
Abstract
Background:
Secondary upper extremity lymphedema occurs after an insult such as surgery. One theory suggests underlying lymphatic dysfunction predisposing certain patients into developing secondary lymphedema. We aim to determine the rate of incidental edema in the contralateral upper extremity of patients with secondary unilateral lymphedema.
Methods and Results:
MRI of the upper extremities were obtained in patients with lymphedema who were referred by a lymphedema clinic from 2017 to 2019. Axial short-tau inversion recovery MR images of the symptomatic and contralateral arms were retrospectively reviewed and edema severity was graded. Interobserver agreement was calculated. Indocyanine green (ICG) lymphography was compared against MRI stage in symptomatic and contralateral. Age, symptom duration, body mass index (BMI), and history of chemotherapy were compared between patients with and without contralateral limb lymphedema. ICG severity was compared against MRI stage. Seventy-eight patients were analyzed. The MRI stages of symptomatic versus contralateral arms were 1.7 ± 1.1 versus 0.1 ± 0.4 (p < 0.00001). Interobserver agreement was 0.86 (0.79–0.94). Of the patients with MRI Stage 1 or above in the symptomatic arm (n = 64), 55 (82.1%) patients demonstrated no abnormality in the contralateral arm. Nine patients (14.1%) demonstrated asymptomatic edema (MRI Stage 1). The mean ICG lymphography stage of symptomatic versus contralateral arms was 1.83 ± 0.96 versus 0.04 ± 0.25 (p < 0.00001). There was no difference in the age, symptom duration, BMI, or history of chemotherapy between patients with or without edema in the contralateral arm.
Conclusion:
Asymptomatic contralateral edema was detected in 14.1% of patients with unilateral secondary upper extremity lymphedema using MRI modality.
Introduction
Secondary lymphedema in the upper extremity occurs in a subset of patients who are exposed to an injury or surgery, which damages the lymphatic flow in the arm and the axilla.1–5 Studies have implicated underlying systemic risk factors and even preclinical lymphatic dysfunction in predisposing certain patients to the development of secondary lymphedema.6–10 Since treating lymphedema in its early stages portends better outcome, 11 identification of lymphedema in the contralateral unaffected limb in patients who are at risk would improve prognosis through early intervention. However, the rate of incidental lymphedema in the contralateral limb in patients with secondary lymphedema is not well established.
Previous studies on patients with unilateral secondary lymphedema of the upper extremity reported up to 80% demonstrating lymphedema in the asymptomatic contralateral limb.12–15 However, these studies included <20 patients and used only one diagnostic testing modality to investigate the rate of contralateral limb lymphedema. Moreover, the techniques used in these studies require the administration of exogenous contrast for complete visualization of lymphatic dysfunction and it was not administered.
Diagnostic tools such as perometry, circumference measurements, and bioimpedance rely on a direct comparison between the symptomatic limb against the contralateral limb, which is assumed to be normal. However, these tests would be inaccurate if the contralateral limb exhibited any lymphedema, even if asymptomatic. Currently, investigation of the unaffected limb with indocyanine green (ICG) lymphography or lymphoscintigraphy requires administration of contrast. Noncontrast MRI can identify lymphedema and lymphatic channels without injecting contrast material and would be well suited to the task of noninvasively evaluating the contralateral limb of patients with secondary upper extremity lymphedema.14–17
A lymphedema staging system for MRI without using exogenous contrast has been described, which can be used to describe the severity of lymphedema in either limb, and offers the ability to detect subclinical lymphedema. 16 The purposes of this study was to utilize this MRI staging system to determine the rate of incidental edema in the contralateral upper extremity of patients with postsurgical unilateral lymphedema, and to compare this against the rate of contralateral lymphedema as detected by lymphoscintigraphy and ICG lymphography.
Materials and Methods
Patient selection
This retrospective study was approved by the institutional review board (IRB No. 2018P000085). Patients who were clinically diagnosed with secondary lymphedema of the upper extremity or who showed equivocal presentation on clinical examination were referred from the lymphatic center. The patients who underwent MRI and nuclear medicine lymphoscintigraphy between March 2017 and July 2019 were included. Patient demographic information and ICG lymphography results of the included patients were collected.
