
Abstract
Background:
We aimed to clarify whether pathological changes in skin and subcutaneous tissue with lymphedema affected the skin hardness sensed by palpation.
Methods and Results:
In 50 patients with unilateral legs with lymphedema (LE), the skin hardness of the lower inner thigh and lower inner calf was determined using a scale ranging from 1 (softest) to 7 (hardest) based on palpation. Then, the skin hardness was correlated with the measurements of skin/subcutaneous tissue ultrasonography images obtained from the palpated parts. Multivariate logistic regression analysis demonstrated that dermal thickness was a significant factor that affected the difference in skin hardness between the LE and the contralateral asymptomatic leg for both thigh (p < 0.05) and calf (p < 0.01). When the thigh and calf in the LE were individually studied, subcutaneous echogenicity (p < 0.05), indicating subcutaneous inflammation/fibrosis, and subcutaneous thickness (p < 0.01) also seemed to affect skin hardness, respectively.
Conclusions:
The skin hardness sensed in the LE seemed to be affected predominantly by dermal thickening. In addition, the pathological changes in the subcutaneous tissue caused by LE seemed to have an impact on skin hardness. Clinical Trial Registration number 2020–150.
Introduction
The hardness of skin with lymphedema can affect patients' quality of life and requires careful assessment. 1 However, the concept of hardness is ambiguous. Killaars et al. used Cutometer® to investigate the skin elasticity and viscoelasticity in arms with lymphedema, with which they demonstrated an impaired elasticity. 2 Sano et al. used Indentometer® in addition to Cutometer to study the legs with lymphedema (LE). They found that elasticity age of the skin was significantly increased as lymphedema stage progressed, and this could be related to decreased elastic fibers in the dermis and upper layer of the subcutaneous tissue. 3 Despite these contributions, the relation between the skin hardness reported by patients or therapists and the pathological changes in mechanical properties is still unclear. This is possibly because the sensation of hardness is very much subjective, and also because the skin consists of multiple layers, and its characteristics, including nonlinearity, viscoelasticity, and load history dependency, in addition to pathological changes, may not be represented using any single parameter.4,5 We previously attempted to use ultrasound elastography to measure the strain of skin and subcutaneous tissue with lymphedema, but the sensitivity was low. 6 Thus, we started to use a scale on which commercial sponges of various hardness are aligned to grade the skin hardness assessed by palpation. Although this is only available in our clinic, it is useful to share the same sense of hardness among patients, physicians, and therapists, and also to evaluate the skin hardness in a semi-quantitative manner. In this study, we investigated which pathological changes in the skin and subcutaneous tissue caused by lymphedema affected this subjectively sensed skin hardness using the abovementioned scale and ultrasonography findings, which would enrich the information obtained by skin palpation.
Methods
This retrospective study was approved by the Institutional Review Board of Yamaguchi University Hospital (Center for Clinical Research, Ube, Yamaguchi, Japan, 2020–150), and the need for individual patient consent was waived. Between January 2018, when we started to use the abovementioned scale, and September 2020, 78 patients with unilateral leg LE visited our clinic. Of these, 50 patients agreed to undergo skin assessment and skin/subcutaneous tissue ultrasonography simultaneously, and these patients were included in the analysis. The patient characteristics are summarized in Table 1. At the time of their visits, the leg circumferences were measured at 10 cm above and 30 cm below the upper edge of the patella, which were included in the areas of scanning. Palpation of the skin and skin/subcutaneous tissue ultrasonography were performed as described hereunder.
Patient Characteristics
ISL, International Society of Lymphology.
