
Abstract
Background:
The Australian Lymphoedema Education, Research and Treatment Program (ALERT) at Macquarie University in Sydney, Australia is one of the flagship programs of Australia's first fully integrated academic health sciences centre, MQ Health. The aim of this study was to describe our findings of compensatory drainage demonstrated by indocyanine green (ICG) lymphography in cancer-related upper and lower limb lymphedema and how this may be translated into clinical practice.
Methods and Results:
Retrospective data from 339 patients aged between 18 and 90 years with secondary cancer-related unilateral or bilateral lymphedema of the upper or lower limb who underwent ICG lymphography assessment at the ALERT clinic between February 2017 and March 2020 were analyzed. In patients with upper limb lymphedema, the ipsilateral axilla was the most frequent drainage region (74.9%), followed by clavicular (41.8%) and parasternal (11.3%). For patients with mild upper limb lymphedema, 94.4% drained to the ipsilateral axilla. No patients drained to the ipsilateral inguinal region. For lower limb lymphedema, drainage to the ipsilateral inguinal was most common (52.3%), followed by contralateral inguinal (30.7%), popliteal (26.1%), and gluteal (21.6%) regions. Three main patterns of superficial lymphatic compensation were identified based on which anatomical structure carried lymph fluid. Manual lymphatic drainage (MLD) was used to facilitate movement of the dye. A light/effleurage technique was sufficient to move the dye through patent lymphatic vessels; a slow and firmer technique was required to move the dye through areas of bridging dermal backflow.
Conclusion:
The introduction of ICG lymphography to our program and its use in guiding personalized conservative management plans, including facilitative MLD techniques, has translated into clinical practice and changed research and educational priorities within the ALERT program.
Introduction
Lymphedema is a chronic inflammatory condition that is the result of a functional overload of the lymphatic system whereby the lymph volume exceeds lymphatic transport capacity. 1 Lymphedema is a poorly understood and under-researched condition that can significantly impact physical and psychological function, reduce quality of life, and result in substantial cost burdens to both patients and the health care system.2–9 The Australian Lymphoedema Education, Research and Treatment Program (ALERT) at Macquarie University in Sydney, Australia is one of the flagship programs of MQ Health, Australia's first fully integrated academic health sciences center under a university's leadership, combining excellence in clinical care with teaching and research. ALERT's integrated and transdisciplinary approach is designed to deliver holistic personalized patient care and treatment informed directly by world-renowned research and continuous learning for improved patient outcomes, enhanced student experiences, and a higher quality of translational research. 6 Our united purpose is to “Heal, Learn and Discover,” which underpins the education, research, and treatment arms of ALERT. The treatment arm assesses and manages patients at risk of or living with lymphedema in one of three multidisciplinary clinics (diagnostic, conservative, and surgical). 6 From a research perspective, patients are invited to participate in internal or externally funded studies, including our ALERT Databank where routine clinical outcome data are collected; however, the education program invites patients to share their personal experiences with the students to enhance awareness of person-centered care.
