
Abstract
Background:
This study aimed at understanding the trend in extracellular fluid (ECF) change and estimating the efficacy of the early complex decongestive therapy (CDT) program in terms of prevalence of lower limb lymphedema, as well as at identifying the quality of life (QoL) associated with response to CDT after gynecological cancer therapy.
Methods and Results:
Thirty-one patients undergoing gynecological cancer treatment were enrolled and randomly assigned to the CDT and control groups. In the CDT group, CDT was started within 2 weeks after surgery for 30 minutes a day, for 2 weeks (5 days per week). The patients' QoL was assessed through the European Organization for Research and Treatment of Cancer Quality-of-Life Questionnaire; version 3. Inbody S10® (Biospace, Seoul, South Korea) was used to calculate the ECF. The assessment was performed at pre- and post-surgery and at 3, 6, and 12 months after surgery. Statistically significant differences, in favor of the CDT group, were encountered at the 3-month follow-up visit, especially with respect to the QoL score. Regarding the prevalence of lymphedema, no significant difference was observed between groups. The mean value of the impedance ratio was low in the CDT group during the entire 12 month follow-up.
Conclusions:
The results of the present study show that early CDT had a positive effect on the prevalence of lymphedema and body composition. Long-term follow-up studies with a larger sample size are needed to warrant the time-group effect of early rehabilitation.
Introduction
Lymphedema is a chronic disease in which protein-rich fluid accumulates in the interstitial space because of abnormal lymphatic circulation. Secondary lymphedema is an important side effect after breast cancer surgery, and it is reported to occur in 5%–56% of patients within 2 years after axillary node resection. 1 In most of these patients (71%), it is said to occur within 1 year after surgery. 2 Once the lymphedema has occurred, not only are there functional defects, such as reduced range of motion, of the affected upper limb, but it is also vulnerable to infection, the circumference increases, and patients often experience heaviness, discomfort, and disability in activities of daily life.3,4
Lymphedema of the lower limb has been far less studied than in the upper limb. Research on lower limb lymphedema after gynecological cancer has been limited to retrospective studies; there are a lack of guidelines for standardized diagnosis and evaluation, making it difficult to treat patients. 5 It is also becoming more difficult to evaluate lower limb edema when accompanied by deep-vein thrombosis, congestive heart failure, or drug use.
Currently, there are more than 1 million survivors of cancer in the United States, which is growing every year, and there is an increasing interest in the long-term side effects and treatment of gynecological cancer. The incidence of inguinal–femoral lymph node resection in gynecological malignancies is 25%–67%, which is the most common cause of lower limb edema. 6 In most studies, lower limb edema was diagnosed within 1 year after treatment, 5% was diagnosed before 1 month, and 20% was reported after 1 year.5,7,8
Although there are complex decongestive therapy (CDT), medication, and surgical methods available for the treatment of lymphatic edema, CDT is the first recommended treatment by a systematic literature review. 9 The CDT is a method designed to reduce the volume of edema, maintain skin health, and stimulate the lymphatic vessels to remove stagnant epilepsy proteins. The CDT is used for manual lymphatic drainage (MLD), skin care, remedial exercise, and external compression. It is reported that CDT performed early in patients who did not have edema after breast cancer surgery decreased the incidence of lymphedema 10
Although there have been recent attempts to reduce the risk of lymphatic edema, such as counseling, exercise training, and early diagnosis, there is still a lack of research and analysis on prevention strategies and obtaining an early diagnosis of lymphatic edema. In particular, as the incidence of lower limb swelling after gynecological cancer surgery increases, the need for a prospective study is urgent. In several studies on lymphedema of the lower extremities, it has been reported that CDT effectively reduced edema in these patients. 11 However, studies on the prevention of lymphedema in the lower extremities are very rare.
Therefore, the purpose of this study was to understand the trends in extracellular fluid (ECF) changes that cause lymphedema, analyze the effect of early CDT on the prevalence of lymphedema after gynecological cancer surgery, and identify the quality of life (QoL) associated with the response to CDT.