Skin palpation
One of our staff (a physician and three therapists) in charge for each patient palpated the skin. Skin palpation was performed using the examiner's fingertip, and the sensed hardness was graded using a palpation scale (P-scale). The scale was set from 1 (softest) to 7 (hardest), as given in Figure 1. Three commercial sponges (Yahata Neji Corporation, Aichi, Japan), which were displayed according to their hardness in a DIY store, were obtained and cut into 10 × 5 × 5 cm cubes before being attached to a wooden board in order. The softest sponge (P-scale = 2) was as soft as the skin of a normal inner thigh; the hardest sponge (P-scale = 6) was as hard as skin with lipodermatosclerosis, and the hardness of the medium sponges (P-scale = 4) was the middle of these two sponges, as defined by the manufacturer. On the P-scale, 1 was softer than 2, 3 was between 2 and 4, 5 was between 4 and 6, and 7 was harder than 6. Palpation was performed while the patient was sitting on a bed with their legs stretched out to palpate their own legs. The P-scale was always determined based on the accordance between patients and the staff in charge. When there was disagreement, patients' sensation was adopted. In this study, the P-scale in the lower medial thigh and lower medial calf (hereafter referred to as the thigh and calf, respectively) were evaluated.
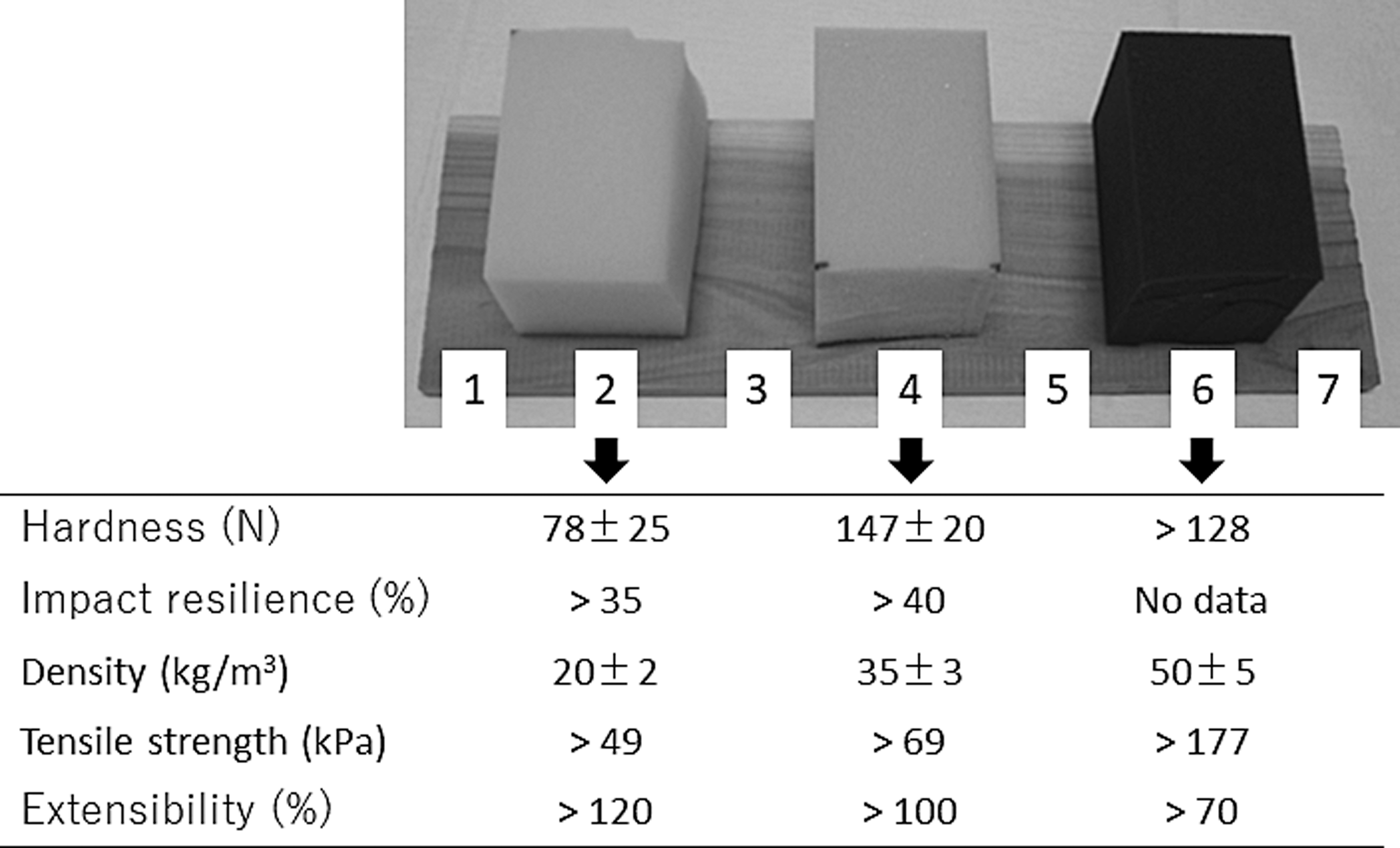
Palpation scale (P-scale). Information regarding the mechanical properties of commercial sponges was provided by the manufacturer (Yahata Neji Corporation, Aichi, Japan).