Traditionally best-practice management for lymphedema treatment has been a “one size fits all” approach. Conservative management has included a two-phase intensive complex decongestive therapy program. 10 Phase one, or the reduction phase, includes an intensive daily treatment regime for 4 to 6 weeks involving manual lymphatic drainage (MLD) massage, compression bandages, exercise, skin care, education, and psychosocial support provided by a qualified and skilled lymphedema therapist. 11 Phase two, or the maintenance phase, involves a modified home program of phase one with use of compression garments, self-MLD, exercise, and skin care along with ongoing, lifelong self-management and monitoring of the limb to maintain decongestion and reduce risks of progression of swelling, symptoms, and infection.5,12,13 The MLD has been widely accepted as a component of conservative treatment, and a variety of MLD techniques have been taught to lymphedema therapists and their patients for more than 70 years. 14 Conventional methods of MLD aim at enhancing lymphatic drainage by shifting fluid toward adjacent functioning lymph node regions.14,15 However, despite its long history, evidence to support the use of MLD is scarce.13,15 Further, self-MLD has been reported to be the least effective therapy, 16 and patient compliance is generally poor. 17
The introduction of indocyanine green (ICG) fluorescent lymphography has significantly changed research and educational priorities as well as translated into clinical practice in guiding personalized MLD drainage techniques and sequences.18,19 ICG lymphography was initially developed to identify the sentinel nodes for breast cancer surgical intervention. 20 It was later applied to lymphedema assessment,18,21–23 in particular to locate lymphatic vessels and nodes in the microsurgical lymphatic surgeries of lympho-venous anastomosis and lymph node transfer. 24 With ICG lymphography, the superficial lymphatic architecture is observed as a dynamic map within a depth of 1 to 2 cm from the skin surface.21,25–27
ICG lymphography can be used for assessing severity of lymphedema according to the MD Anderson Cancer Center (MDACC) lymphedema staging system22,28 and for optimal therapeutic planning of personalized MLD. 18 The areas of superficial dermal backflow can aid in the understanding of the condition of the underlying lymphatic vessels. After disruption to the lymphatic system from cancer and its treatment, the body may develop compensatory adaptations to encourage lymphatic drainage from the area of obstruction. 19 We refer to this concept as compensatory drainage. ICG lymphography is considered a useful, minimally invasive, and safe tool for imaging of the superficial lymphatic system and its drainage in vivo and in real time. 18 Analysis of compensatory drainage includes visualization of where the fluid is going (drainage region) and how it gets there (drainage pattern). 18 Unlike lymphoscintigraphy, ICG lymphography does not expose the patient to radiation and has the advantage of using a faster-moving dye. 26 ICG lymphography has confirmed earlier lymphangiography findings but is capable of an immediate translation to clinical practice. 19
The primary aim of this study was to explore the compensatory drainage identified in secondary cancer-related lymphedema from those attending the ALERT diagnostic clinic using ICG lymphography and to document how these results have been translated into the ALERT education training program. The specific research questions were:
What are the common drainage patterns and regions in cancer-related lymphedema of the upper and lower limbs? Does compensatory drainage change as the MDACC's lymphedema stage increases? Which MLD techniques may be useful for drainage in upper and lower limb cancer-related lymphedema?
Methods
Design
For this cohort study, we used data collected from patients who attended our clinic at Macquarie University between February 2017 and March 2020. Data were sourced from electronic medical records, and written informed consent was obtained from all patients.
Participants
Eligibility criteria included men or women who were between 18 and 90 years of age with clinically diagnosed secondary cancer-related unilateral or bilateral lymphedema of the upper or lower limb who underwent ICG lymphography. Patients were excluded if they had primary lymphedema, secondary non cancer-related lymphedema, lipedema, or if lymphedema was not detected by ICG lymphography. Patients attended the clinic on a single occasion for a 60- to 90-minute appointment.
Anthropometric measurements
Demographic information for each patient was obtained along with information regarding cancer, adjuvant treatments, and lymphedema history. Height was measured to the nearest 0.1 cm in a standing position without shoes by using a stadiometer (SECA 213, Hamburg, Deutschland). Weight was measured by standing on electronic scales (SECA 813, Hamburg, Deutschland) without shoes and in light clothing to the nearest 0.1 kg. Body mass index was calculated from weight in kilograms divided by height in meters squared. Age was calculated from date of birth.