Materials and Methods
Patients
In the screening stage of patients who underwent surgery for gynecological cancer, the patient's medical records and interviews were used to confirm the selection and applicability of the exclusion criteria. Patients with pelvic or inguinal lymph node dissection for cervical, endometrial, or ovarian cancer, Eastern cooperative oncologic group performance status 0 or 1, with no complications except for simple wound infection after surgery were enrolled. Those with a history of lymphedema of the lower extremities or chronic edema of the lower extremities, with the presence of other diseases (congestive heart failure, chronic kidney disease, and chronic liver disease), with a history of previous surgery for vascular disease of lower extremities or for cancer other than gynecological cancer, with a history of radiation therapy for the pelvis, abdomen, perineum, or lower extremities, and those who did not understand or disagreed to the consent form were excluded.
Forty-seven patients were assessed for eligibility, and 31 patients completed the study (Fig. 1). The study protocol was approved by the institutional review board (IRB) of our hospital (IRB No. 2015-08-034), and informed consent was obtained from all participants.
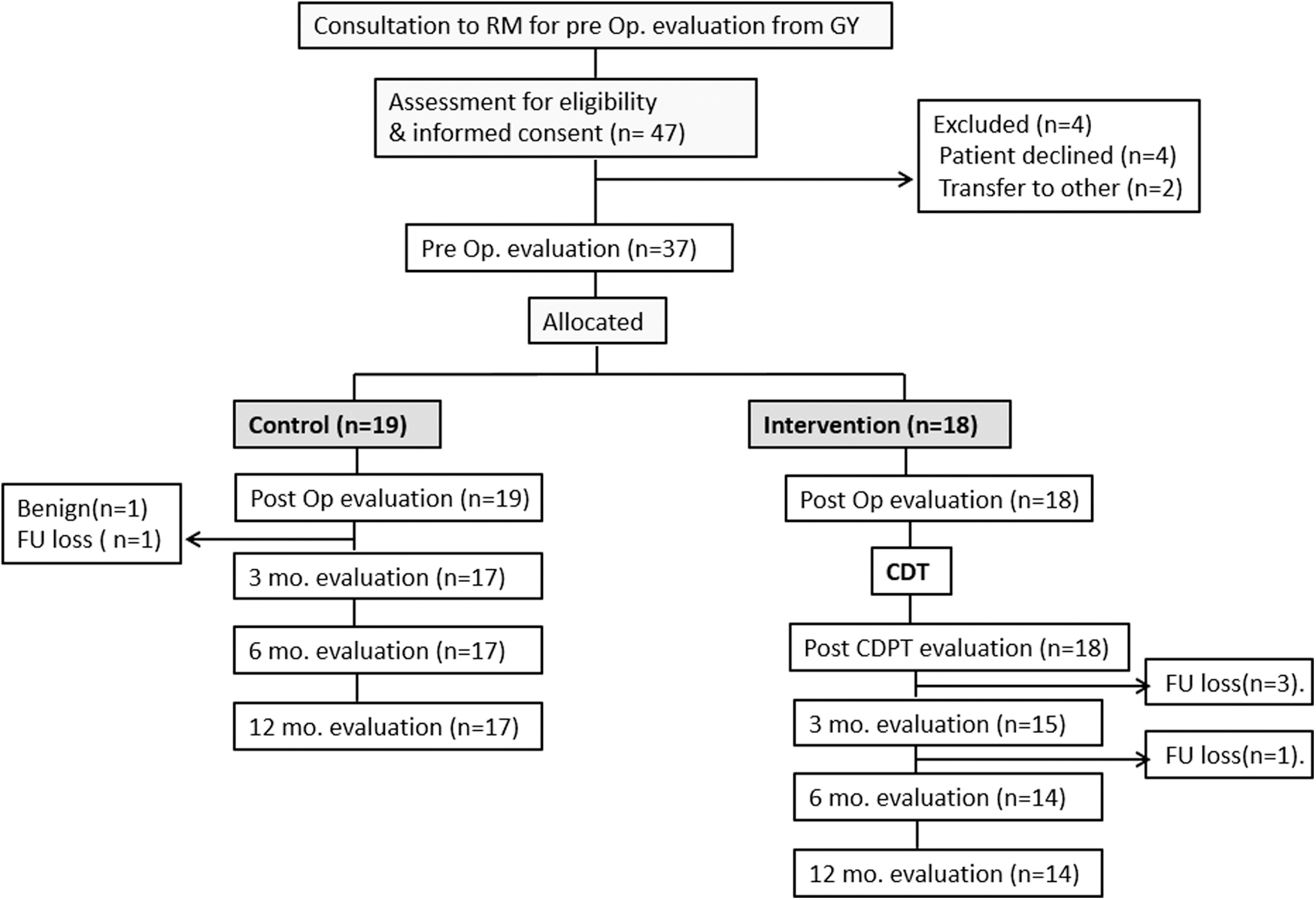
Flow of the study.
