
Abstract
Background:
Sentinel lymph node biopsy (SLNB) is the accepted approach to stage the clinically negative axilla. The incidence of lymphedema (LE) after SLNB is about 5%. We hypothesize that patients undergoing axillary excision of >5 lymph nodes (LNs) are at increased risk of developing LE.
Methods and Results:
A single institution prospective breast cancer database was retrospectively reviewed from January 2013 to December 2017, to identify patients who underwent SLNB and were diagnosed with LE. Inclusion criteria was (1) de novo breast cancer, (2) SLNB in clinically node negative patients, and (3) no preoperative diagnosis LE of an extremity. Exclusion criteria was history of axillary lymph node dissection. Age, body mass index, tumor–node–metastasis status, surgery type, neoadjuvant or adjuvant chemotherapy, radiotherapy, and hormone therapy were analyzed. Of the 3325 patients identified, 2940 patients met the inclusion criteria and were included in the final analysis. Median follow-up time was 24 months. Forty-seven (2%) patients were diagnosed with LE, and nine patients (19%) had >5 LNs excised. LE was diagnosed in 3.7% of patients who had >5 LNs excised versus 1.4% of patients with ≤5 LNs excised. Incidence of LE was higher in patients with >5 LNs excision (p = 0.006).
Conclusion:
Our study showed that patients have a higher likelihood of developing LE when >5 LNs are excised.
Introduction
Breast cancer is the most common cancer in women worldwide with 1.8 million new cases diagnosed annually. 1 Lymphedema (LE) is the most cumbersome complications of the axillary lymph node dissection (ALND) with an incidence of 25%–40%. 1 LE accumulation of proteinaceous fluid in the extracellular compartment. Localized pain, chronic edema, and decreased arm potency are clinical manifestations of LE, and can result in body dysmorphia that can substantially affect quality of life. Other symptoms include atrophic skin changes and recurrent infections.1–5
Fortunately, in past three decades sentinel lymph node biopsy (SLNB) replaced ALND in patients with clinical negative sentinel lymph nodes (LNs) and increasing evidence support doing SLNB only even in patients with low burden metastasis in their LNs.1–5 The incidence of LE is lowered from average 25% to 5% after implementing SLNB to the clinical practice. 6 In contrast, radiation therapy (RT) in the treatment of breast cancer and number of LNs excised for axillary staging can increase the incidence of this complication. 7 Herein, we reviewed our SLNB only patients' data retrospectively to evaluate if there is a subset of patients in risk for arm LE.
Methods
A single-institution prospective breast cancer database was retrospectively reviewed from January 2013 to December 2017, to identify patients who underwent SLNB and were diagnosed with LE. LE was diagnosed at LE Clinic in Breast Surgery Unit of Magee-Womens Hospital. Inclusion criteria was (1) de novo breast cancer, (2) SLNB in clinically node negative patients, and (3) no preoperative diagnosis LE of an extremity. Exclusion criteria was history of ALND. Age, body mass index (BMI), tumor–node–metastasis status, surgery type, levels, neoadjuvant or adjuvant chemotherapy, RT, and hormone therapy were analyzed. Dual technetium (Tc-99) and blue dye tracers identification used for SLNB. LE was diagnosed by physical examination, indocyanine green lymphography (ICG-L), lymphoscintigraphy (LSG), and L-dex score. Patients were diagnosed based on LE stage, as defined by the International Society of Lymphology (Table 1). Stages are defined by presence of lymphatic channels, and degree of fibrosis leading to irreversible edema the affected extremity. Demographics, type of surgery, locoregional RT, and clinicopathologic features were evaluated (Table 2).
Staging System of Lymphedema Adapted from the International Society of Lymphology
Patients With and Without Lymphedema
Bold/italics values shows significant.
Others: segmental mastectomy and lumpectomy with or without re-excision.
BMI, body mass index; LE, lymphedema; SD, standard deviation.
Continuous and categorical variable differences between the two groups were analyzed using the t-tests and chi-square tests, respectively. p-Values <0.05 were considered as statistically significant. All analyses were conducted with R program version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria, https://www.r-project.org). Institutional Review Board approval was taken.
Results
Of the 3325 patients identified, 2940 patients met the inclusion criteria and were included in the final analysis. Mean age was 59 ± 12 and mean BMI was 28.9 kg/m2. Mean number of resected LNs during SLNB was 3 ± 1.64. Median follow-up time was 24 months. Forty-seven (2%) patients were diagnosed with LE, and nine patients (19%) had >5 LNs excised.
When the number of regional nodes compared between the LE+ and LE− groups as a continuous variable, there was no statistically significant difference between their means. Because the median number of nodes was three and standard deviation was two for both groups, follow-up analyses compared number of patients below and above median (three) number of nodes, and more than a standard deviation more or less number of nodes (five) between the LE+ and LE− groups.
