
Abstract
Background:
Recurrent cellulitis has high impact on physical, psychological, and social aspects for lymphedema patients. We speculated that identification of characteristics of skin and subcutaneous adipose tissue with cellulitis history can help considering new approach for prevention of recurrent cellulitis in lymphedema patients. Therefore, in this study, we aimed to noninvasively identify the ultrasonographic features of skin and subcutaneous tissue of lymphedema in patients with a cellulitis history.
Methods and Results:
This was a cross-sectional study, and all data were collected from patients' medical records. We assessed ultrasonographic images of the lower extremity of patients with lymphedema that were obtained in a lymphedema clinic. The ultrasonographic images were analyzed on the basis of the following five features: dermal hypoechogenicity, unclear dermal border, unclear superficial fascia, increased subcutaneous echogenicity, and subcutaneous cobblestone appearance. Fifty-two ultrasonographic images from 19 female patients with lower extremity lymphedema, including 8 with and 11 without a cellulitis history, were analyzed. The proportion of dermal hypoechogenicity on the upper leg was significantly higher in the patients with than in those without a cellulitis history (75.0% vs. 9.1%, p = 0.006).
Conclusion:
Cellulitis history in lymphedema patients appears to be associated with dermal hypoechogenicity, particularly in the proximal lower extremity. This finding suggests that it may be the initial step to consider new approach for prevention of recurrent cellulitis in lymphedema patients.
Introduction
Recurrent cellulitis is the most common complication of lymphedema and is related to the reduction of patient quality of life due to its impact on physical, psychological, and social aspects.1–3 Owing to the vicious cycle between recurrent cellulitis and worsening lymphedema, 4 the identification of characteristics of skin and subcutaneous adipose tissue with cellulitis history can help considering new approach for prevention of recurrent cellulitis in lymphedema patients.
Cellulitis is an acute inflammatory condition of the dermis and subcutaneous tissue caused by infection with Staphylococcus aureus, Streptococcus pyogenes, or various other exogenous bacteria. 5 High prevalence rates of cellulitis ranging from 49.0% to 52.8% were reported in patients with lower extremity lymphedema.6,7 Of these patients, 50.4% had a recurrent cellulitis within a year. 6 The vicious cycle between the recurrence of cellulitis and worsening edema was also suggested. 4 This concept is supported by the fact that compression therapy inhibits the recurrence of cellulitis in patients with edema. 8 Therefore, effective prediction and prevention of cellulitis recurrence are highly required.
Lymphedema is caused by insufficient lymphatic circulation that induces inflammation response.9,10 In this response, macrophages are the major players to the release of transforming growth factor (TGF)-β and interleukin 6 (IL-6).9,11 TGF-β contributes to the progression of lymphedema by inhibiting lymphangiogenesis and enhancing fibrosis in lymphedema tissues.8,12 IL-6 is a proinflammatory cytokine that mediates chronic inflammation and adipose metabolism.13,14 Abundant IL-6 expression was reported in lymphedema tissues.11,13 Puel et al. reported recurrent cellulitis in a child with autoantibodies for IL-6, 15 suggesting that IL-6-mediated latent inflammation may promote cellulitis recurrence. Therefore, we speculated that history of cellulitis caused to showing the characteristics such as latent inflammation.
We focused on ultrasonography, which is a potential tool for noninvasive identification of specific characteristics in lymphedematous skin and subcutaneous adipose tissue. To date, some studies have reported the ultrasonographic features of lymphedema.9,16–18 Increased echogenicity and the disappearance of the superficial fascia of the subcutaneous tissue reflect the inflammatory status, whereas the cobblestone appearance of adipose tissue indicates severe edema.17,18 However, no study has shown the relationship between ultrasonographic features and the history of cellulitis in patients with lymphedema.
The purpose of this study was to noninvasively identify the ultrasonographic features related to cellulitis history in patients with lower extremity lymphedema.