Patients were randomly assigned to two groups: CDT and control. At baseline (time of study entry), the patient's body fluid composition was recorded by using the bioimpedance spectroscopy (BIS; Inbody S10®; Biospace, Seoul, South Korea). Follow-up body fluid composition was assessed at 3, 6, and 12 months postoperatively. The QoL questionnaire was evaluated at 3 and 12 months after surgery.
Intervention
In the CDT group, CDT was initiated within 2 weeks after surgery. A total of 10 sessions (5 times/week, for 2 weeks) were performed. The CDT consisted of MLD, compression therapy, skin care, and remedial exercise. The MLD is a light and rhythmic form of stretching of the superficial skin. The MLD technique included stationary circles, pumping, rotational strokes, thumb circles, and scooping with varying degrees of light pressure. Pneumatic compression was applied in both groups. A multilayer low-stretch bandage was placed on the lower limb in case lymphedema was diagnosed by BIS at postoperation evaluation. The patients were instructed on remedial exercises, including isometric exercise and skin and nail care, which were performed at home. In the control group, one session of education consisted of instructions about secondary lymphedema, possible precipitation factor; strategies to prevent lymphedema were performed. The CDT and educational strategy were performed by one certified physical therapist.
Assessment
Bioimpedance analysis
Measurements were performed in the supine position. The BIS was used to assess ECF. The 1 kHz impedance ratios were used for analysis. Since impedance declines as ECF increases, the measured value of bioimpedance is expressed as the impedance ratio of the arm/leg. Lymphedema was considered present when the ratio of impedance of the arm/leg exceeded 2 standard deviations (SDs) from the mean normative ratios, assessed separately for the dominant and nondominant side; dominance was determined by the side used for writing. 12
Prevalence calculation
Point prevalence was calculated by counting the number of subjects who were diagnosed as having lymphedema at each assessment phase (baseline, postop. post-CDT, and -3, -6, and 12 months follow-up).
QoL questionnaire
The GCLQ-K (Korean version of the Gynecological Cancer Lymphedema Questionnaire) and EORTC QLQ-C30 (European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30) were used for evaluating lymphedema-related symptoms and QoL. The GCLQ is an effective tool for screening for lymphedema in patients with gynecological cancer. This questionnaire includes 20 items involving seven symptoms (physical functioning, numbness, general swelling, infection symptom, heaviness, aching, and limb swelling). If patients have five or more of the seven symptoms in the lower extremities, they can be classified as having lower limb lymphedema. The GCLQ-K has high internal consistency and reproducibility. 13 Each item is scored as 0 or 1, for answers of “no” and “yes,” respectively, within the previous 4 weeks. The EORTC QLQ-C30 is a 30-item questionnaire consisting of 5 function scales (physical, functional, cognitive, emotional, and social performance), 3 symptom scales (fatigue, pain, and nausea and vomiting), and scales of QoL and overall health status. With the EORTC QLQ-C30, a higher score means better function in the function scales and more symptomatic problems in the symptom scales. This questionnaire is used worldwide for many kinds of cancer and has been fully validated. 14
Statistics
Continuous data were expressed as mean ± SD. The Chi-square test was used to compare between two groups over time. p < 0.05 was considered statistically significant. All statistical analysis was performed by using SPSS 22.0.