Limb volume and extracellular fluid measures
Limb volume was determined by one of two methods: Perometry (350NT Model, Pero-System, Wuppertal, Germany) or circumferential limb measurements taken at 4 cm intervals by using a tape measure and calculated by using the truncated cone formula. 29 Percentage volume difference was calculated by comparing the affected limb with the unaffected limb for unilateral lymphedema. Percentage volume difference was not calculated for bilateral lymphedema. Bioimpedance spectroscopy (BIS) was used to measure extracellular fluid in the affected limb as a ratio compared with the unaffected limb for unilateral lymphedema, and the ipsilateral arm/leg for bilateral lymphedema. The BIS measurements were recorded in L-Dex units (normal range is −10 to +10). 30 Two devices were used: the L-Dex® U400 (ImpediMed, Brisbane, Australia) or SOZO® (ImpediMed, Brisbane, Australia) following standard operating procedures. Both devices have been validated for use in patients with lymphedema. 1
ICG lymphography
The ALERT ICG lymphography protocol has been previously described in the upper limb 18 and breast. 31 For the upper limb, four standard injection sites were used on the affected side: at the first and fourth web spaces, and the ulnar and radial volar wrist area. 18 For the lower limb, four standard injection sites were used circumferentially around the foot. The injection sites were chosen based on previous lymphatic anatomy studies in cadavers.32,33 ICG (Verdye 25 mg; Diagnostic Green GmbH) was mixed with 5 mL of saline. Immediately after application of a cryogenic numbing device (CoolSense; CoolSense Medical Ltd.) at each injection site to reduce needle discomfit, 34 intradermal injections of 0.05–0.1 mL (0.25–0.5 mg) of ICG solution were administered.
Lymphatic scanning with the near infrared camera system (Photodynamic Eye Neo II; Hamamatsu Photonics K.K., Japan) commenced immediately after administration of the injections, and imaging data were recorded by using a digital video recorder (MDR-600HD Ikegami Tsushinki Co., Ltd.). Lymphatic imaging was continuously conducted in three phases. In phase one, any spontaneous movement of dye via the lymphatics was observed. In phase two, lymphatic scanning continued while MLD was performed by an accredited lymphedema therapist to expedite dye transit. Phase two continued until dissemination of the dye reached a plateau. Finally, imaging data were collected in phase three. The imaging data were used to provide each patient with a report outlining an individualized and personal body chart or map indicating remaining functioning lymphatic vessels, compensatory drainage patterns and regions, and the direction, speed, and pressure for MLD. This report was then discussed with the individual patient by the lymphedema therapist to assist in planning their future self-management, including recommendations for other treatments such as use of sequential intermittent pneumatic compression pump and compression garments.
