
Abstract
Background:
Debulking via power-assisted liposuction has been established internationally as the gold standard for patients with chronic fat-dominant lymphedema. In this study we share our experience implementing a debulking surgery program in the United States.
Methods and Results:
A retrospective review was performed of patients who underwent debulking surgery using power-assisted liposuction at a single institution. Between December 2017 and January 2020, 39 patients with lymphedema underwent 41 extremity debulking procedures. In patients with lymphedema of the upper extremity, median excess volume reduction was 111% at 6 months and 116% at 12 months post-operatively. In patients with lymphedema of the lower extremity, excess volume reduction was 82% at 6 months and 115% at 12 months post-operatively. L-Dex and quality of life improved across all domains in upper and lower extremity patients as well.
Conclusion:
Debulking with power-assisted liposuction is an effective treatment for chronic lymphedema, supported by improvement in both objective and subjective metrics.
A

Fat- and fluid-dominant soft tissue swelling in cases of lower extremity lymphedema.
The surgical approach to perform extremity debulking at our institution was adapted from the technique developed by Håkan Brorson.3,4 The limb is debulked using power-assisted liposuction (MicroAire Surgical Instruments, VA) with custom-made 3- and 4-mm cannulas (MD Resource, CA) under tourniquet control. Custom garments are placed on the patient's extremity after the liposuction is completed up to the distal edge of the tourniquet. The tourniquet is then released and the proximal limb is tumesced with 1 or 2 L of tumescent solution for the upper and lower extremity, respectively, and liposuction of the proximal limb is performed. Upon completion, the custom garment is fully unrolled to cover the proximal limb. The intraoperative debulking aspirate collected while under tourniquet control is stored in a separate container from that collected after tourniquet release to allow for more accurate fat volume estimation.
After surgery, patients must remain in custom compression 24 hours per day. For patients with lower extremity lymphedema, waist-high (class III) and thigh-high (class II) garments are worn on top of one another during the day, and the waist-high garment alone is worn at night. 5 For patients with upper extremity lymphedema, a class II compressive sleeve and glove is worn during the day and night. 5 Compliance with compression is required for postoperative volume control. In the United States, the largest barrier to compliance with compression is financial, as garment coverage is insurance provider dependent and rarely entirely covered. The financial requirement of these garments is a key element of the preoperative counseling at our institution.
Between December 2017 and January 2020, 39 patients with lymphedema underwent 41 extremity debulking procedures at our institution. 2 For 23 patients who underwent an upper extremity debulking, objective and subjective metrics both demonstrated marked improvement (Fig. 2). Median excess volume reduction utilizing circumferential measurement was 111% at 6 months and 116% at 12 months postoperatively. Median upper extremity L-Dex was 55.2 (Q1–Q3 33–65) preoperatively versus 26.3 (Q1–Q3 14–32) at 6 months and 23.2 (Q1–Q3 17–27) at 12 months postoperatively. Subjective measurements were similarly improved. The mean overall quality of life (QOL) reported at the preoperative surgical consultation was 6.5 versus 8.3 at the last point of contact with the patients, an average of 8 months (standard deviation [SD] 4.5 months) after the debulking operation.
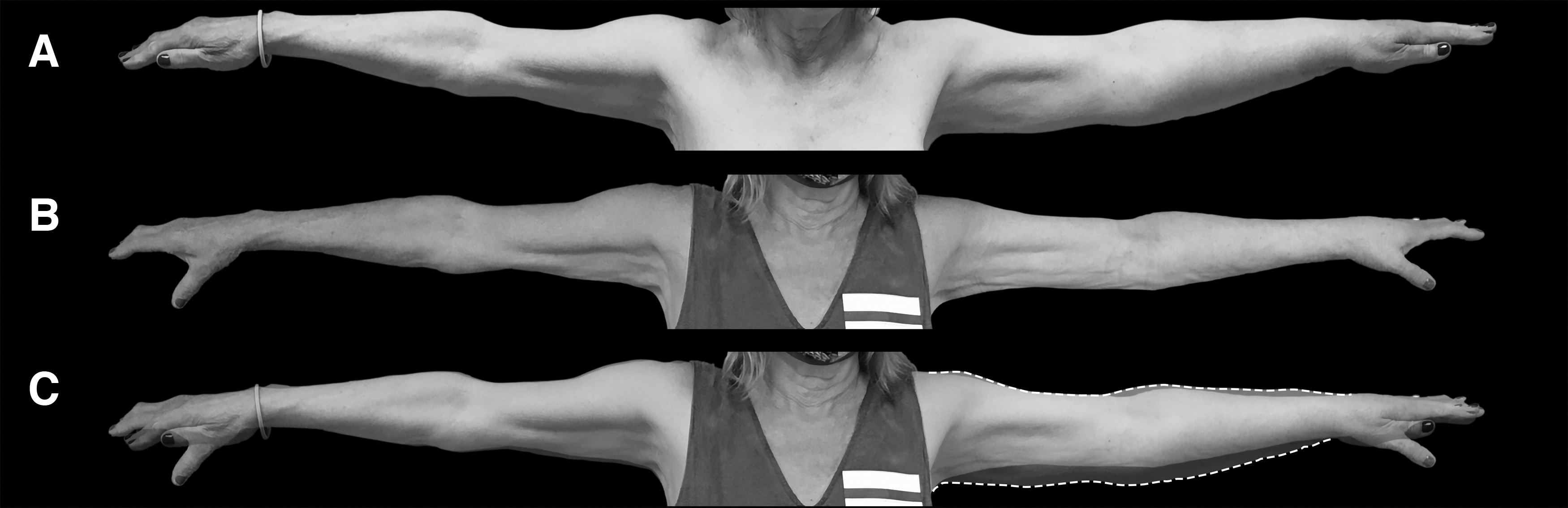
Patient before and after an upper extremity debulking.
Eighteen debulking procedures of the lower extremity were performed during this time period. Median excess volume reduction was 82% at 6 months and 115% at 12 months postoperatively. Median lower extremity L-Dex was 68.2 (Q1–Q3 47–87) preoperatively versus 21.5 (Q1–Q3 15–37) at 6 months and 20.3 (Q1–Q3 7–46) at 12 months postoperatively. The mean overall QOL improved from 5.9 to 8.5 an average of 9.1 months after the debulking operation (SD 4.9 months).
Debulking with power-assisted liposuction is an effective treatment for chronic lymphedema, supported by improvement in both objective and subjective metrics. 2 Debulking can stand alone with lifelong postoperative compression, or can be the first stage in a two-part surgical treatment, where the second stage is a physiological procedure after long-term postoperative volume control is established. Although no operative or other treatment for chronic lymphedema is curative, this treatment approach shows great promise in reducing disease burden for the long term and assisting patients in resuming a more normal life.