Materials and Methods
Study design, participants, and setting
This was a cross-sectional observational study. We collected all data from the patients' medical chart from January to October 2019. The facility was at a lymphedema outpatient clinic of a specialized lymphedema hospital in Tokushima prefecture, Japan. The hospital has a physician specializing in lymphedema and nurses and physiotherapists with significant experience in lymphedema management. The inclusion criteria were patients diagnosed as having lower extremity lymphedema who were >20 years of age. The exclusion criteria were lymphedema of grade 0 or I severity according to the International Society of Lymphology (ISL) classification, 1 bilateral lymphedema, a lymphedema duration of <1 or >15 years, and the presence of acute attacks of cellulitis in the past 1 month before the ultrasonographic examination.
The study protocol was approved by the ethics committee of the Graduate School of Medicine of the University of Tokyo (No. 2020287NI) and conducted in accordance with the 2008 revision of the Declaration of Helsinki.
Ultrasonographic examination
The ultrasonographic images of both limbs were obtained by a physician who specialized in lymphedema and routinely performed ultrasonographic examinations for lymphedema management. The device used was an Aplio300 with a 10- to 16-MHz linear probe (Canon Medical System, Tochigi, Japan). Ultrasonographic gel was applied liberally to the skin, and the probe was placed longitudinally on three medial sites, namely the thigh, upper leg, and lower leg. The thigh was 15 cm above the knee, the upper leg was 10 cm below the knee, and the lower leg was 20 cm below the knee. The field size was set to a depth of 40 mm. The B-mode gain and dynamic range were adjusted to the proper level for each measurement to clearly visualize the target area.
Analysis of ultrasonographic images
The ultrasonographic images of the affected limbs were reviewed by a researcher with experience in studies using ultrasonography and an expert sonographer with >20 years of experience. The images of the unaffected limbs were used as reference images. The following five features were analyzed in this study (Fig. 1):
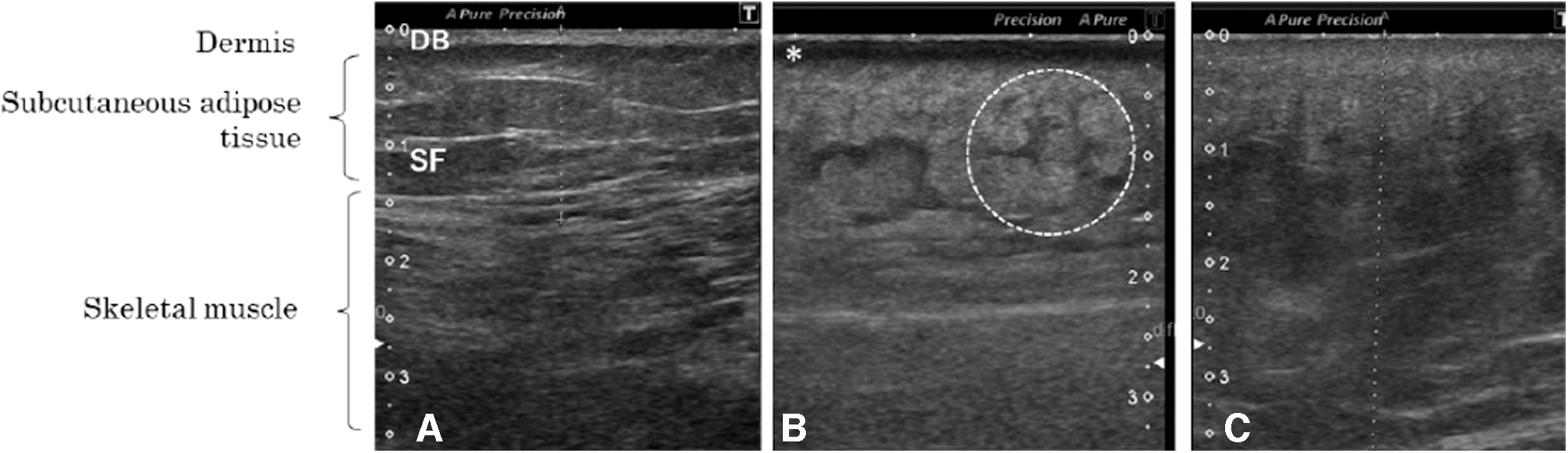
Representative ultrasonographic images of the dermis and subcutaneous adipose tissue of normal limbs and limbs with lymphedema.