Lymphatic drainage regions were determined by the location of identified lymph nodes or extension of ICG dye to the areas where lymph nodes are known to be located underneath. Where the ICG dye extended to an area where lymph nodes are not known to be located, the position was recorded and considered to drain to the deep lymphatics alongside the perforating vascular vessels. 35 The severity of lymphoedematous limbs was classified by MDACC Stage as 1: many patent lymphatic vessels with minimal patchy dermal backflow, Stage 2: moderate number of patent lymphatic vessels with segmental dermal backflow, Stage 3: a few patent lymphatic vessels with extensive dermal backflow involving the entire limb, Stage 4: no patent lymphatic vessels seen with dermal backflow involving the entire limb with extension to the dorsum of the hand or foot, and Stage 5: ICG did not move from injection sites.22,28
Results
Participant characteristics
In the data collection period, 621 patients attended the clinic for ICG lymphography, of whom 267 patients with cancer-related upper limb lymphedema (259 unilateral and 8 bilateral) and 72 patients with cancer-related lower limb lymphedema (56 unilateral and 16 bilateral) participated in the study. A total of 275 arms and 88 legs were included in the analysis (Fig. 1). The patient demographics are summarized in Table 1. Most patients with upper limb lymphedema had undergone breast cancer treatment (93.7%), with the majority undergoing an axillary lymph node dissection with adjuvant chemotherapy and radiotherapy treatments. More than 80% of patients with lower limb lymphedema were female and had undergone lymph node dissection for gynecological cancers. The mean time since lymphedema diagnosis was 4.6 years for upper limb and 8 years for those with lower limb lymphedema. The mean limb volume difference was 16.4% for the upper limb and 23.0% for the lower limb. Mean BIS L-Dex scores were observed for the upper and lower limbs at 24.3 and 27.6, respectively. Although there was a large range in volume difference and L-Dex scores, most patients presented with clinical lymphedema, as defined by these methods. 36
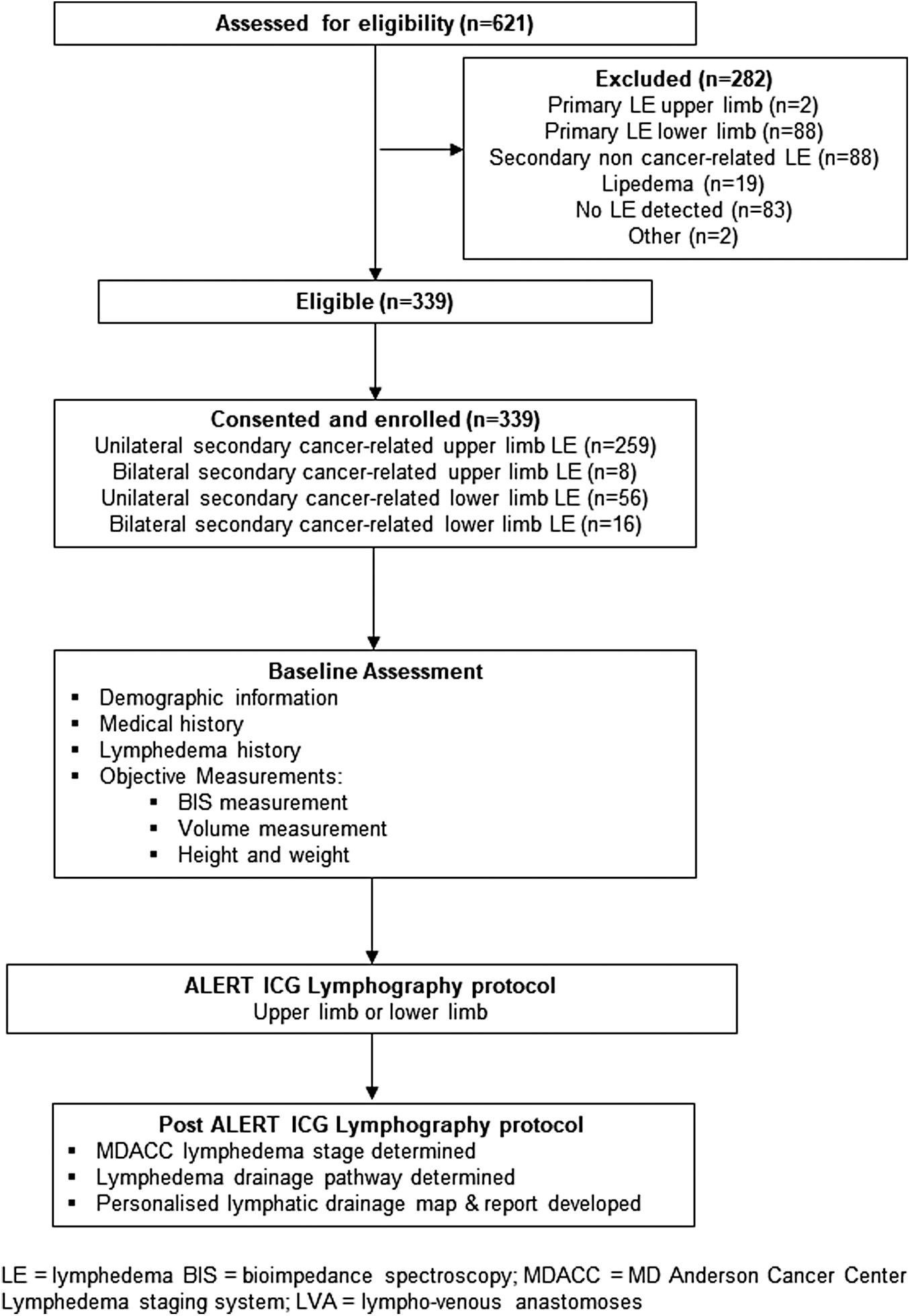
Flow of participants through the study.
