
Abstract
Background:
The aim of this study was to compare the effects of complex decongestive therapy (CDT) accompanied by resistance exercises on extremity circumference, lymphedema volume, grip strength, functional status, and quality of life in the treatment of breast cancer-related lymphedema (BCRL) in patients with and without pain.
Methods and Results:
Fifty patients with unilateral BCRL were divided into groups: with pain (Group 1, n = 25) and without pain (Group 2, n = 25). Thirty minutes of manual lymphatic drainage and multilayered short-stretch bandaging were applied to all patients five times a week for 4 weeks. In addition, all patients were informed about skin care and given a supervised resistance exercise program throughout the treatment. During the 1-month follow-up period, patients were asked to use low-tension elastic garments and to continue their home exercise program. Differences in upper extremity circumference and volume; grip strength; Quick Disabilities of the Arm, Shoulder, and Hand; and Functional Assessment of Cancer Therapy-Breast scores were evaluated at baseline, after treatment (week 4), and at 1-month follow-up. Moreover, the pain intensity of patients in Group 1 was measured using the visual analog scale (VAS). Patients in both Group 1 and Group 2 showed a statistical improvement in all outcome measures after treatment and at follow-up (p < 0.05); however, no significant difference was observed between the groups (p > 0.05). In Group 1, a statistically significant decrease was observed in the VAS score both at the end of treatment (−1.7 ± 0.9) and at 1-month follow-up (−3.5 ± 1.2) (p < 0.05).
Conclusion:
Combined CDT and resistance exercises appear to be effective in BCRL patients both with and without pain.
Introduction
Lymphedema is a condition characterized by chronic abnormal swelling in the torso and/or extremities caused by accumulation of protein-rich fluids in the interstitial area due to an imbalance between lymphatic drainage and capillary filtration. 1 Upper extremity lymphedema, which occurs most frequently in patients undergoing surgery and/or radiation therapy due to breast cancer, is one of the most challenging sequelae of breast cancer treatment. The pooled incidence of breast cancer-related lymphedema (BCRL) is estimated to be 16.6%. 2 Several risk factors exist for development of lymphedema, including extensive invasive surgery, adjuvant therapy (radiation and chemotherapy), high body–mass index (BMI), low physical activity, and genetic factors associated with lymphatic and angiogenic genes.3,4
In addition to swelling in the affected extremity due to lymphedema, secondary problems such as pain, weight, tension, and decreased range of motion (ROM) affect patients' work and social life through daily activities and psychological conditions, thus negatively affecting their quality of life.5,6 Persistent pain after breast cancer treatment can affect 20%–50% of patients, depending on the treatment.7,8 Pain has been reported to be the greatest problem associated with lymphedema after breast cancer and it has been observed to be the most adverse factor affecting the function and quality of life of patients with lymphedema.9,10
The main goal is to prevent lymphedema and related factors in patients undergoing breast cancer surgery. Conservative interventions (education, self-manual lymphatic drainage [MLD], and exercise) for the prevention of BCRL appear to be more beneficial when started early. 11 Early diagnosis and treatment of lymphedema have been shown to increase treatment efficacy and decrease disease progression. 12 Complex decongestive therapy (CDT), which has been proven as an effective treatment method in patients diagnosed with BCRL in systematic reviews and meta-analyses and which is accepted as the current standard treatment approach by the International Society of Lymphology (ISL), is a two-stage treatment program comprising Phase I, which includes skin care, MLD, compression therapy with multilayered bandaging, and therapeutic exercises, and Phase II, which includes the use of compression garments.1,13–15 Recently, upper body resistance exercises have been shown to be a potential effective management strategy for BCRL patients, especially due to their potential to improve muscle function and increase lymphatic drainage by providing muscle contraction and pumping.16,17
Although the efficacy of CDT in BCRL has been proven in literature, the patient response to treatment varies widely. Therefore, our study aims to investigate the efficacy of combined supervised resistance exercises and CDT in BCRL and whether the presence of pain has an effect as a negative potential factor that may affect treatment response.
