BIS assessment. Participants were placed in supine position on a nonconductive plinth, with arms and legs slightly abducted away from the midline to make sure they were not touching other parts of the body. They rested in this position for 5 minutes before the measurement was undertaken. The skin at the sites of electrode placement was cleaned with an alcohol wipe before placement of electrodes. Electrodes were placed to measure the whole-body right side, right arm, and left arm. The positioning of electrode placement was device dependent for the arm measurements.
Whole-body right side measurement for both devices
For measuring the whole-body right side, one measurement electrode was placed at the midpoint between the ulnar and radial styloid processes on the dorsum of the wrist, while the other measurement electrode was placed in front of the ankle, between the medial and lateral malleoli. Current drive electrodes were placed 5 cm distal to the measurement electrodes (Fig. 1a).
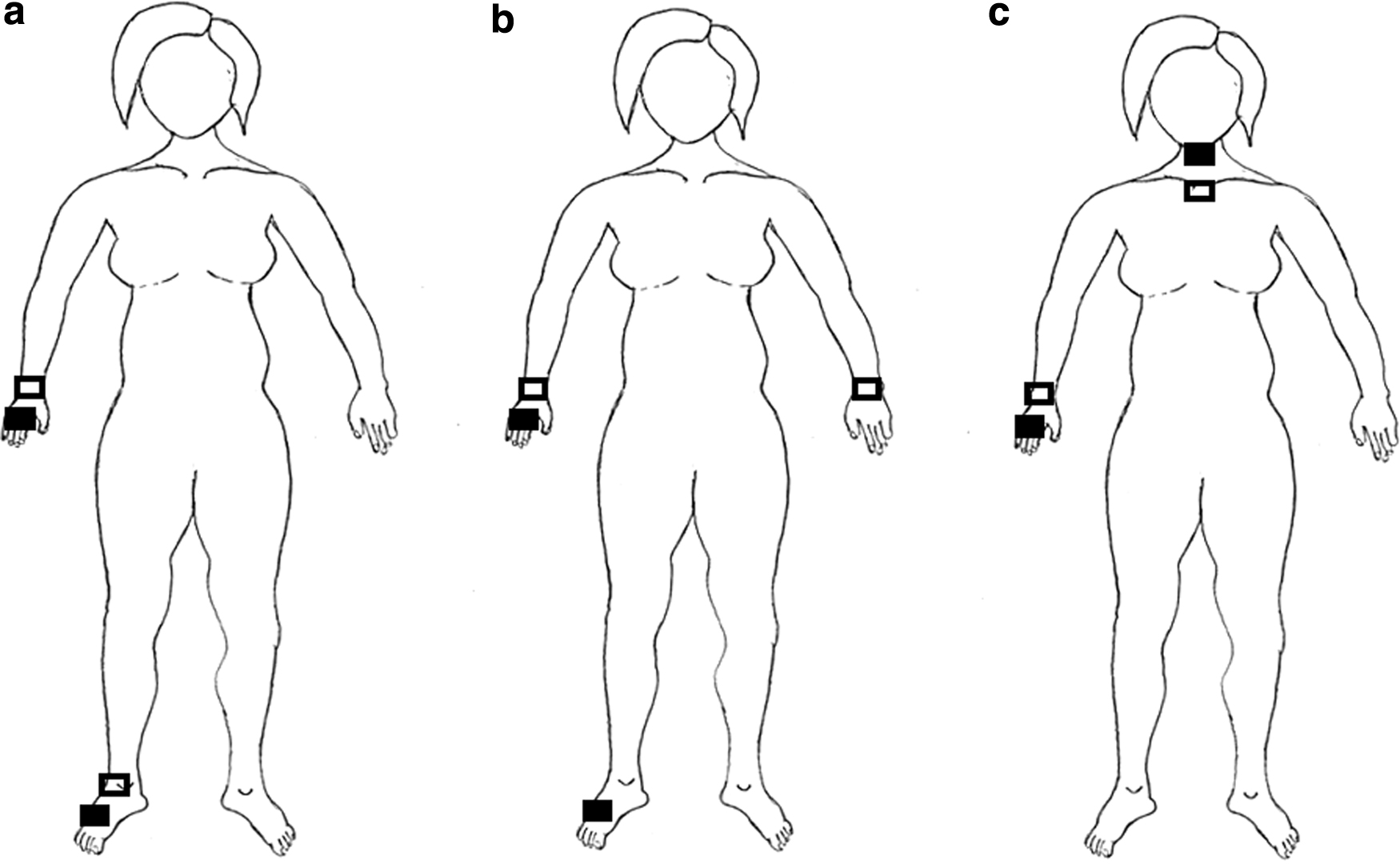
Electrode placement:
Arm measurement—equipotential protocol
The electrodes were placed as per Cornish et al. 12 Briefly, to measure right arm impedance, the measurement electrodes were placed in the midpoint between the ulnar and radial styloid processes on the dorsum of each wrist. One current drive electrode was placed 5 cm distal to the right measurement electrode, and the other measurement electrode was placed on the dorsum of the right foot, 5 cm below the midpoint between medial and lateral malleoli (Fig. 1b). For the left arm impedance measurement, electrodes were placed in a mirror image position to that of the right arm electrode placement.
Arm measurement—sternal notch protocol
For measurement of the right arm, one measurement electrode was placed at the midpoint between the ulnar and radial styloid processes on the dorsum of the right wrist and the other measurement electrode was placed across the sternoclavicular joint. The current drive electrodes were placed 5 cm distal to the measurement electrodes (Fig. 1c). For measurement of left arm impedance, electrodes were placed in a mirror image position to that of the right arm electrode placement.
All BIS measurements were performed according to the instructions provided by their respective manufacturers. For the equipotential protocol, single-tab, ECG-style disposable electrodes (Ag/AgCl, Ref: F3001ECG; FIAB, Italy), with a size (23 × 25 mm) similar to the manufacturer's bioimpedance electrodes, were used with the SFB7 device. 15 For the sternal notch protocol, single-tab electrodes (Bodystat – 0525, LOT 180307-0645), sized 23 × 45 mm, issued by the manufacturer were used with the MS5000 device.