Magnetic resonance imaging
Compression garments were removed 48 hours before MRI. Dedicated both upper extremity MRIs were performed on a single 1.5 T scanner (Siemens Magnetom Aera) using two 13-channel body array coils. Patients were positioned supine with arms at the sides and palms facing medially. The contralateral arm was imaged as control. Each arm was imaged separately, with the nonaffected contralateral arm first, followed by the affected arm. The patient is positioned so that the target limb was at or as close as possible to the magnet isocenter. Axial short-tau inversion recovery (STIR, slice thickness 6 mm, in-plane resolution 1.5–1.7 mm, TR: 7000–7500 mseconds, TE: 50–60 mseconds) sequences were acquired in two stations, first from shoulder to elbow and then forearm to hand.
Two radiology residents and a board-certified radiologist analyzed MRI images using McKesson PACS and independently rated the affected and unaffected (“contralateral”) limb according to a previously established MRI Lymphedema Staging system, which was developed to gauge the presence and distribution of edema. 16 The readers were blinded to all clinical history. Majority consensus was used as the final MRI stage of the affected and contralateral arm.
ICG lymphoscintigraphy
Under sterile conditions, 0.05 cc of 0.625 mg/cc ICG (Patheon Italia SpA, Monza, Italy) solution with albumin was injected intradermally into the first and fourth web spaces, volar forearm, and the radial aspect of the elbow in bilateral upper extremities. Fluorescent images were captured using a near-infrared imaging system (Hammamatsu Photonics, Hammamatsu, Japan) and recorded in real time. Images were saved into an institutional clinical repository. Detection of any other pattern besides linear (e.g., splash, stardust, or diffuse) was considered abnormal and each abnormal ICG finding was given a numerical score according to the severity (linear: 0, splash: 1, stardust: 2, diffuse: 3).18,19
Lymphoscintigraphy
Any compression garments were removed for at least 48 hours before imaging. Tc-99m labeled tilmanocept or sulfur colloid were injected just proximal to the second and third web spaces of both upper extremities, with a total dose of ∼0.4 mCi. Large field of view detector with parallel hole collimators were used at 140 keV with a 20% window. Cobalt-57 was used for transmission images. Flow images were taken at 30 s/frame for 20 minutes. The presence of dermal back flow 20 and axillary lymph nodes were assessed on the static images that were acquired for 5 minutes at 1 hour and on delay images at 2 or 6 hours. Abnormal findings included the absence of tracer migration, lack of visualization of draining lymph nodes, or the presence of dermal backflow.
Statistical analysis
Wilcoxon signed rank-sum test was performed of the MRI stages between the affected and nonaffected arm of the same patient. Student's t-test or Fisher's exact test of the age, duration of symptoms before imaging, body mass index (BMI), and history of chemotherapy between patients with and without evidence of lymphedema in the contralateral arm were performed. Fisher's exact test was performed on the presence of dermal backflow or axillary lymph node in the affected versus unaffected contralateral arm. Interobserver agreement between the three readers on the assessment of the MRI Lymphedema Staging of the contralateral arm was calculated using Fleiss kappa. 21
Results
Eighty-five patients were imaged. One patient was excluded because of history of primary lymphedema and one was excluded for bilateral breast cancer surgeries. Five patients were excluded because STIR sequences were omitted in the MRI acquisition. Seventy-eight patients were included in the final analysis of the MRI of the contralateral arm. No intervention or symptoms were reported in the contralateral arm.
Interobserver agreement for MRI edema staging was 0.86 (0.79–0.94). Majority consensus was achieved in every case, that is, there were no cases where three different scores were recorded. Fourteen patients showed no edema in the affected arm (MRI Stage 0) (Table 1). Sixty-four patients (64/78, 82.1%) demonstrated at least MRI Stage 1 or higher in the affected arm (Table 1). 88.5% (69/78) patients demonstrated no edema in the contralateral arm (Fig. 1 and Table 1). Nine patients (9/78, 11.5%) demonstrated MRI Stage 1 edema in the contralateral arm (z = −6.955, p < 0.00001; Fig. 2 and 3; Table 1), with all also demonstrating MRI Stage 1 or greater in the affected arm. No stage higher than MRI Stage 1 was recorded for any of the contralateral arms, even across individual scores.