Materials and Methods
A total of 50 patients who were diagnosed with unilateral upper extremity lymphedema after breast cancer surgery in the physical medicine and rehabilitation outpatient clinic between May 2016 and May 2019 were included in the study, which had a 1-month follow-up period. The patients were divided into two groups: with extremity pain (Group 1, n = 25) and without pain (Group 2, n = 25). Evaluations of outcome measures were performed at baseline, after 4 weeks of treatment, and at 1-month follow-up. All evaluations were performed by the same physician. The patients received oral and written information regarding the purpose, duration, and application methods of the study, and the Informed Consent Form was signed after their consent was obtained. The Ethics Committee of the University of Health Science Kanuni Sultan Suleyman Research and Training Hospital approved the study protocol in accordance with the Helsinki Protocol (IRB study protocol: 2020.08.182).
The inclusion criteria were being above 18 years of age, stage 1 or 2 unilateral lymphedema based on ISL after breast cancer surgery, and >2 cm difference in circumference between extremities and/or >10% difference in volume. 18 Exclusion criteria in the study were the presence of primary lymphedema or bilateral upper extremity lymphedema; stage 3 lymphedema based on ISL; presence of active cancer; skin infection or radiotherapy burn in the affected extremity; rheumatic diseases, such as systemic lupus erythematosus, renal failure, and advanced heart failure; and a history of untreated deep vein thrombosis. In addition, patients who received CDT or other lymphedema treatments within 12 months were also excluded.
Standard CDT treatment was administered to all patients for 4 weeks, 5 days a week (Monday–Friday), by an experienced physiotherapist. Thirty minutes of MLD was applied from the affected extremity toward the unaffected side (anterior trunk, posterior trunk, and affected extremity) before bandaging as per the same standardized protocol. Multilayered short-stretch bandages were used for compression. All patients were asked to keep the multilayered bandaging on the arm for at least 22–23 hours a day. In the maintenance phase, low-tension elastic garments were used instead of bandaging. Patients were also trained in proper skin care, such as avoiding excessive heat and trauma and applying moisturizer daily. They were also warned about not gaining weight, drinking plenty of fluids, and eating a salt-free diet.
Furthermore, a supervised exercise program was applied for all patients by the physiotherapist after the CDT treatment session for 4 weeks, 5 days a week. During exercise sessions, patients were instructed on the correct techniques of exercises. Patients continued to wear the multilayered bandages during the exercises, depending on their personal preferences. The exercise volume was adjusted and individualized based on the capacities of patients. The 45–60 minutes of supervised exercise program included warm-up and cooldown exercises (walking or stationary cycling), active shoulder ROM, stretching exercises for the upper extremity muscles (trapezius, levator scapulae, and pectoralis), and a resistance training program targeting upper extremity muscle groups. Resistance exercises (chest press, bent-over row, bicep curl, triceps extension, lateral raise, and wrist curl) were performed using free weight dumbbells (0.5 or 1 kg).19,20 Each exercise, comprising 3 sets of 10–12 repetitions, was performed with a 2-minute rest period between sets and exercises. The weights for lifting during each set were adjusted so that the last repetition in each set could be completed with a successful lift using maximum effort. In addition, all patients were trained to perform home exercises until the follow-up after 4 weeks of treatment, and the patients were called once a week during the follow-up period. Details about the exercise program are presented in Table 1.
Exercise Program
ROM, range of motion.
All patients in both groups were required to attend at least 16 (80%) of the 20 treatment sessions for final analysis. Furthermore, the patients kept an exercise diary to monitor their compliance with the exercise program throughout the follow-up period.
Outcomes
Extremity circumference measurements were performed at 4-cm intervals starting from the wrist with the patient in an upright sitting position on the chair, while the shoulder was in 90° abduction. 21 The 9-mm-wide, flexible, and nonelastic tape measure used in circumference measurements had a precision of 0.1 cm. Measurements were performed separately for both upper extremities, and the difference was recorded in centimeters. The extremity volume values were found by calculating the circumference measurement values using the Frustum formula (truncated cone formula). 22 The difference in volume values between the two extremities was recorded in milliliters.
Self-assessment of pain intensity during rest and activity of the patients in Group 1 during the previous week was measured using a 10-cm visual analog scale (VAS): 0 at the left end of the line represented no pain and 10 at the right end represented worst pain imaginable. 19
Grip strength was assessed by measuring the lymphedematous extremity in kilograms using a Jamar hydraulic hand dynamometer (Sammons Preston Rolyan, Bolingbrook, IL). 23 After a trial measurement without using maximum force, patients were asked to perform three consecutive measurements with maximum force at 30-second intervals in the standard position (shoulder adduction, forearm neutral position, elbow 90° flexion, wrist 0°–30° extension, and 0°–15° ulnar deviation). The arithmetic mean of the three values was calculated.