Dermal hypoechogenicity: Dermal echogenicity reflecting a relatively high collagen density19,20 in the normal state. Some images of the patients with lymphedema showed absolutely low echogenicity on the dermal layer.
Unclear dermal border: In normal skin, the border between the dermis and subcutaneous adipose tissue is clearly observed as a hyperechoic line. The dermal border was unclear in some of the patients' images.
Unclear superficial fascia: The superficial fascia, which is a fibrous connective tissue among lobules of subcutaneous adipose tissue, appears as continuous hyperechogenic line. 21 In some images of the subcutaneous tissue, the superficial fascia was not clearly visible.
Increased subcutaneous echogenicity: In reference images, the echogenicity of the subcutaneous adipose tissue is low except for the superficial fascia. Homogeneously increased echogenicity was observed in some patients' images. This feature reflects the inflammatory status of the subcutaneous adipose tissue. 22
Subcutaneous cobblestone appearance: Swelling of the subcutaneous adipose tissue is generally observed as having a cobblestone appearance, which is also called the echo-free space. It shows round fat lobules in lymphedematous skin9,17 and at the onset of cellulitis. 23
Individual patient and edema characteristics
We collected individual patient and lymphedema characteristics, including age, gender, height, and body weight to calculate the body mass index, lymphedema type (primary or secondary), lymphedema severity by ISL classification, cancer history (uterine, ovarian, or others), experience of chemotherapy (yes or no), experience of radiation therapy (yes or no), experience of surgical operations for lymphedema (e.g., lymphaticovenous anastomosis and/or liposuction; yes or no), lymphedema sites (left or right), lymphedema duration (years), and cellulitis history (yes or no).
Statistical analyses
The proportion was described for the categorical data. Medians and interquartile ranges (IQRs) were used for the continuous variables. The characteristics of the patients and the ultrasonographic features were compared between the groups with and without a cellulitis history. The Fisher's exact test was used for categorical variables and the Wilcoxon rank-sum test was used for continuous variables. The statistical analysis was performed using Stata/SE version 14.2 (Stata Corp., College Station, TX). p-Values <0.05 were chosen to represent statistical significance.
Results
Participants
Thirty patients with unilateral lower extremity lymphedema were recruited. We excluded 11 patients because 7 patients had a lymphedema duration of >15 years and 4 patients had a lymphedema of ISL I. Finally, we analyzed 19 patients, including 8 with a cellulitis history (42.1%) and 11 without a cellulitis history (57.9%).
Individual patient and lymphedema characteristics
All 19 patients were female, and 94.7% of the patients had a secondary lymphedema after cancer (Table 1). The median (IQR) of age was 69 years (59–78 years), and the lymphedema duration was 48 months (12–96 months). The major lymphedema severity was ISL II (63.2%), followed by ISL late II (31.6%). No significant differences in individual patient and lymphedema characteristics were found between the groups with and without a cellulitis history.
Individual Patient and Lymphedema Characteristics With and Without a Cellulitis History
Categorical variables are expressed as n (%) and analyzed using the Fisher's exact test. Continuous variables are expressed as median (interquartile range) and analyzed using the Wilcoxon rank-sum test.
BMI, body mass index; ISL, International Society of Lymphology.
Ultrasonographic features
Fifty-two images, including 14 of the thigh, 19 of the upper leg, and 19 of the lower leg, were collected from 19 patients. Table 2 shows the proportions of ultrasonographic features at the thigh, upper leg, and lower leg. At the thigh and lower leg, no significant difference was found between the two groups. At the upper leg, the proportion of dermal low echogenicity was significantly higher in the group with than in the group without a cellulitis history (75.0% vs. 9.1%, p = 0.006).
Comparison of Ultrasonographic Features Between the Patients With and Those Without a Cellulitis History
Data are presented as n (%) and analyzed using the Fisher's exact test.
Discussion
This study shows the association of dermal hypoechogenicity with cellulitis history in patients with lower extremity lymphedema. This finding can contribute to understanding the characteristics of lymphedematous skin to consider new approach for prevention of recurrent cellulitis.