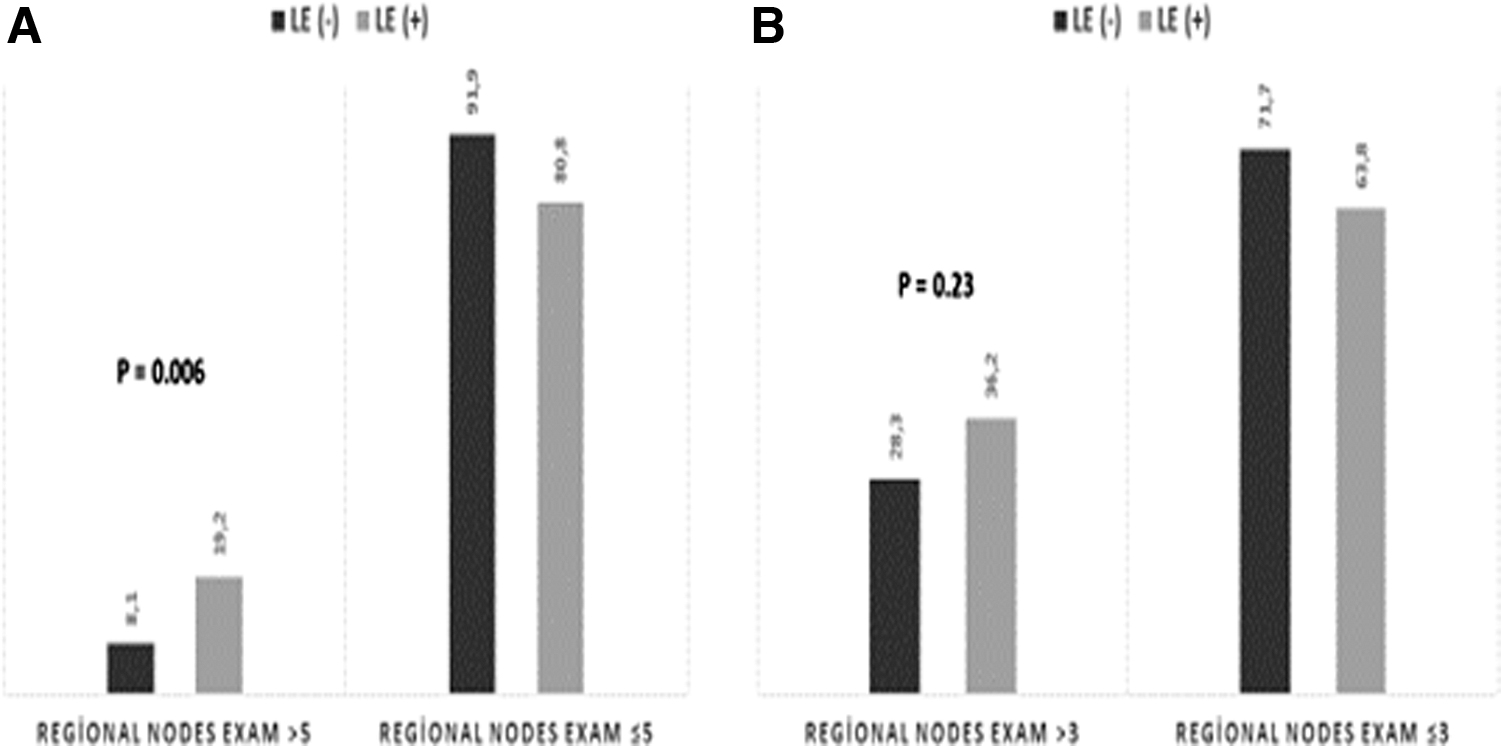
LE was diagnosed in 3.7% of patients who had >5 LNs excised versus 1.4% of patients with ≤5 LNs excised. Incidence of LE was higher in patients with >5 LNs removed (p = 0.006) (Fig. 1A). Positive LN number was not correlated with incidence of LE (p = 0.17). Of the 2893 patients who were not diagnosed with LE, mean BMI was 28.9 kg/m2 and of the 47 LE patients mean BMI was 30.0 kg/m2 (p = 0.31). Surgical procedure and locoregional RT rates were similar in the two groups. Mean age was similar: 59.9 years in the no-LE versus 59.1 years in the LE (p = 0.66). More than 5 LNs removed had almost three times higher risk of having LE at 2 years. LE was 2% in >3 LNs dissected versus 1.4% in <3 LNs dissected. More than 3 LN dissection was not correlated with LE (p = 0.23; Fig. 1B).
There was no statically significant difference between >5 LNs excised versus ≤5 LNs in patients diagnosed with LE who received RT (p = 0.41; Table 3).