An 11-question Quick Disabilities of the Arm, Shoulder, and Hand (Q-DASH) questionnaire, which evaluated physical function and symptoms and was answered by the patient, was used to determine the upper extremity functional level. 24 A 5-item scale (1 representing no difficulty and 5 representing the highest difficulty) was used for each question. The total Q-DASH score was calculated, where 0 represented no disability and 100 represented the most severe level of disability.
Functional Assessment of Cancer Therapy-Breast (FACT-B) was used in the quality-of-life assessment; it was assessed by the participants themselves. 25 FACT-B comprises five subgroups (Physical well-being [7 items], Social/Family well-being [7 items], Emotional well-being [6 items], Functional well-being [7 items], and Additional concerns [10 items]), and each question comprises 5 options (0: not at all, 1: very little, 2: a little, 3: quite, and 4: a lot). Higher scores of FACT-B indicate a better quality of life.
Statistical analysis
SPSS software (Version 22.0; IBM Corp., Armonk, NY) was used for analysis. Descriptive statistics of the data are expressed as mean values and standard deviations for continuous variables and as counts and percentages for categorical variables. Mann–Whitney U and chi-squared tests were used to analyze qualitative independent data. The Shapiro–Wilk test was used to analyze the normal distribution of quantitative variables. In all data, the Friedman test was used to compare outcome measures between the groups at three time points (baseline, posttreatment, and 1-month follow-up). The Wilcoxon signed-rank test was performed to evaluate intragroup changes. Moreover, the Mann–Whitney U test was used to compare group differences at each time point. The significance level in the study was determined as p < 0.05.
Results
Participant characteristics
The demographic and clinical characteristics of patients are summarized in Table 2. The sample size was 45 patients (Group 1 with pain, n = 22; Group 2 without pain, n = 23). Five patients were excluded from the final analysis due to insufficient level of participation and loss to follow-up (Fig. 1). In terms of demographic and clinical characteristics of patients and all evaluation criteria, no significant difference was observed between the two groups at the baseline evaluation (p > 0.05).