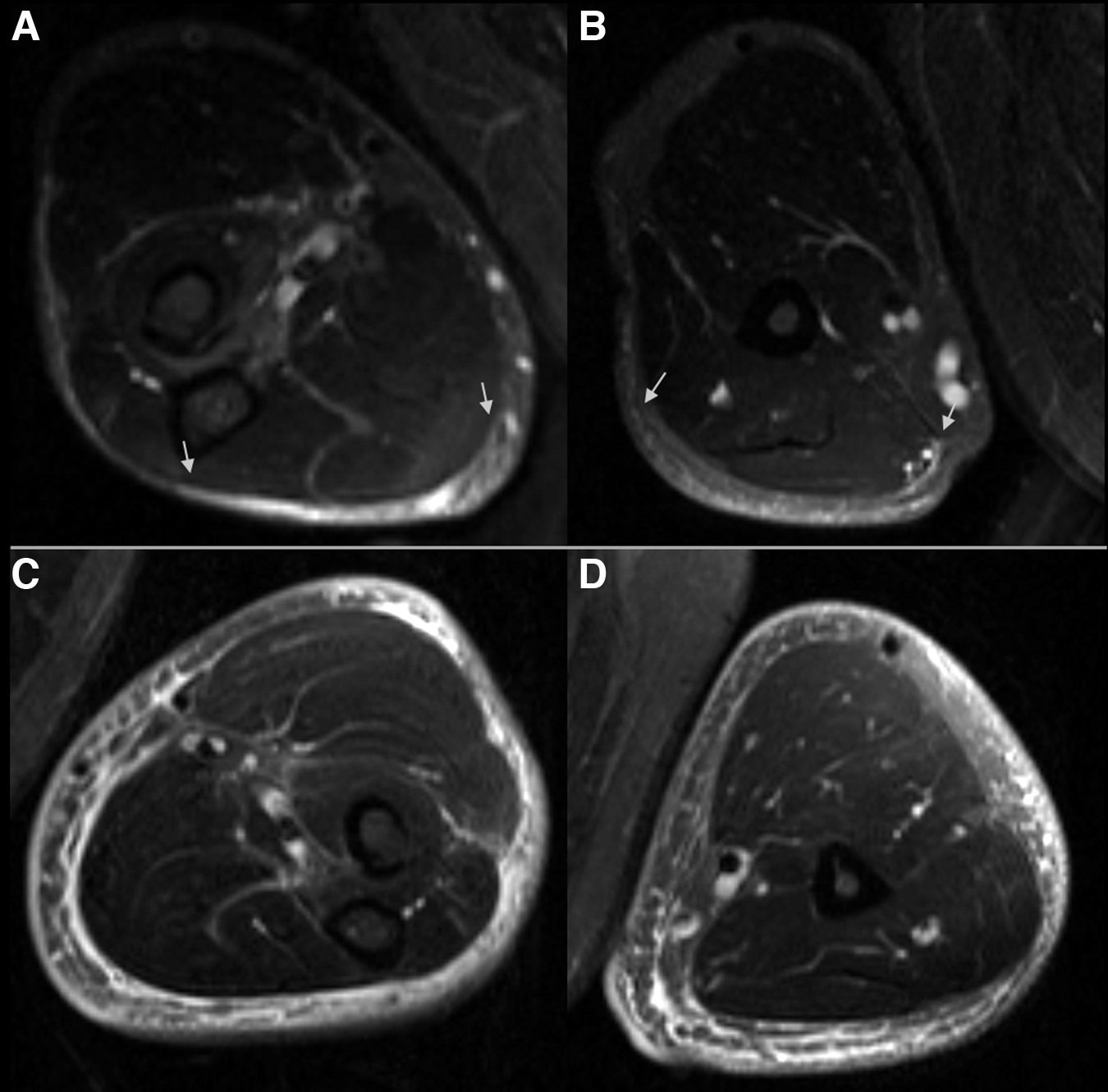
Forty-five year-old man with history of resection of a lipoma in the left axilla. Axial STIR MRI images demonstrate minimal edema (MRI Stage 1) in the forearm

Fifty-two year-old woman with history of left breast cancer, treated with breast conservation therapy, including axillary dissection and chemoradiation. Axial STIR MRI images demonstrate trace amount of edema in the unaffected contralateral right forearm