Locoregional Radiation in the Lymphedema Group
Discussion
LE is a major morbidity of axillary surgery and a well-known complication of ALND. LE is the most cumbersome complication of the ALND with an incidence of 25%–40%. 1 Although incidence of LE is much lower with SLNB, there is a subset of patients undergoing SLNB that are more prone to developing this complication.8,9 Obesity is a known risk factor for the development of LE after axillary surgery.8,9 The hypothesis of the cause of obesity is that lymphatic channels can be occluded by excess fat deposits. Adding RT to the chest wall and axilla increases the development of LE. 8 In The American College of Surgeons Oncology Group (ACOSOG) Z0011 study whether the 10-year overall survival of patients with sentinel LN metastases treated with breast-conserving therapy and SLND alone without ALND is noninferior to that of women treated with ALND was determined. Among 891 women who were randomized 856 (96%) completed the trial. The 10-year overall survival and disease-free survival were similar in SLND alone and in ALND groups (p > 0.05). Between years 5 and 10, one regional recurrence was seen in the SLND alone group versus none in the ALND group. 10 In this study of 668 breast cancer patients prospectively screened for LE and the incidence of LE by arm measurements at 12 months were 6% (14/226) in the SLND group and it was 11% (26/242) in the ALND group (odds ratio = 05.2, 95% confidence interval 0.260–1.057, p = 0.0710). 11 In ACOSOG Z0011 study clinical LE incidence in 1 year was higher than our study; this may be attributed the number of excised SLNs in the ACOSOG Z0011 (LN excised range 0–33) and the high tangent RT. In our study, more patients who received RT developed LE in our cohort (76% vs. 67% p = 0.21), although this was not statistically significant average.
We found that BMI was not a risk factor for LE; however, there was a slight increase in the number of patients who developed LE in the BMI >25 cohort (66%, p = 0.72).
At After Mapping of the Axilla: Radiotherapy or Surgery trial, the 1-, 3-, and 5-year LE was evaluated. Signs of LE were noted at 5 years in 23% of the patients after ALND and 11% of those after axillary RT. In axillary RT group 43% of cases has 1, 32% has 2, 15% has 3, and 10% has ≥4 SLNs removed. In subgroup analysis both RT and surgery to the axilla caused more LE incidence compared with patients who were treated with ALND or axillary RT only. 12 The incidence of LE by arm measurements at 12 months were 28% (114/410) in the ALND group and it was 15% (62/410) in the axillary RT group (p ≤ 0.0001). 12 In our analysis, there is no difference for LE occurrence considering RT [LE (−): 66.2% vs. LE (+): 74.5%; p = 0.21].
Although LE is diagnosed with volume measurements or with patients subjective reporting in the clinical trials, imaging studies such as LSG is currently the standard imaging test to confirm the diagnosis. 13 Kayiran et al. provided an algorithm to diagnosing LE. 14 The authors stated that the use of ICG-L and Bioelectrical Impedance Spectroscopy (BIS) measurements are provided a more accurate diagnosis and guided therapeutic interventions better. In our series the diagnosis rate with these modalities was >95%.
Incidence of LE was higher in patients with >5 LNs dissected. This threshold calculated by statistical analysis. In a study of 587 patients undergoing mastectomy and conservative axillary regional excision (CARE), Cowher et al. showed that the development of LE was associated with the number of LNs dissected (p = 0.05) and RT (p = 0.04). 1 CARE consisted of the removal of SLNs and palpable nodes only, whereas omitting intraoperative frozen section and reoperation for node positive patients. Twenty patients developed LE, and the authors concluded that excising ≥5 LNs could lead to an increased risk of developing LE. LN positive patients (N1) undergoing CARE had a locoregional recurrence rate of 3.4%, and three patients had recurrences in the axilla for a mean follow-up of 5.4 years. The threshold number of excised LNs causing LE was 5, which was the same in Kilbreath et al. studies. 7
Goldberg et al. 2 studied the rate of perceived LE in 600 women who underwent SLNB for breast cancer. Patients upper extremity circumference was measured pre- and postoperatively. Perceived LE was evaluated with a surgical follow-up interview. At a median 5-year follow-up, 3% of patients reported perceived LE. The authors noted that there was poor concordance between patient perceptions and objective measures of LE. However, they did find that patients with numbness were more likely to report perceived LE, and that those patients underwent a more extensive axillary LN excision during SLNB (p = 0.02). 2 To eliminate mis-LE diagnosis based on subjective symptoms we evaluated all patient with tape measurements and additionally one of the objective diagnostic tools where appropriate such as ICG-L, LSG, and BIS in our study.
Even though, in our study, the LE incidence is low in SLNB patients (1.6%) removing >5 LNs more than doubles the risk of LE [LE was 3.7% in >5 LNs dissected vs. 1.4% in ≤5 LNs dissected (0.006) at 2 years]. The majority of our patients had breast conserving surgery and whole breast RT in both groups and average BMI were similar in LE and non-LE patients.
There are several limitations in our study. First, there may be a correlation between postoperative infection and the development of LE, which was not explored in this study. Second, longer follow-up is needed to evaluate this cohort over time. In addition, the LE diagnosis is from the e-record review so there may be some patients that were not evaluated for LE.
Conclusion
Our study provides evidence that the number of SLNs dissected does predispose patients to developing LE. Notwithstanding, a longer follow-up is needed, we have expanded close follow-up for early diagnosis of LE in patients with >5 LNs dissected in our clinical practice. To diagnose LE earlier (preclinical; Stage 0) than clinical stage we also include >5 LNs removal is an indication for BIS and ICG.
Footnotes
Authors' Contributions
Data collection by A.I., A.S., A.G., and N.B. Statistical analysis by E.S. Writing of the article by A.I., A.S., A.G., N.B., and E.S.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.