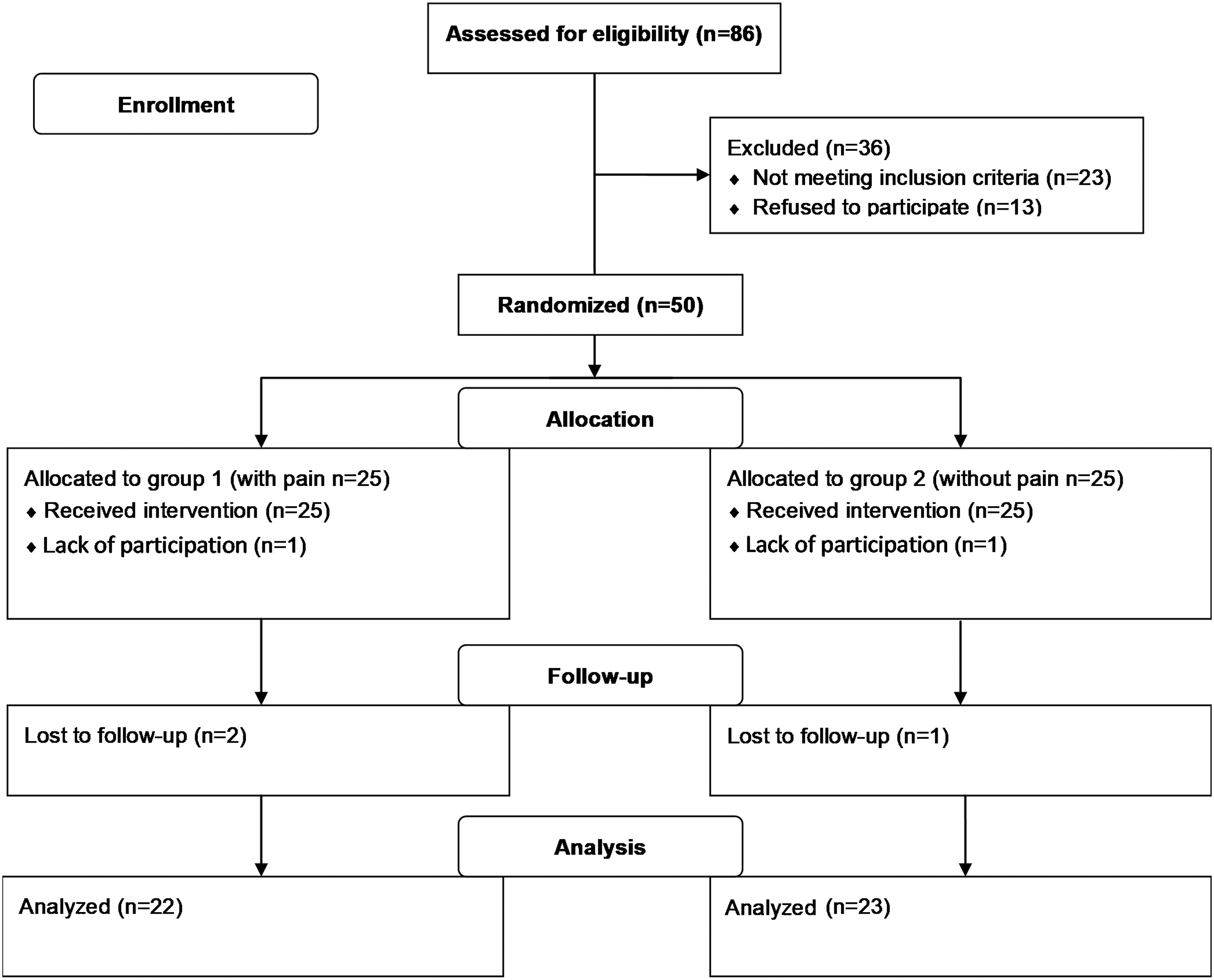
Flow diagram of patients in the study.
Baseline Demographic and Clinical Characteristics of the Patients
Means (SDs) are given for continuous variables; n (%) is given for categorical data.
p-Values for continuous variables were calculated using the Mann–Whitney U test; p-values for categorical data were calculated using the chi-squared test.
BMI, body–mass index; CDT, complex decongestive therapy; PC, pneumatic compression; PG, pressure garment; SD, standard deviation.
Outcomes
Extremity circumference difference showed a statistically significant decrease in both Group 1 and Group 2 at the end of treatment (−3.2 ± 2.3, p < 0.001, and −4.2 ± 2.8, p = 0.011, respectively) and at 1-month follow-up (−2.1 ± 3.7, p = 0.003, and −3.6 ± 3.2, p < 0.001, respectively). However, in the group comparison, no statistically significant difference was observed after treatment (p = 0.219) and at follow-up (p = 0.733) (Table 3). Patients in Group 1 and Group 2 had a statistically significant decrease in lymphedema volume difference at the end of treatment (−80.0 ± 56.1, p < 0.001, and −110.1 ± 63.3, p = 0.001, respectively) and at 1-month follow-up (−55.6 ± 100.7, p = 0.003, and −90.8 ± 79.3, p = 0.001, respectively). No significant difference was observed in the comparison between Group 1 and Group 2 (p = 0.173 and p = 0.413, respectively) (Table 3).
Descriptive Data and Comparisons Within and Between Groups for Each Outcome Measure
p-Values for within-group comparisons were calculated using the Wilcoxon signed-rank test; p-values for between-group comparisons were calculated using the Mann–Whitney U test.
FACT-B, Functional Assessment of Cancer Therapy-Breast; Q-DASH, Quick Disabilities of the Arm, Shoulder, and Hand.
In Group 1, pain intensity was 4.8 ± 1.7 at the beginning, 3.9 ± 1.7 at the end of the treatment, and 1.3 ± 1.1 at the 1-month follow-up. A statistically significant decrease was observed in the VAS score both at the end of treatment (−1.7 ± 0.9, p < 0.001) and at 1-month follow-up (−3.5 ± 1.2; p < 0.001) (Fig. 2).