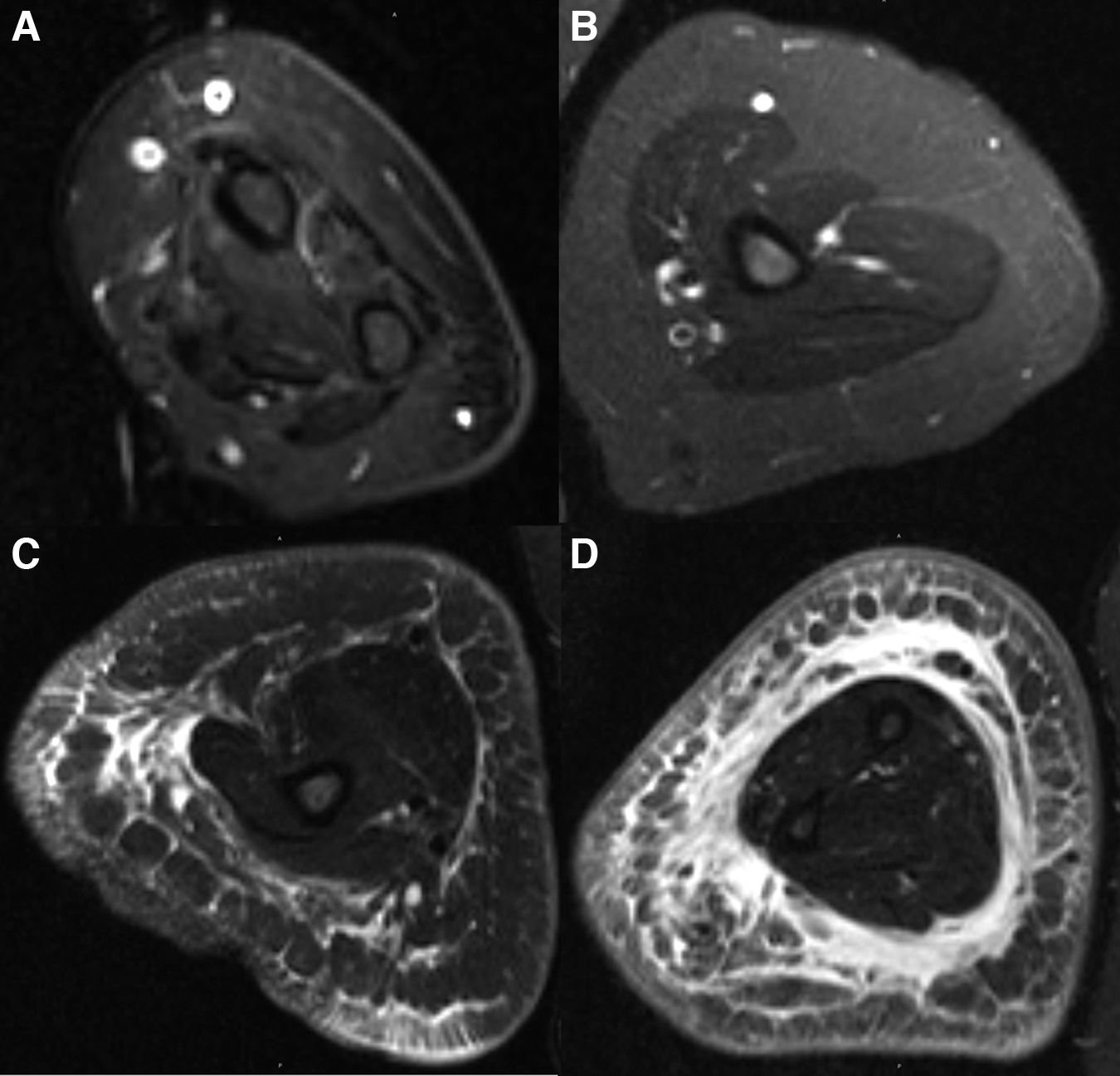
Fifty-seven year-old woman with history of right breast cancer, treated with mastectomy, axillary dissection, and chemoradiation. Axial STIR MRI images demonstrate no edema (MRI Stage 0) in the unaffected contralateral right forearm
MRI Stages of Symptomatic Limb Versus Contralateral Limb (n = 78)
z = −6.955, p < 0.00001.