Skin and subcutaneous tissue ultrasonography
Each patient underwent skin and subcutaneous tissue scans using an ultrasound system (LOGIQ S6; GE Healthcare, Little Chalfont, Buckinghamshire, United Kingdom) with a 7- to 12-MHz linear transducer as we previously reported.
7
The images of the thigh (the lower half of the thigh, immediately anterior to the great saphenous vein) and calf (lower half of the leg, immediately posterior to the great saphenous vein) were evaluated, because these two sites would best represent tissue changes according to our previous work.
8
The probe was placed longitudinally on the leg. The size and gain were adjusted as necessary to optimize the image quality and boundary definition. In particular, when subcutaneous echogenicity (SEG) was evaluated, the B-mode gain was adjusted so that normal subcutaneous fat in the other parts of the body appeared black. The thickness of each structure was defined as follows:
Dermis: The distance between the deep echogenic border of the epidermal entrance echo and the deep echogenic border of the dermis (because an epidermal entrance echo does not reflect the true thickness of the epidermis).9,10 Subcutaneous tissue: The distance between the deep echogenic border of the dermis and the superficial echogenic border of the deep muscular fascia.
Because the borders of these structures were irregular and were not always located parallel to the epidermal surface, the distances were measured at three points (right, middle, and left) of each acquired image, and the average distance was recorded. SEG and subcutaneous echo-free space (SEFS) were graded as given hereunder. 7
SEG grade
Grade 0: No or only a slight increase in echogenicity in the subcutaneous layer. Horizontally or obliquely oriented echogenic lines caused by connective tissue bundles are clearly observed.
Grade 1: Diffuse increases in echogenicity in the subcutaneous layer. Echogenic lines are unclear but identifiable.
Grade 2: Diffuse increases in SEG. Echogenic lines are not identifiable.
SEFS grade
Grade 0: No SEFS.
Grade 1: Horizontally oriented (<45° to the skin) SEFS only.
Grade 2: Presence of vertically oriented (≥45° to the skin) SEFS bridging the horizontally oriented SEFSs.
Ultrasonography images were acquired by a qualified technician and graded using a single interpreter (K.S.). Representative ultrasonography images are given in Figure 2.