Results
Table 1 presents the demographic and disease characteristics. This study included 31 patients who underwent surgery for cervical, endometrial, or ovarian cancer, with 17 patients in the control group and 14 in the CDT group.
Demographic Characteristics
Data are expressed as mean ± SD or number of patients.
BMI, body mass index; CDT, complex decongestive therapy; SD, standard deviation.
The mean impedance ratio increased over time up to 6 months after surgery in the control group. In the CDT group, the mean impedance ratio decreased immediately after CDT, and it slowly increased up to the 3-month follow-up; however, at the 6-month follow-up, it tended to be close to that of the control group. At the 12-month follow-up assessment, the impedance ratio in the control group had increased, but that in the CDT group tended to be maintained or decreased. For the entire 12 months, the mean value remained low in the CDT group (Fig. 2).
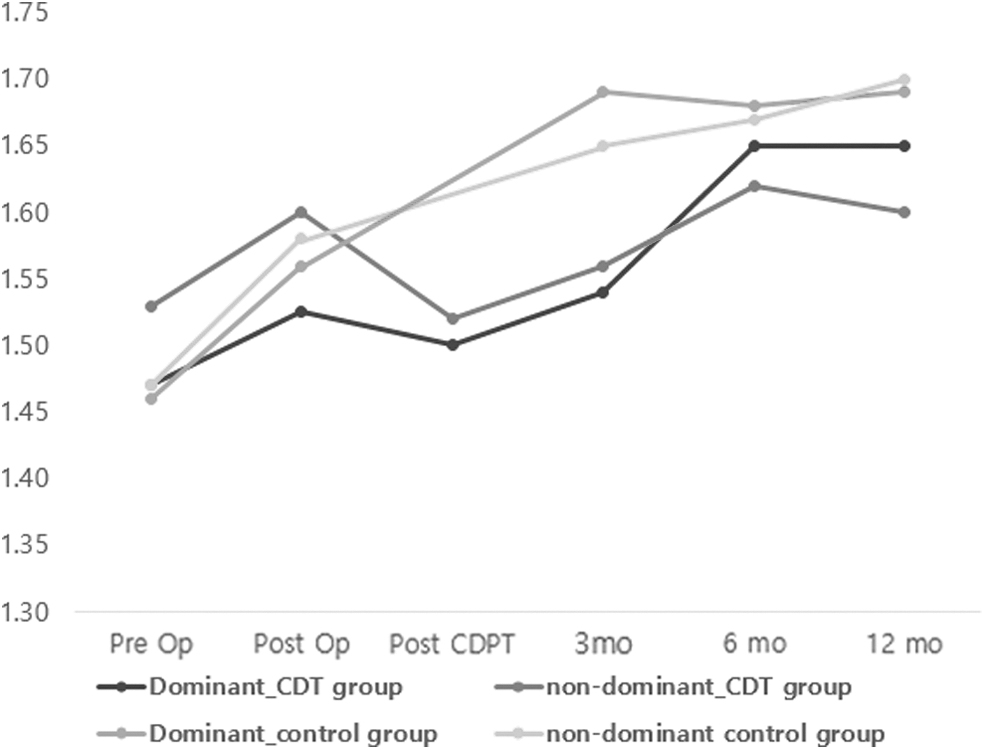
Arm-to-leg impedance ratio trend.
The point prevalence of lymphedema after surgery was 17.6%–23.5% in the control group and 14.3%–21.4% in the CDT group when including all gynecological cancer types; there was no statistically significant difference between group (Table 2). The prevalence of lower limb lymphedema increased over time up to 6 months after surgery in both groups. According to the cumulative prevalence of lymphedema, by 12 months after surgery, 35.3% in the control group and 28.6% in the CDT group had measurable lymphedema. No significant difference was observed between the two groups over time (Table 3).