The proportion of patients with edema in the contralateral arm was not significantly different when using the entire population of patients included in the study versus a narrowed cohort of patients with any imaging evidence of lymphedema in the affected arm (9/78, 11.5% vs. 9/64, 14.1% [X 2 = 0.20, p = 0.65]). Similarly, when the cohort of patients were narrowed to only those who were clinically diagnosed with lymphedema (n = 74), the rate of contralateral edema was 12.2% (9/74), which is not statistically different compared with the rate across the entire cohort (9/78, 11.5% vs. 9/74, 12.2% [X 2 = 0.02, p = 0.89]). There was no statistical difference in the age, duration of symptoms before MRI, BMI, or history of chemotherapy when comparing the patients who demonstrated asymptomatic edema versus those with no edema in the contralateral arm (all p > 0.3, Table 2).
Patient Demographics of Patients with (Non-Stage 0) and No (Stage 0) Evidence of Lymphedema
BMI, body mass index.
ICG lymphography was performed on 39 (39/78, 50%) patients. In those patients, the average ICG severity score was significantly higher than the contralateral unaffected limb (1.83 ± 0.96 vs. 0.04 ± 0.25, p < 0.00001) (Table 3). Only one (1/39, 2.6%) patient showed any abnormality in the contralateral unaffected limb; this was not statistically significantly different than the detection rate by MRI (X 2 = 2.62, p = 0.11), but in this single case the extremity did also exhibit mild (Stage 1) edema on MRI.
Comparison of the Indocyanine Green Lymphography Severity Scores Between the Symptomatic Versus the Contralateral Arm
z = −4.8554, p < 0.00001.
ICG, indocyanine green; SD, standard deviation.
Nuclear medicine lymphoscintigraphy of both arms was performed on 74 of the 78 patients included in the study (74/78, 94.9%). Within this cohort, 74.3% (55/74) of patients demonstrated an abnormal lymphoscintigraphy (64.9%, 48/74), whereas no lymphoscintigraphic abnormality was detected in the any of the contralateral arms (p < 0.00001) (Table 4). The MRI detection rate of edema within the contralateral arms was statistically significantly greater than that of lymphoscintigraphy (X 2 = 8.98, p = 0.003).
Comparison of the Presence of Abnormal Flow or Dermal Backflow on Lymphoscintigraphy in the Symptomatic Versus Contralateral Arm, and Rate of Abnormal MRI in the Symptomatic Versus Unaffected Arm in Patients with Normal Lymphoscintigraphy (n = 74)
Discussion
In this study, we found that the proportion of contralateral limb edema on MRI is 14.1% among patients who were confirmed by imaging to have secondary lymphedema in the affected limb. More importantly, contralateral limb edema was seen only in patients with imaging-proven lymphedema in the affected arm. Of those patients who showed evidence of edema within the contralateral limb, none were symptomatic or demonstrated an MRI Stage above 1, only one demonstrated any abnormality on ICG lymphography, and none had an abnormal finding on lymphoscintigraphy.
To our knowledge, this is the first study of the rate of contralateral upper extremity edema in patients with unilateral surgery-related secondary lymphedema who are otherwise healthy and without a history of primary lymphedema, suggesting that there may be an increased risk of underlying lymphatic dysfunction in these clinically asymptomatic limbs. Such studies have been performed for the lower extremity, where the rate of contralateral lymphedema in patients with unilateral lymphedema has been reported to be up to 32%–70%.22,23
Our study also highlights the potential utility of MRI in identifying patients with lymphedema, or at risk of lymphedema, who are not symptomatic. The fluid sensitive sequence that was used are readily available commercially and in fact, one of the sequences that are routinely used in body imaging. In addition, the grading of edema showed high interobserver agreement between the three observers, two of whom were residents who are not experts.