In this study, 52 ultrasonographic images from 19 female patients with lower extremity lymphedema who visited the lymphedema outpatient clinic were analyzed. Their median age, body mass index, proportion of lymphedema severity, and cellulitis history were similar with those of patients with lower extremity lymphedema who visited lymphedema outpatient clinics in other reports.7,17,24 Of the patients with lymphedema of moderate severity who visited the lymphedema outpatient clinic, ∼40% had a cellulitis history.
We found that the dermal hypoechogenicity on the upper leg was a significant feature of the affected limbs of patents with lower extremity lymphedema who had a cellulitis history. This study overcame the limitation of our previous study that stated that the result may be due to a difference in dermal echogenicity. 25 Dermal hypoechogenicity may indicate an extracellular fluid accumulation as a result of inflammation in the dermal layer. High water contents show hypoechogenicity25,26 because of the low acoustic impedance of water, which is 1.48 × 106 kg/m2·s. As patients who had an acute inflammation in the past month before the ultrasonographic examination were excluded, the association of dermal hypoechogenicity to recurrent cellulitis history suggested the presence of latent inflammation persisting for >1 month after the onset of clinical acute inflammation.26,27 Therefore, anti-inflammatory skin care may be a possible approach to prevent the recurrence cellulitis in patients with lymphedema.
Alterations of the ultrasonographic features of subcutaneous adipose tissue due to acute inflammation have been reported. Jaovisidha et al. reported increased echogenicity in cellulitis, fasciitis, myositis, or abscess. 22 In this study, increased echogenicity of the subcutaneous adipose tissue was highly prevalent in both groups, with no significant difference between the groups. This finding indicates that most patients with lymphedema have continuous inflammation of the subcutaneous adipose tissue regardless of cellulitis history.
Although lower extremity lymphedema affects the whole leg, different ultrasonographic features were reported for the thigh, upper leg, and lower leg regardless age, body composition, and lymphedema severity in the previous studies.16,24 Therefore, we separately analyzed the ultrasonographic images from the three sites. The association of dermal hypoechogenicity was found only in the upper leg. The possible reasons for this finding are the anatomical differences, and the different location of the previous cellulitis. Further studies are required to clarify the site-dependent tissue responses and the relationship between the sites of previous cellulitis and dermal hypoechogenicity.
The study has two major limitations. First, the information on cellulitis history was only “presence” or “absence.” Although the period from the previous to the current occurrence of cellulitis and the frequency, severity, and sites of the previous cellulitis can affect the results, we could not analyze them because of the limited information in the medical records from the medical facility. To evaluate the predictive validity of dermal hypoechogenicity for cellulitis recurrence, a prospective study is required. Regarding this limitation, although the ultrasonographic features were confirmed, whether saturation due to discussion with a sonographer if further features related the detailed information on cellulitis episodes was present is unclear. Therefore, a prospective study analyzing the relationship between the details of the cellulitis episode and ultrasonographic features could overcome this limitation. Second, the number of patients was small, and the data collection period was short. Further study in multiple facilities and with longer investigation period is needed.
Conclusion
Cellulitis history in lymphedema patients appears to be associated with dermal hypoechogenicity, particularly in the proximal lower extremity. This finding suggests that it may be the initial step to consider new approach for prevention of recurrent cellulitis in lymphedema patients.
Footnotes
Authors' Contributions
M.D. designed this research. H.S. and T.M. supervised the scheme of the study. Y.O. performed the ultrasonography for all the patients and collected individual patient and lymphedema characteristics. M.D. assessed the ultrasonographic images, and A.K. reviewed the results. M.D. and G.N. analyzed the statistical data. M.D. and T.M. interpreted the results. M.D. drafted the article. T.M. and H.S. supervised the writing of the article. All authors revised and approved the final version of the article.
Author Disclosure Statement
M.D. and T.M. belong to the department of Skincare Science, which is sponsored by Saraya Co., Ltd.; however, it is not related to this study. All other authors have no competing financial interests.
Funding Information
This study was supported by JSPS KAKENHI Grant-in-Aid for Scientific Research (C) (18K10307) from Japan Society for the Promotion of Science.