Data acquisition
Both impedance devices were calibrated according to the manufacturer's instructions at the beginning and at frequent intervals after that to ensure consistent measurement. The SFB7 device recorded resistance and reactance at 256 logarithmically spaced frequencies in the range of 3 to 1000 kHz, whereas the MS5000 device recorded 50 logarithmically spaced frequencies in the range 5 to 1000 kHz. Impedance data were transferred from SFB7 and MS5000 devices to a computer using Bioimp, version 5.4.0.3 (ImpediMed Ltd.), and BIOBIS, version 2.15 (Bodystat Ltd.), software, respectively. Both software programs use curve-fitting procedures to extrapolate the measured resistance and reactance data—two components of impedance—to estimate impedance at zero frequency (R0). The impedance at zero frequency is inversely proportional to the volume of the ECF. The impedance ratio of the arms was calculated by dividing R0 of the unaffected arm (contralateral to the operated side arm) by R0 of the affected arm (operated side arm).
Data analysis
Participants' clinical characteristics were analyzed using descriptive statistics and presented either as mean and standard deviation or as percentages. The reliability of devices was assessed using the coefficient of variation (CV). Paired t-tests were used to compare mean R0 values between both electrode placement protocols. Agreement between the electrode placement protocols was evaluated using both the Bland–Altman plot and Passing–Bablok regression analysis.22–26 Limits of maximum acceptable differences were defined as 9% to −9% for the interarm ratio, based on the two standard deviations of the impedance ratio of arms from the 596 healthy participants. 19 The Passing–Bablok regression evaluates whether there are any systematic and proportional differences between the electrode placement protocols. There are no systematic differences between data from each electrode protocol if the 95% confidence interval (CI) of the intercept includes zero in the Passing–Bablok regression analysis. Furthermore, there are no proportional differences between data from each electrode protocol if the 95% CI of the slope includes one in the Passing–Bablok regression analysis. The descriptive statistics and t-test were performed using SPSS® Statistics, version 26 (IBM®), and all other analyses were performed using MedCalc®, version 19.1 (MedCalc software, Belgium).