Participant Characteristics
BIS, bioimpedance spectroscopy measured in L-Dex units; BMI, body mass index; LE, lymphedema; SD, standard deviation.
Compensatory patterns
The location of lymphatic vessel obstruction was frequently observed with ICG lymphography. Three compensatory patterns were identified based on which anatomical structure carried lymph fluid. First, bridging via dermal backflow extended from the obstruction site through the dermal lymphatics toward a patent lymphatic vessel, lymph node region, or an anticipated entry point to the deep lymphatics via perforating lymphatics. Second, a newly generated lymphatic vessel in the subcutaneous tissue formed a bridge between the obstructed vessel and a patent lymphatic vessel or a lymph node region (lymphangiogenesis bridging). Finally, the infrared signal initially moved in a superficial vessel but disappeared. The signal reappeared at a lymph node region, which was considered to have entered the deep lymphatics. This has been termed a localized (non-bridging) deep entry point adjacent to the area of obstruction. These patterns were sometimes combined in each case to maintain lymphatic drainage from a lymphedematous limb.
Compensatory drainage regions & MDACC staging—upper limb
The drainage regions for the upper limb are summarized in Table 2 and Figure 2. Drainage to the ipsilateral axilla was the most frequent drainage destination (74.9%), followed by clavicular (41.8%) and parasternal (11.3%). For patients with mild lymphedema (MDACC Stage 1), 94.4% drained to the ipsilateral axilla. The ipsilateral axilla was the only drainage region identified in 127 arms (46.2%). In 92 arms (33.5%), two or more combined drainage regions were evident. Overall, drainage to the contralateral axilla occurred in only 6.2% of upper