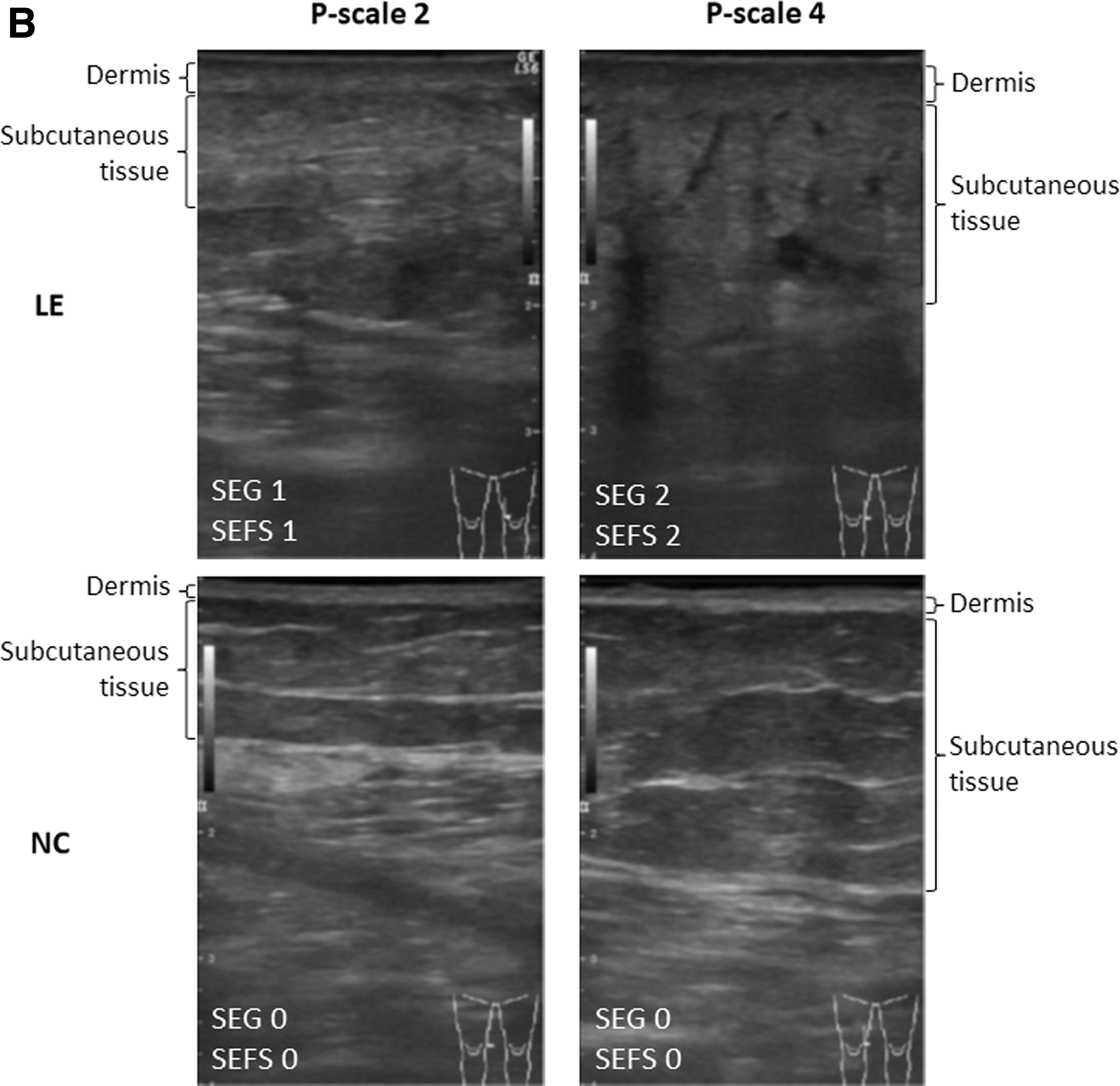
Representative ultrasonography images.
Statistical analysis
The results are reported as median (range) or count (percentage), unless otherwise indicated. The Kruskal–Wallis test was used to determine differences in measurements among the groups. The Mann–Whitney U-test was used for multiple comparisons. The χ 2 test was used to assess the differences in the P-scale and SEG/SEFS grades between the thigh and calf, or between the affected and unaffected legs. Logistic regression analyses were used to test the correlation between the P-scale and the measurements. Statistical analyses were performed using JMP 11.0 (SAS Institute, Cary, NC). Values of p < 0.05 were considered significant.
Results
Normal counterpart
Absence of lymphedema symptoms in normal counterpart (NC) was confirmed by physical examination and skin/subcutaneous tissue ultrasonography. The P-scale, circumferences, and ultrasonography measurements are summarized in Table 2. In the NC, the P-scale in the calf (3.5 [2–4]) was greater than that in the thigh (2 [1–4]). No P-scale exceeded 4 in the NC. In the calf, the dermis was slightly but significantly thicker, whereas the subcutaneous tissue was thinner than that in the thigh. In 13 of the NC, SEG 1 was observed only in the calf, and SEFS 1 was observed in only one calf but not in the thigh of the NC.