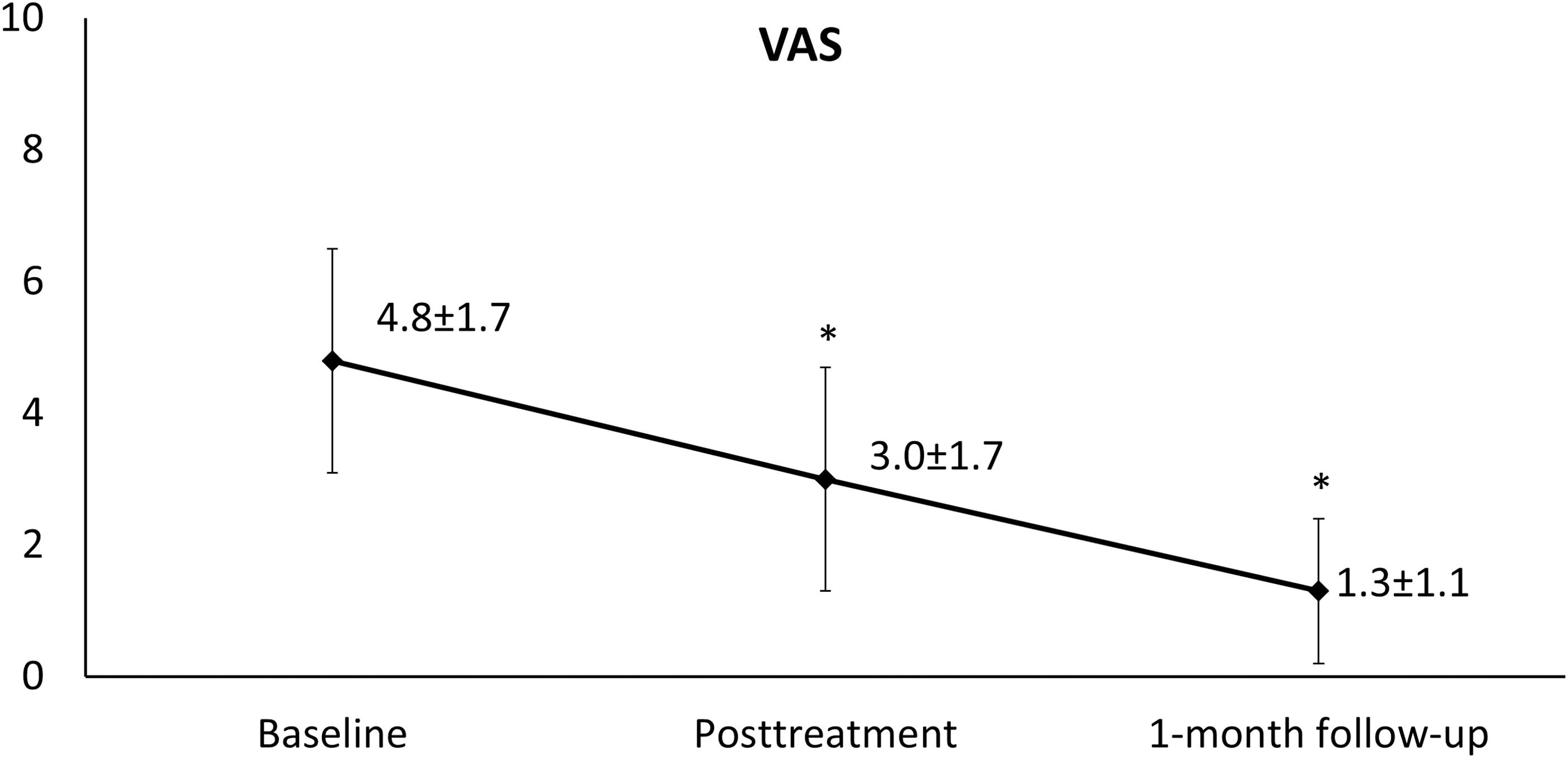
Changes in mean values with standard deviations for VAS scores in Group 1. *p < 0.05. VAS, visual analog scale.
Grip strength was significantly higher both at the end of treatment (0.6 ± 0.8, p = 0.005, and 0.6 ± 1.2, p = 0.041, respectively) and 1-month follow-up (0.5 ± 0.7, p = 0.012, and 1.0 ± 1.4, p = 0.005, respectively) in Group 1 and Group 2. In the comparison of groups, no significant difference was observed in grip strength between the groups both after the treatment (p = 0.808) and at 1-month follow-up (p = 0.491) (Table 3).