limbs and was highest in patients with advanced lymphedema (MDACC Stage 4) (15.6%). For three upper limbs (1.1%), drainage regions were unable to be identified. All three upper limbs with unidentified drainage regions had a higher severity of lymphedema (MDACC Stage 4). Only one arm was classified as MDACC Stage 5. For this patient, no patent lymphatic vessels were evident; however, ICG dye appeared in the ipsilateral axilla, which was considered to have traveled via the deep lymphatics. There were no patients with upper limb lymphedema that drained to the ipsilateral inguinal region.
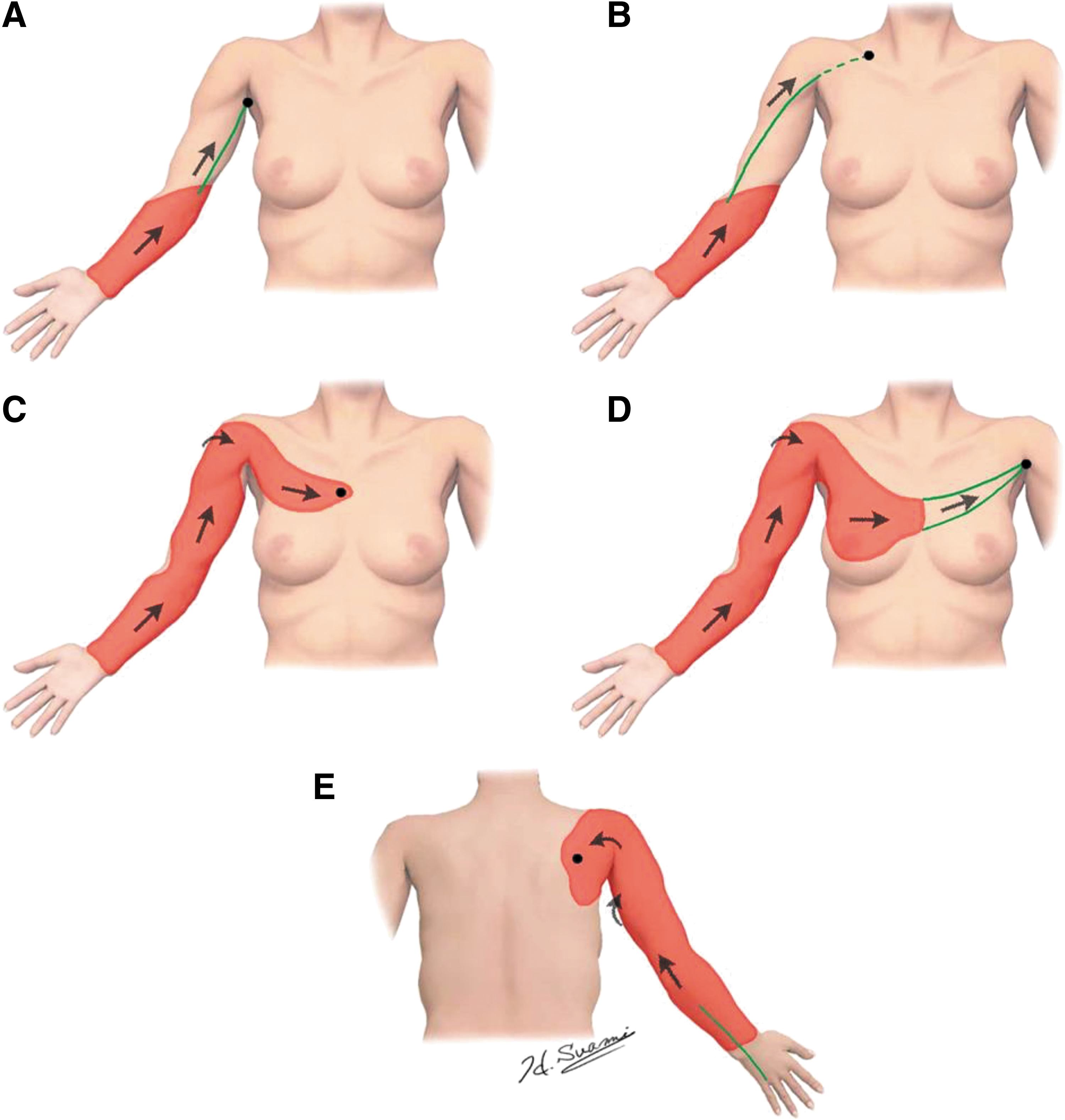
A schematic drawing of upper limb compensatory drainage regions.
Upper Limb Compensatory Drainage Regions & MD Anderson Cancer Center Staging for Secondary Cancer-Related Lymphedema
MDACC Stage, MD Anderson Cancer Center Lymphedema staging system.
Compensatory drainage regions & MDACC staging—lower limb
The drainage regions for the lower limb are summarized in Table 3 and Figure 3. Overall, drainage to the ipsilateral inguinal was most common (52.3%), followed by contralateral inguinal (30.7%), popliteal (26.1%), and gluteal (21.6%) regions. Drainage to the ipsilateral inguinal was more frequently observed with mild lymphedema (MDACC Stage 1) (88.2%) compared with MDACC Stages 3 and 4 where drainage to the ipsilateral inguinal occurred in 31.3% and 43.8% of limbs, respectively. In 22 legs (25.0%), the ipsilateral inguinal was the only drainage region identified. Two or more combined drainage regions were evident in 51 legs (58.0%). The drainage regions were unable to be identified in two legs (2.3%), both of which were classified as MDACC Stage 4. No legs were classified as MDACC Stage 5.

A schematic drawing of lower limb compensatory drainage regions.