Measurements in the Legs of Patients with Unilateral Lymphedema
Data are expressed as median (range). *p < 0.05 versus thigh, †p < 0.0001 versus LE.
LE, Leg with lymphedema; NC, normal counterpart; SEFS, subcutaneous echo-free space; SEG, subcutaneous echogenicity; SLEB, subepidermal low-echogenic band.
The ultrasonography measurements according to the P-scale are given in Figure 3. The dermal thicknesses both in the thigh and calf of NC were roughly constant, regardless of an increase in P-scale, although a very mild increase in dermal thickness according to the increase in P-scale was observed in the calf (p < 0.05). When the P-scales were the same, the dermal thicknesses in the thigh and calf were not significantly different. The subcutaneous thickness varied depending on the patient's physique (thin or obese), and no certain trends according to P-scale could be found. Logistic regression analyses revealed that the most significant factors affecting the P-scale in the thigh and calf of NC were age, that is, increased age was associated with decreased P-scale, and dermal thickness, respectively. Body mass index had no significant impact on P-scale (Table 3).
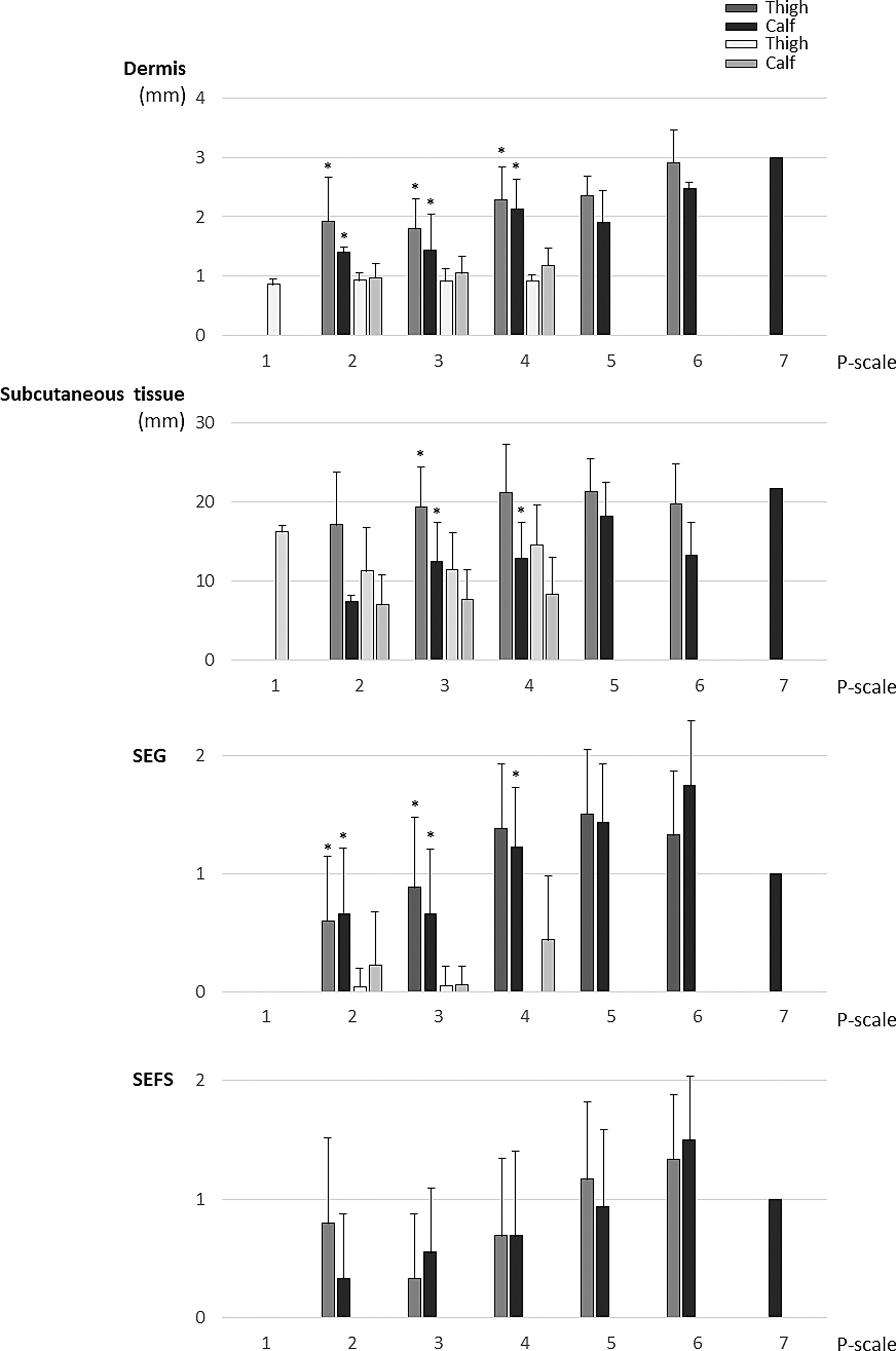
Ultrasonography measurements according to P-scale. Lymphedema, NC, SEG, and SEFS: as in Figure 2. *p < 0.05 versus NC. When increases in SEG or SEFS are not found in NC, statical analyses were not performed. P-scale 7 was recorded only in one leg, and therefore error bar was not attached.
Factors Affecting the P-scale
p-Values are demonstrated.
Legs with lymphedema (LE)
In LE, the P-scale in the calf (4.5 [2–7]) was greater than that in the thigh (4 [2–6]) (Table 2). In contrast to the NC, the median dermal thicknesses in the thigh and calf were not significantly different. The circumference and ultrasonography measurements were all greater in LE legs than in NC.
As given in Figure 3, the dermal thicknesses in the thigh and calf of LE were not significantly different, but were significantly thicker than those in the NC when the P-scales were the same. In contrast to the NC, the dermal thickness increased as the P-scale increased in both the thigh (p < 0.01) and calf (p < 0.0001) of LE. The subcutaneous thickness varied depending on the patient' physique and/or condition of disease, that is, proliferation of adipose tissue and/or edema of various severities, and no certain