Results
Device reliability
Both devices exhibited a high degree of technical reproducibility. The CV for repeat measurements for both devices was minimal, irrespective of device and test artifact combination (Table 2). Both devices measured near-identical R0 values for the RRC circuit. However, both devices did not measure near-identical R0 values for the simple resistor. The MS5000 device measured significantly higher impedance than the SFB7 device in a simple resistor (5.3 ohms; 95% CI: 4.6 to 5.9; p < 0.002). The impedance measured with the MS5000 device was also significantly higher than the nominal value of the simple resistor (500 ohms).
Comparison of Instruments with Test Artifacts and In Vivo Testing Using Identical Electrode Placement
CI, confidence interval; CV, coefficient of variation; RRC, resistor–resistor/capacitor; SD, standard deviation.
Measurements—in vivo
Whole body
The mean difference (bias) between the R0 values of both devices was not significant (0.26 ohms; 95% CI: −3.8 to 4.3; p = 0.9) and two standard deviation limits of agreement were narrow (5.8% to −5.6%). Both devices exhibited excellent correlation and did not show any systematic or proportional differences (Spearman's ρ = 0.97; 95% CI: 0.95 to 0.98) (Table 3 and Fig. 2b).
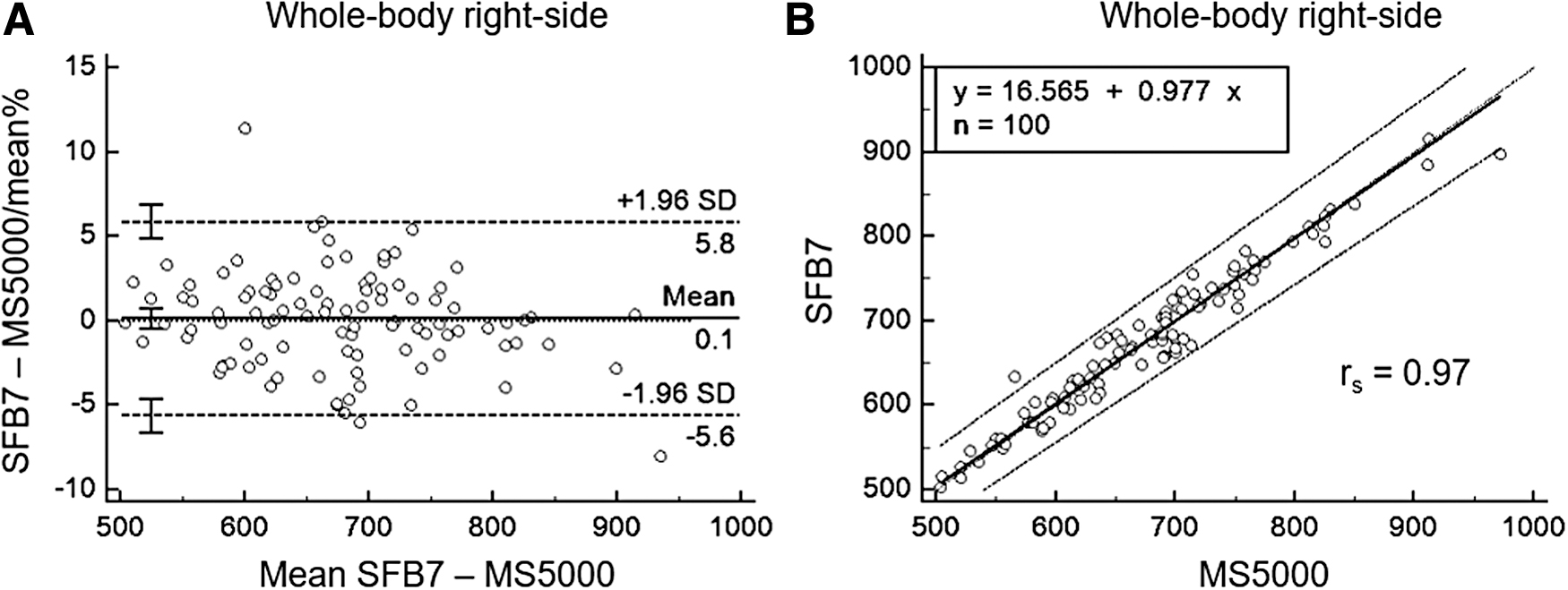
Method comparison of R0 value of whole-body right side measured by SFB7 and MS5000 devices:
Passing and Bablok Regression Analysis
Cusum test of linearity.