Lower Limb Compensatory Drainage Regions & MD Anderson Cancer Center's Staging for Secondary Cancer-Related Lymphedema
MLD techniques used to facilitate compensatory drainage patterns
Dermal backflow was commonly observed at the site of obstruction. The MLD was shown to facilitate movement of the dye, and although a light/effleurage technique was sufficient to move the dye through patent lymphatic vessels, a slow and firmer technique was required to move the dye through areas of bridging dermal backflow. The therapist and patient were able to gain feedback from observing the movement of the dye on the screen in real time and to feel the level of pressure of the MLD technique required to move the dye. When MLD was applied to dermal backflow, the ICG dye appeared to extend in a specific direction rather than dispersing randomly.
Translation of results to education program
The results of the compensatory drainage patterns have been used to modify the teaching of MLD techniques to new and existing lymphedema therapists focusing on moving fluid toward the ipsilateral axilla for the upper limb and the ipsilateral inguinal region for the lower limb, especially in patients with mild lymphedema. Based on our observations during ICG lymphography, a slow and firmer pressure for MLD appears to facilitate fluid movement through areas of congestion and bridging dermal backflow. The goals would be to continue further research in this area with the aim of improving patient outcomes and reducing the time spent on unnecessary massage to pathways that are unlikely to be present.
Discussion
The introduction of ICG lymphography and its use in guiding personalized MLD has translated into clinical practice and changed research and educational priorities within the ALERT program. The aim of this study was to describe compensatory drainage in cancer-related upper and lower limb lymphedema and potential MLD techniques to facilitate utilization of these compensatory patterns as demonstrated by ICG lymphography. Where the lymphatic system is damaged or begins to dysfunction as in cancer-related lymphedema, and any of the original lymphatic collector vessels are no longer viable conduits for lymphatic fluid transport, the body makes compensatory adaptations to move fluid toward a region where it can gain access to a deeper drainage structure. 35 Our ICG lymphography observations have enabled a more thorough understanding of the movement of fluid in pathophysiological conditions, related to both the drainage pattern and the drainage region. Although individual drainage may vary, the results from the current study suggest that there are region-specific drainage trends, which may be used to infer likely compensatory drainage in individuals with cancer-related lymphedema in the absence of ICG.
For the upper limb, the most common drainage region was the ipsilateral axilla (74.9%). In 94.4% patients with mild MDACC Stage 1 upper limb lymphedema, 94.4% drained to the ipsilateral axilla despite having had an axillary lymph node dissection. The lymphatic drainage regions and their relationship to MDACC staging of upper limb lymphedema observed in this study support and strengthen previously published results.18,37 For the lower limb, the most common drainage region was the ipsilateral inguinal (52.3%). Similar to the upper limb, 88.2% of patients with MDACC Stage 1 lower limb lymphedema drained to the ipsilateral inguinal region, with the majority having had nodes dissected from this area. These data demonstrated that drainage tends to remain in the quadrant of the lymph node dissection. It is evident that as lymphedema stage worsens compensatory drainage patterns expand to other regions; however, in upper limb lymphedema, there are more options within the same quadrant (clavicular and parasternal) for drainage to occur than in the lower limb. Our results suggest that most compensatory drainage patterns shift fluid toward regions that are localized/isolated within a quadrant, but in some cases (more severe cases), fluid will superficially cross to another quadrant to find a viable drainage region.
The pattern of compensatory drainage that has been widely published as “dermal backflow” in lymphedema has been used as an imaging indicator of the disease.38,39 In the current study, we observed dermal backflow creating a bridge between obstructed and patent lymphatic vessels. Where no patent vessels were remaining, bridging dermal backflow was often recruited to move fluid from the affected area. However, as the lymphatic vessels in the dermis are microscopic in size, when dermal backflow is involved in the process of lymphatic drainage, lymph flow is restricted. 35 Historically, MLD has been applied superficially with a light effleurage pressure,40,41 as it has been suggested that MLD with firm pressure will damage the fine anchoring filaments or cause spasms in the surrounding smooth muscle sheath of the superficial lymphatic vessels. 42 In the current study, we observed the movement of lymphatic fluid in real time under ICG lymphography. Although a light effleurage is sufficient to encourage movement of the fluid through patent lymphatic vessels, when the lymphatic system is compromised and bridging dermal backflow is present, a slow and firm technique is required to achieve movement of the fluid through the dermal lymphatic vessels toward the drainage region.