trends could be found. The SEG grade increased as the P-scale increased in both the thigh (p < 0.05) and the calf (p < 0.05), but no such tendency was found in the SEFS grade. Multivariate logistic regression analyses revealed that the significant factors that affected the P-scale in LE were dermal thickness and SEG grade for the thigh, and dermal and subcutaneous thickness of the calf (Table 3).
Difference between LE and NC
The difference in P-scales between LE and NC was correlated with the difference in ultrasonography measurements (Table 4). Because the subcutaneous thickness in NC legs (i.e., the control) varied widely among the individuals, % increases in subcutaneous thickness (value in affected leg—value in unaffected leg/value in unaffected leg) were calculated and assessed. Multivariate logistic regression analyses showed that the most significant factor affecting the difference in P-scales between LE and NC was the increase in dermal thickness for both the thigh (p < 0.05) and the calf (p < 0.01) (Table 4).
Factors Affecting the Difference in P-Scale Between the Legs
p-Values are demonstrated.
Discussion
The main findings in this study were as follows: (1) The most significant factor that affected the difference in the skin hardness sensed by palpation between LE and NC was the difference in dermal thickness, and (2) when the thigh and calf were individually assessed, the skin hardness in the LE were also affected by the condition of the subcutaneous tissue.
Dermal thickening is a dominant factor affecting the subjective skin hardness in LE
It is well known that the thickness of the dermis increases in LE. 11 Because the collagen content in the dermis contributes most to the hardness of the skin, and because the superficial layer affects the hardness of the skin more than the deeper layer,4,5 it is natural that dermal thickening affected the subjective skin hardness the most. In normal skin, a loss of collagen in the dermis progresses as the age increases. 12 We demonstrated that the subjective skin hardness decreased as the age increased in the thigh of the NC. Sano et al. reported a negative correlation between skin elasticity and age in the normal thigh skin, 3 which is in agreement with the current data. However, the correlation between skin hardness and age seemed to be abolished by a pathological increase in dermal thickness in legs with lymphedema.