The clinical definition of lymphedema relies on comparisons between the affected and contralateral limbs, for example, a limb volume difference >200 mL2,24 or bioimpedance ratios exceeding a certain threshold, with the assumption that the contralateral arm is normal. 25 However, if there is preclinical lymphedema within the contralateral limb, these volume difference or bioimpedance ratios may falsely decrease the measured severity of lymphedema in either limb. Diagnostic tests such as MRI or ICG lymphography that evaluate each limb independently may thus be more accurate in staging.16,26
Every case of contralateral arm edema seen on MRI occurred in patients with imaging findings positive for lymphedema in the affected limb. The significant association between the presence of lymphedema in the affected limb and edema in the contralateral limb (p < 0.00001) suggests that MRI evidence of lymphedema in the affected arm is a risk factor for having edema and, therefore, potential lymphatic dysfunction in the contralateral arm. The severity of edema in the contralateral arm was no more than minimal (MRI Stage 1) regardless of the severity of the affected limb. This is expected as these patients did not exhibit any symptoms in the unaffected side, and none of the contralateral limbs were subjected to surgical intervention. Also expected was the absence of any detectable edema in the contralateral limb in patients who were ultimately found not to have lymphedema in the affected limb.
Although contralateral edema was detected in some patients on MRI, no abnormal lymphatic flow was detected in any contralateral arm with nuclear medicine lymphoscintigraphy, a difference that was statistically significant. Only one patient demonstrated any contralateral arm abnormality on ICG lymphography, which was not significantly different from the MRI detection rate due to a smaller cohort of patients who underwent lymphography, although this single case matched the MRI findings of mild edema. Even as MRI has either an equivalent or better detection rate for abnormalities in the contralateral limb in these patients, MRI also has the added advantages of avoiding use of any ionizing radiation, exogenous contrast agents, or invasive injections. Still, lymphoscintigraphy and ICG lymphography offer functional data that our MRI technique does not show, and their use may still be necessary, but MRI may be used first to select the patients who would require these additional studies.
No typical risk factors associated with secondary lymphedema were found to be associated with edema in the contralateral arm. Specifically, prior studies have shown that the risk of lymphedema in the treated arm increases with age, BMI, and chemotherapy.27–31 However, the same risk factors were not correlated with the edema of the contralateral arm. This suggests that there may be an underlying mechanism that predisposes a patient to developing lymphatic dysfunction in the contralateral limb, and further research is needed in this area.
There are several limitations of this study. First, the study is a retrospective review of the imaging, which lacks the ability to determine a causal relationship between the lymphedema in the affected arm and the contralateral arm. Because the study was conducted at a single academic center, the results may not be generalizable to community practices. ICG lymphography was performed in only 50% of patients. Although there may be selection bias, this represents a clinically relevant cohort who needed further evaluation before surgical intervention or conservative treatment. Finally, we did not compare our results against the rate of upper extremity edema in a healthy cohort, as this was beyond the scope of this retrospective study.
In conclusion, we found that the rate of contralateral arm edema was 14.1% in patients with unilateral secondary lymphedema of the arm on MRI. When it does occur, the edema tends to be mild (no more than MRI Stage 1) and may not show functional abnormality on the lymphoscintigraphy or ICG lymphography. No risk factors for contralateral edema were identified in our study. Although low in prevalence, edema of the asymptomatic contralateral arm does occur and full evaluation should be performed for accurate staging and management.
Footnotes
Authors' Contributions
Conceptualization, data curation (lead), formal analysis (lead), investigation, methodology, writing (lead), review, and editing (equal) by G.K. Data curation (equal), writing (supporting), review, and editing (equal) by M.A. Methodology (equal), resources, review, and editing (equal) by M.P.S. Conceptualization (equal), resources, review, and editing (equal) by D.S. Conceptualization (equal), supervision (lead), methodology (supporting), review, and editing (lead) by L.L.T.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
G.K. is supported by the RSNA Research Grant RR1820. None of the other authors has a financial interest in any of the products, devices, or drugs mentioned in this article.