Q-DASH scores statistically significantly decreased in Group 1 both at the end of treatment (−4.5 ± 4.2, p < 0.001) and at 1-month follow-up (−6.2 ± 6.3, p < 0.001) and also in Group 2 at the end of treatment (−3.3 ± 5.4, p = 0.004) and at 1-month follow-up (−2.5 ± 9.7, p = 0.040). However, in the comparison between groups, no significant difference was observed at the end of treatment and follow-up compared with the baseline (p = 0.776 and p = 0.467, respectively) (Table 3).
When the FACT-B scores were evaluated within the group, a statistically significant increase was observed in Group 1 and Group 2 after the treatment (6.2 ± 8.1, p = 0.005, and 3.9 ± 6.0, p = 0.004, respectively) and at 1-month follow-up (2.3 ± 3.5, p < 0.001, and 2.9 ± 4.7, p = 0.004, respectively); however, when the groups were compared, no significant difference was found compared with the baseline at the end of treatment and at follow-up (p = 0.882 and p = 0.500, respectively) (Table 3).
Discussion
This study investigated the effectiveness of combined resistance exercises and CDT in BCRL treatment and the effect of pain on treatment results. To the best of our knowledge, our study is the only clinical study in the literature testing the effectiveness of combined resistance exercises and CDT in BCRL patients with and without upper extremity pain. Based on the results of our study, it was observed that the resistance exercises and CDT method used in BCRL management had statistically positive effects on volume, circumference measurements, grip strength, functional status, and quality of life in patients both with and without pain, while no statistical difference was observed in any outcome measures between the groups.
Consistent with our results, literature suggests that the multicomponent therapy, called CDT, is effective in reducing volume and circumference measurements in BCRL.1,13 In our study, mean percentage change in lymphedema volume was 29.2% and 20.1%, respectively, in Group 1 and Group 2 at the end of the intensive phase and 37.2% and 30.7%, respectively, during follow-up; mean decrease in lymphedema volume after CDT varies between 20% and 73% in literature. 13 Factors such as the length of lymphedema duration, presence of advanced lymphedema, and obesity have been shown to negatively affect CDT in reducing lymphedema volume.10,26,27 However, to the best of our knowledge, the risk of pain on treatment has not been assessed in previous studies that have investigated predictive factors for the effectiveness of CDT.
Leysen et al. 28 examined pain risk factors in breast cancer survivors in their systematic review and meta-analysis. They showed that BMI >30, education <12–13 years, presence of lymphedema, smoking, axillary lymph node dissection, chemotherapy, and radiotherapy were significantly associated with development of pain and that lymphedema was the strongest risk factor. In addition, lymphedema may cause pain in the upper extremity as well as decreased ROM, stiffness, weakness, numbness, and dysfunction. 29 Lymphedema and these conditions of the upper extremity have been shown to lead to limitation in activity.30,31 Moreover, as is well known, pain in BCRL has a negative impact on both physical and mental quality of life.8,32 Dawes et al. 9 suggested that pain, rather than lymphedema, was the only condition that was directly related to upper extremity activity limitation in BCRL.
The primary goal of lymphedema treatments is to reduce extremity swelling and thus improve physical function and quality of life. However, the effectiveness of CDT on symptoms associated with lymphedema, upper extremity function, and quality of life is controversial. Mobarakeh et al. 33 and Hamner et al. 34 examined the effects of CDT in BCRL patients in their studies and found that it effectively reduces pain as well as the volume of lymphedema. In contrast, some other studies show that CDT used for management of BCRL leads to a significant relief regarding lymphedema volume; however, it may not help improve the subjective symptoms and arm function and quality of life associated with lymphedema.35,36 In their study, Dawes et al. 9 examined the effect of lymphedema on arm function and health-related quality of life in women after breast cancer surgery and reported that treatments only reduced lymphedema volume without pain reduction, which was unable to improve upper extremity functions or quality of life. However, in our study, a statistically significant decrease in extremity circumference and volume, as well as a statistically significant improvement in grip strength, DASH, and FACT-B scores, was observed in BCRL patients in Group 1. In our study, the reason for the improvement in upper extremity functions or quality of life was the 1.3-point minimal clinically important difference in VAS score for pain intensity in Group 1 37 (a decrease of −1.7 points after treatment and −3.5 points at follow-up).