A, affected; CI, confidence interval; RSD, residual standard deviation; RWB, whole-body right side; UA unaffected.
Arm R0
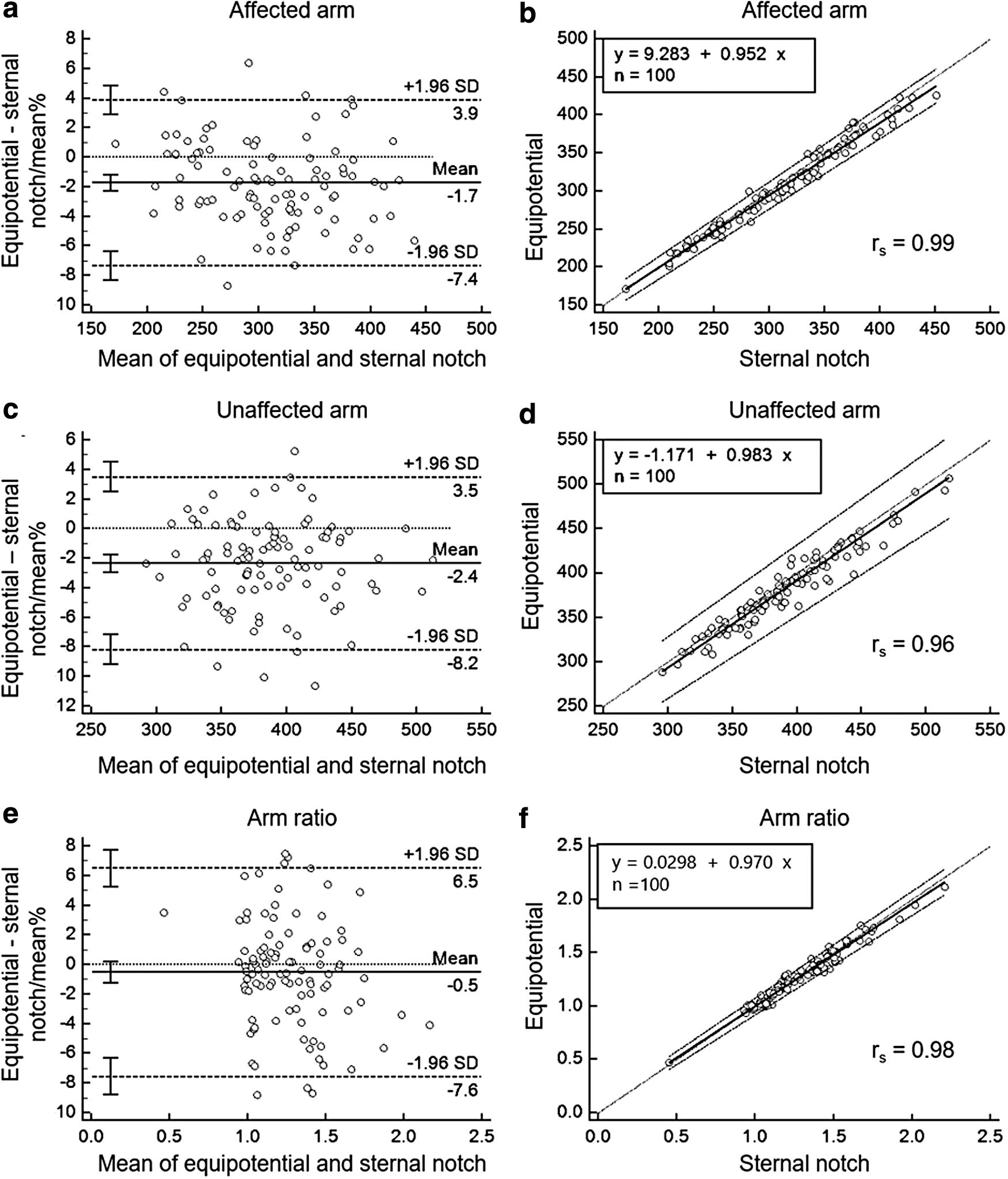
Mean differences (bias) between equipotential and sternal notch protocols for both the affected arm and unaffected arm were small, but significant (−5.71 ohms; 95% CI: −7.5 to −3.9; p < 0.001, and −9.09 ohms; 95% CI: −11.4 to −6.8; p < 0.001, respectively) (Table 4). Limits of agreement, however, were narrow for both the affected and unaffected arms (3.7% to −7.4% and 3.5% to −8.2%, respectively; Fig. 3a, c). Both protocols were also highly correlated in the affected and unaffected arms and did not show any systematic or proportional differences (Spearman's ρ = 0.99; 95% CI: 0.98 to 0.99 and Spearman's ρ = 0.96; 95% CI: 0.95 to 0.98, respectively) (Table 3 and Fig. 3b, d).
Method comparison of equipotential and sternal notch protocols:
Mean Difference of Equipotential and Sternal Protocols
Interarm R0 ratio
Mean differences (bias) between equipotential and sternal notch protocols for the R0 ratio were not significant (−0.008 ohms; 95% CI: −0.18 to 0.001; p = 0.07). The agreement limits were narrower than the a priori defined agreement limit (5.8% to −5.6% vs. −9% to 9%). Both electrode placement protocols were highly correlated in the interarm R0 ratio and did not show any systematic or proportional difference (Spearman's ρ = 0.98; 95% CI: 0.97 to 0.99) (Table 3 and Fig. 3e).
Discussion
This study shows that the equipotential and sternal notch electrode placement protocols are interchangeable for assessment of BCRL. The evidence for interchangeability of these two protocols is that the agreement between both electrode placement protocols is narrow and there are no systematic or proportional differences between both electrode placement protocols for the whole-body right side, affected arms, unaffected arms, and interarm ratio. Reliability between both SFB7 and MS5000 devices used in this study was good despite there being differences between the devices.
In clinical practice, the interarm ratio of R0 is used to inform the presence of, and change in, BCRL over time. This ratio, or its equivalent L-Dex score, 10 is the impedance analog of the interarm volume or interarm circumference differences used to assess lymphedema quantitatively. The present study showed that the R0 ratio of the arms measured by the equipotential and sternal notch protocols was in close agreement without any significant systematic or proportional bias. Limits of agreement for the interarm ratio found in this study (5.8% to −5.6%) were within acceptable limits (9% to −9%) calculated from the standard deviation of the impedance assessment of 596 healthy participants. 19
The narrow agreement limit and lack of systematic or proportional differences indicate that both electrode placement protocols could be used interchangeably for assessing BCRL. More importantly, this level of agreement also demonstrates that R0 ratios determined using the sternal notch electrode placement protocol could be compared with existing normative ranges established using the equipotential electrode placement protocol.
There was excellent agreement between both equipotential and sternal notch protocols in R0 values of the arms, irrespective of lymphedema status. However, R0 values were significantly different between the two electrode placement protocols. This difference is unlikely to be due to technical measurement differences between the two devices since technical reliability between both SFB7 and MS5000 devices was good especially for the RRC circuit, which more closely models the impedance response of biological tissues than a simple resistor.