Of interest, the skin thicknesses were different between LE and NC even when the P-scales were the same. One possible explanation for this result is the difference in the composition of the dermis. In normal human skin, 75% of the dry weight of skin is collagen, of which 80%–90% is type I and 8%–12% is type III. 12 However, it has been reported that the increase in collagen type III in dermal fibrosis in lymphedema was significantly greater than type I. 13 This may be related to the difference in skin hardness between LE and NC because collagen type I is known to be stiffer than type III. 14 Another possible explanation is the impact of an increase in subcutaneous fat, as described hereunder.
Impact of the subcutaneous tissue on skin hardness in LE
When the thigh and calf in the LE were individually assessed, factors regarding the subcutaneous tissue were found to be relevant. The echogenic bands observed in the subcutaneous tissue are superficial fasciae composed of collagenous fibers surrounded by mucinous proteoglycans and glycosaminoglycans. In general, thinner subcutaneous layers are associated with greater echogenic band densities, 15 and consequently, they would probably be felt harder; this may partly explain why the calf was felt harder than the thigh in both the LE and NC.
Adipose tissue proliferation and fibrosis, mainly found in the interlobular septa, are the major changes in the subcutaneous tissue with lymphedema. 16 It is known that impaired lymph transport can cause adipose tissue proliferation, possibly by a mechanism such as reverse cholesterol transport. 17 The thicker subcutaneous tissue (fat) is likely to disperse the mechanical forces, and as a result, it might have felt softer. Indeed, the thigh of the NC with thin skin and thick subcutaneous tissue was felt to be very soft, that is, with a P-scale = 1. At the same time, subcutaneous tissue fibrosis progresses in LE through chronic mixed T helper cell inflammatory reactions. 18 These reactions can be observed using ultrasonography as increased SEG, which represents the subcutaneous tissue with acute/chronic/ex-inflammation caused by inflammatory infiltrate with or without fibrosis.19,20 Adipose tissue in LE contains more collagen fibers and fewer elastic fibers, 21 and as a result, it might have felt harder than normal adipose tissue 21 ; this would explain why the SEG grade was positively correlated with P-scale in both the thigh and calf with lymphedema in this study. The edema is another characteristic of lymphedema, and the accumulation of fluid in the subcutaneous tissue, which can be observed as an increase in SEG and SEFS grade, 22 might also be felt harder. The overall impact on the skin hardness depends on the balance between adipose tissue proliferation (soft) and fibrosis (hard), but further studies are necessary to determine the impact of these on skin hardness.
Limitations
This study has several limitations. First, it might be difficult to draw definite conclusions because the number of subjects included in this study was small and this was a retrospective study. Furthermore, it is known that proliferation of the epidermis is evident in LE, and this is likely to affect the subjective skin hardness. However, observation of the epidermis requires ultrasonography with a resolution of >20 MHz, which was not available in our clinic. Practically, palpation of the skin may be difficult when the subcutaneous tissue is very thin, which is often encountered in the calves of thin patients. In such patients, the hardness of the muscle might have been sensed, which again could have affected the results. Indeed, the subjectively sensed hardness is ambiguous, and all sensations, such as increased firmness, increased viscosity, and reduced elasticity, may all be expressed as hard by patients. Therefore, it may be difficult to mimic skin with lymphedema using sponges alone. Both in P-scale and ultrasonography measurements, intra- and inter-rater reliability has not been validated. In addition, these were interpreted by single interpreter without blinding, which could reduce the reliability of data.
Conclusion
We found that dermal thickening in LE affected the subjectively sensed skin hardness of LE. The pathological changes in the subcutaneous tissue caused by lymphedema also had a certain impact on subjective hardness in subjectively sensed hardness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.