Some studies using the combination of CDT and exercise report a significant reduction in both pain intensity and lymphedema volume and extremity circumference as well as an increase in function and quality of life.38,39 Melam et al. 39 compared the CDT group (MLD, compression garment, shoulder girdle mobilization, and pectoralis and trapezius muscle stretching) and conventional therapy group (MLD, compression garment, shoulder ROM, and deep breathing exercises) in their study on 60 BCRL patients (including five sessions of treatment per week for a total of 6 weeks); they achieved more pain reduction and improvement in quality of life in the supervised exercise CDT group. Similarly, the significant change in pain reduction in our study may be associated with the fact that it included individualized progressive resistance exercises that were applied together with standard CDT. In the randomized controlled study by Park, 36 69 patients diagnosed with BCRL were given standard CDT (pneumatic compression, MLD, and bandaging) or supervised complex exercises (aerobic exercise and strength training) five times a week for a total of 4 weeks, and they found that complex exercises significantly decreased VAS scores compared with CDT at the end of 4 weeks. This significant difference has shown that supervised exercises have become an integral part of lymphedema treatment for pain management in BCRL patients. In addition, although there was some worsening in extremity circumference and lymphedema volume during follow-up, pain reduction continued in our study. This showed that pain reduction in BCRL was independent of lymphedema volume reduction and that the effects of supervised resistance exercises on pain continued in the short term.
As BCRL patients often have a significant fear of resistance exercise and exercise programs in CDT mostly include aerobic and stretching exercises, the affected extremity muscle mass decreases, which affects quality of life and functions.40,41 Studies have shown that different types of physical exercises, such as aerobic, relaxation, and aqua training, and resistance exercises do not cause or exacerbate lymphedema and therefore it has been emphasized that they can be safely performed by breast cancer patients.42–44 Moreover, Sim et al. 45 reported that active resistance exercise did not cause additional swelling and that it decreased extremity lymphedema volume and significantly increased quality of life. Bok et al. 46 investigated the effectiveness of CDT and progressive resistive exercises in BCRL patients, five times a week for a total of 8 weeks, and the effectiveness of only CDT. Since their study used ultrasound measurements, Bok et al. 46 observed a significant reduction in the subcutaneous tissue in the affected arm, a significant increase in muscle thickness, and a marked decrease in upper extremity circumference in the CDT and progressive resistive exercise group. In addition, they found different rates of muscle growth between the affected and unaffected arms, contrary to previous assumptions. Thus, we can conclude that this is due to the increased movement in the affected arm muscles in response to the resistance exercise stimulus. Therefore, upper body resistance exercises stand out as an important part of the treatment for BCRL patients as they show the potential to increase functional capacity as well as increase lymphatic drainage with muscle contraction.
Strengths and limitations of the study
This study is important in terms of demonstrating the effectiveness of CDT and supervised resistance exercises in management of pain with concurrent lymphedema treatment. In addition to measuring lymphedema volume, the evaluation of grip strength, upper extremity function, and quality of life is one of the strengths of our study. Another strength of our study is that resistance exercises were performed under the supervision of a physiotherapist and were individualized.
The first limitation of the study is the relatively small sample size. The second limitation is that long-term effects of the treatment could not be observed due to the short follow-up period in our study. The third limitation is that the results of the study cannot be generalized to severe lymphedema (stage 3) as the patients enrolled in the study had stage 1 or 2 lymphedema. Another limitation is that the measurement of extremity volume was performed by indirect calculation using circumference measurement. Finally, increased patient activity levels during treatment and follow-up could have affected the results, but this was not investigated herein.
Conclusion
The results of our study showed that the CDT combined with resistance exercises applied five times a week for a total of 4 weeks in BCRL treatment was effective in reducing extremity circumference and lymphedema volume; improving grip strength, function, and quality of life; and reducing upper extremity pain at the end of the treatment and during the 1-month follow-up period. In addition, pain reduction continued despite the increase in lymphedema volume during follow-up in our study, which indicates that resistance exercises can be used as a potential additional therapy to CDT. However, the optimal treatment protocol (number and frequency of sessions) for resistance exercises and the muscle groups for these exercises should be evaluated in the treatment of BCRL and associated symptoms in a larger number of patients in future controlled studies with longer follow-up.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest with respect to the authorship and/or publication of this article. No competing financial interests exist.
Funding Information
The authors didn't receive any financial support for the research and/authorship of this article.