There are several clinical and educational implications of this ICG lymphography research that the ALERT team are translating and integrating into their clinics and educational courses. Patients attending the ALERT clinics for ICG lymphography assessments are gaining insight into how their own lymphatic system is currently functioning and how a personalized guided MLD plan can assist in building their confidence and skill in performing their own MLD at home. Individual patients have reported substantial benefit in being able to see their lymphatics on the monitor screen and to feel the pressure and direction used by the therapist to move the fluid through their limb. Some patients have reported feeling “empowered to help themselves” with a greater understanding of the new techniques recommended from the individualized mapping of their own lymphatic system. Anecdotally, we have seen a greater adherence to self-MLD and overall conservative treatment plans for patients who have completed the ICG lymphography assessment. Our future research plans include formal assessment of adherence to conservative management and patient outcomes after ICG lymphography.
The ALERT education arm has also made significant changes to its program over recent years due to the advances from introducing ICG lymphography into the clinic as we strive to teach health professionals evidence-based care to manage those at risk of or living with lymphedema. When we are teaching compensatory drainage of the arm or leg, our main message is that generally, drainage bypasses obstructions and finds an alternative entry point to intact deep lymphatic transportation within the quadrant of dysfunction. We teach our students facilitative MLD, which uses techniques that have been observed during ICG lymphography to move fluid through the range of vessels recruited in compensatory drainage patterns. We also teach the use of sequences that encourage the movement of fluid toward evidence-based drainage regions, rather than spending time on traditional pathways. Our ALERT team has repeatedly observed in our ICG lymphography clinic that the lymphedema affected limb appears to have developed compensatory lymphatic drainage, which can be augmented but not modified by MLD. While not dismissing the notion that over time creation of new pathways are possible, we have little evidence that MLD generally results in the formation of compensatory drainage to areas outside the affected quadrant.
Despite the personalized mapping for patients being used to maximize outcomes for the individual and aid in their self-management, we are now able to use the large amount of data collected to infer likely drainage to teach health professionals in our training courses so that they can benefit from this information without necessarily having access to ICG lymphography in their own clinical setting. The ALERT education program has developed learning units that are mapped to the Australasian Lymphology Association's competencies and includes all learning needed to be accredited as a Lymphedema Therapist in Australia relative to their discipline's scope of practice. Our ICG lymphography clinical and research findings are embedded in our educational modules and will continue to be updated considering new research.
Conclusion
The ALERT's integrated and transdisciplinary approach to lymphedema has been designed to deliver holistic personalized patient care and treatment informed research to improve patient outcomes and enhance student experiences. The introduction of ICG lymphography into the program has enabled changes in clinical practice to achieve its mission of “Delivering high-standard personalized clinical care, evidence-based education and innovative research in the field of lymphedema.” As our team's knowledge and experience increases with further research in this area, it is anticipated that larger scale outcome studies can be conducted to improve the lives of those at risk of or living with lymphedema.
Ethics Committees Approval
This study was approved by Macquarie University Human Research Ethics Committee MQ Health Ethics Committee (Reference Nos. MQCIAC2018017A and 52020107614130).
Footnotes
Authors' Contributions
L.A.K.: conceptualization, project administration, resources, writing—original draft, and writing—review and editing. B.M.T.: conceptualization, formal analysis, writing—original draft, and writing—review and editing. H.M.: conceptualization, data collection, formal analysis, and writing—review and editing. R.B.: conceptualization, data collection, writing—original draft and writing—review and editing. A.H.-W.: conceptualization, data collection, and writing—review and editing. E.M.: data entry and analysis, writing—review and editing. K.G.: data analysis, writing—review and editing. J.B.: conceptualization, and writing—review and editing. H.S.: conceptualization, data collection, formal analysis, images, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.