Point Prevalence of Lymphedema up to 12 Months Post-Surgery for Gynecological Cancer
Cumulative Prevalence of Lymphedema up to 12 Months Post-Surgery for Gynecological Cancer
Statistically significant differences, in favor of the CDT group, were observed at the 3-month follow-up visit, especially with respect to the QoL score. In the CDT group, statistically significant differences were apparent in global health, physical, role, and emotional functions, as well as cancer-related symptoms such as fatigue and pain, nausea, and dyspnea on the EORTC QLQ-C30 (Table 4).
Quality of Life in Both Groups
Bold values indicates significant difference from the corresponding “control” values (p < 0.05).
EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire C30; GCLQ-K, Korean version of the Gynecological Cancer Lymphedema Questionnaire; QoL, quality of life.
Discussion
In the present study, we report the effect of early intervention using CDT on the prevalence of lower limb lymphedema and patients' QoL after surgery for gynecological cancer. Over time, there was no statistically significant difference in the prevalence of lymphedema between the two groups. However, the QoL was found to be significantly improved in the CDT group.
The CDT is the main treatment for lymphedema; it promotes the removal of fluid from the interstitial space to restore the balance between filtration and resorption. 11 In relation to early rehabilitation to prevent lymphedema, some studies have reported the effect of CDT relevant to breast cancer-related lymphedema. In a study by Lacomba et al., who researched the effectiveness of early physiotherapy on lymphedema after breast cancer surgery, secondary lymphedema was diagnosed four times earlier in the control group than in the intervention group. 10 In a similar context, we assumed that the implementation of manual lymph drainage after surgery for gynecological cancer in the early CDT group could have contributed to the better results regarding the prevalence of lymphedema.
Although it is likely that earlier intervention will result in better outcomes, in this study, there was no statistically significant difference in the prevalence of lymphedema. Regarding the trends of ECF change, in the CDT group, the mean value of the impedance ratio initially increased before decreasing again to the preoperative value after 2 weeks of CDT. The impedance ratio increased up until the 6-month follow-up assessment, and tended to approach that of the control group, although the mean value remained low. The CDT has been shown to be effective in lymphatic drainage, as it encourages a reduction in the interstitial fluid. Therefore, this could explain the effectiveness of early CDT and the prevention of secondary lymphedema in patients with gynecological cancer; the period of lymphedema-free days is expected to increase at least during the few months of follow-up.
This study has some limitations, including the small sample size recruited from a single hospital and the short duration of follow-up (1 year after surgery). At the 12-month follow-up assessment, the impedance ratio showed different trends in the two groups: It was maintained or decreased in the CDT group, and it increased in the control group. A long-term follow-up after 12 months would have been beneficial to sufficiently observe the effect of CDT. Another limitation is that we used particular criteria for diagnosing lymphedema. In this study, lymphedema was diagnosed via BIS, which is considered the most sensitive objective assessment. There was no definite reference value for ECF volume for Asians or diagnostic criteria for bilateral lymphedema through BIS. Therefore, we established the criteria for the diagnosis of bilateral lymphedema based on a study by Hayes et al. 12 However, the BIS equipment used in that study is not the same as that used in ours. In addition, all participants in the study were Australians and New Zealanders; therefore, the biological reference value may be different from that of Asians. In another study by Hayes et al., the diagnostic standard was set to ±1 SD; however, in this study, ±2 SD was set as the diagnostic standard for lymphedema. Therefore, the prevalence of lymphedema may be less than that reported in a prior study.
Nevertheless, this study shows evidence of the positive effect of early CDT in the prevention of secondary lymphedema and QoL by using an objective measurement tool. Seventy-five percent of cases of lower limb lymphedema after gynecological surgery present by 12 months post-surgery. In this study, the first case of lymphedema occurred most frequently in the period from 3 months after surgery up until the 12-month follow-up. Regular assessment and early CDT, at least during the first year after surgery, is required.
Conclusions
Early CDT has been shown to be effective in lymphatic drainage, as it encourages a reduction of ECF and plays a role in improving QoL after gynecological surgery. Regarding the prevalence of lower limb lymphedema after gynecological cancer surgery, the effect of early CDT was positive. Long-term follow-up studies with a larger sample size are needed to determine the time-group effect of early rehabilitation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by Chungnam National University Hospital Research Fund, 2015.