The sternal notch protocol estimated significantly higher mean R0 values than the equipotential method in both unaffected and affected arms. This difference in absolute R0 values is not surprising since the interelectrode distance between the measurement electrodes is different between the protocols. For the sternal notch protocol, this distance is essentially equivalent to the linear distance between the electrode on the wrist and the electrode on the sternal notch. In contrast, for the equipotential protocol, while the position of the wrist electrode is defined, the exact position of the proximal electrode is virtual. The position of this virtual electrode is located somewhere in the axilla region on the equipotential line. 12 This position is unknown, but it is symmetrically located for each arm, which allows for an acceptable calculation of R0 interarm ratios.12,16
It is likely that the higher R0 value seen for the sternal notch protocol is due to the distance between the measurement electrode at the sternal notch and the current drive electrode on the neck differing from that of the corresponding electrodes in the equipotential protocol.27,28 A decrease in the distance between the current and measurement electrodes has been observed to significantly increase the R0 value in other studies.15,16 That the difference in absolute R0 values is small given the proportionally much larger difference in interelectrode distance between protocols may seem surprising, but is explained by the fact that much of the additional interelectrode distance is in the upper quadrant of the chest with a larger cross-sectional area than the arm. Resistance decreases with increasing cross-sectional area and hence yields a small increase in resistance than otherwise expected on the basis of an increased linear distance. 16
The SFB7 and MS5000 devices used in this study differ in two respects. First, the number of frequencies to estimate R0 is different. Although both SFB7 and MS5000 BIS devices use the Cole modeling methods to estimate R0, the two devices use measurements obtained at 256 and 50 frequencies, respectively. The precision of R0 values estimated by these BIS devices is dependent on the number of frequencies used to estimate R0.12,29,30 However, 50 frequencies comfortably exceed the minimum number (>15) of frequencies recommended to provide accuracy of estimation. 31 Second, the surface area of tab electrodes used by these two devices is different. Although both SFB7 and MS5000 BIS devices use Ag/AgCl single-tab electrodes, the respective surface areas are 23 × 25 mm and 23 × 45 mm. Variability in the surface area of electrodes has been shown to produce variation in the estimation of R0 values. 15
Despite these differences, they provided nearly identical absolute R0 measurements when used on test artifacts or when measuring in vivo using the same electrode placements, that is, whole-body right side measurements. These findings also suggest that the two measurement protocols are BIS instrument agnostic. Practically, however, while the SFB7 device could be used with either electrode arrangement, the MS5000 device can only be used with the sternal notch arrangement as the electrode leads are too short to span the distance between the wrists while keeping the arms abducted on either side of the trunk.
A limitation of the study should be recognized. Although the devices showed a high degree of technical reliability, absolute accuracy was not assessed. Both devices measured the test artifacts within manufacturers' specifications. However, the significant difference between devices when measuring a simple resistor, but not when measuring an RRC circuit, is intriguing. It implies a technical difference in measurement that deserves further study. In practice, however, this may be of limited concern since the human body is more correctly represented as an aggregation of RRC circuits than simple resistors. 32 Normative resistance ratios have not been established using the sternal notch protocol. The present data suggest that equipotential-derived ranges may be used; however, this should be confirmed.
Conclusion
The equipotential and sternal notch electrode placement protocols are interchangeable in the assessment of BCRL. Confirmation of normatively determined diagnostic thresholds for use with the sternal notch protocol is desirable.
Footnotes
Acknowledgments
The authors acknowledge Rajendra Badwe, Nita Nair, Vani Parmar, Shalaka Joshi, Seema Ghulia, Rajiv Sarin, and Sudeep Gupta for their contribution in participant recruitment; Ajeeta Kulkarni and Sarika G Mahajan for participant recruitment and data collection; and Durga Gadgil for her guidance and support in trial registration with Clinical Trials Registry of India.
Author Disclosure Statement
Author Ward provides consultancy services to ImpediMed Ltd., manufacturer of the SFB7 device used in this study. ImpediMed Ltd. had no input into the design, execution, or reporting of this study. Bodystat provided the electrodes for the MS5000 device for free. Bodystat Ltd. had no input into the design, execution, or reporting of this study.
Funding Information
V. Paramanadam was supported by a University of Sydney International Scholarship—Strategic (USydIS). No other funding was received to support this research.