
Abstract
Lymphatic circulation, a one-way channel system independent of blood circulation, collects interstitial fluid in a blind-end way. Existing widely in various organs and tissues, lymphatic vessels play important roles in maintaining tissue fluid homeostasis, regulating immune function, and promoting lipid transport. Recent studies have shown clear evidence that lymphangiogenesis has a strong mutual effect on coronary atherosclerosis (AS). In this study, we focus on this topic, especially in the aspects of relevant ligand/receptor, inflammation, and adipose metabolism. For the moment, however, the role of lymphangiogenesis and remodeling in coronary AS still remains controversial. The studies of our group and accumulating published evidence show that the pathological remodeling of lymphatic vessels in coronary AS may have a negative effect, but normal functional lymphangiogenesis is probably beneficial to the regression of coronary AS. Thus, the conclusion of this review is that lymphatic vessel function rather than its quantity determines its influence in AS, which needs more evidence to support.
Introduction
Cardiovascular disease (CVD) is a major disease endangering the global population. Recent data have shown that the prevalence of CVD among adults (over 20 years old) is reaching 48.0%, and is growing among young people.1,2 Coronary atherosclerosis (AS) is considered to be one of the most important pathological bases of chronic CVD. AS starts from the inflammatory reaction caused by the injury of the intima, and develops into progressive plaques. The plaques finally block or fall off the artery, causing acute or even life-threatening events like myocardial infarction (MI). The pathogenesis of AS has been widely studied, but the mechanism is still unclear.
Inflammation induced by a bacterial pathogen, immunization in the presence of complete Freund's adjuvant, and contact sensitization have been shown to promote the growth of lymphatic vessels from the preexisting ones, and this process is named lymphangiogenesis. 3 Particularly, as a channel of innate immune transport and lipid absorption, the lymphatic vessel system is closely related to a variety of diseases with chronic inflammation and abnormal lipid metabolism, such as AS.
In this review, we summarize the major ligands/receptors inducing lymphangiogenesis, immune cells in the chronic inflammatory microenvironment of AS. Meanwhile, we conclude the mutual effect between lymphangiogenesis and AS, and try to explain the influence through the role of lymphangiogenesis in promoting lipid transportation.
Structures and Functions of Cardiac Lymphatic System
Structures
In 1653, Olaus Rüdbeckin first demonstrated cardiac lymphatics, followed by the works of other researchers in the following 250 years.4–6 Through these remarkable works, now we can draw a detailed model of the whole system (Fig. 1a). The lymphatic capillaries lined with unilateral lymphatic oak leaf-shaped button-like endothelial cells (LECs) with bare or discontinuous basement membranes originating from different parts of the heart collect lymph passively from endocardium to epicardium, merge and integrate corresponding precollectors, and then extend into the collecting vessels (Fig. 1b).
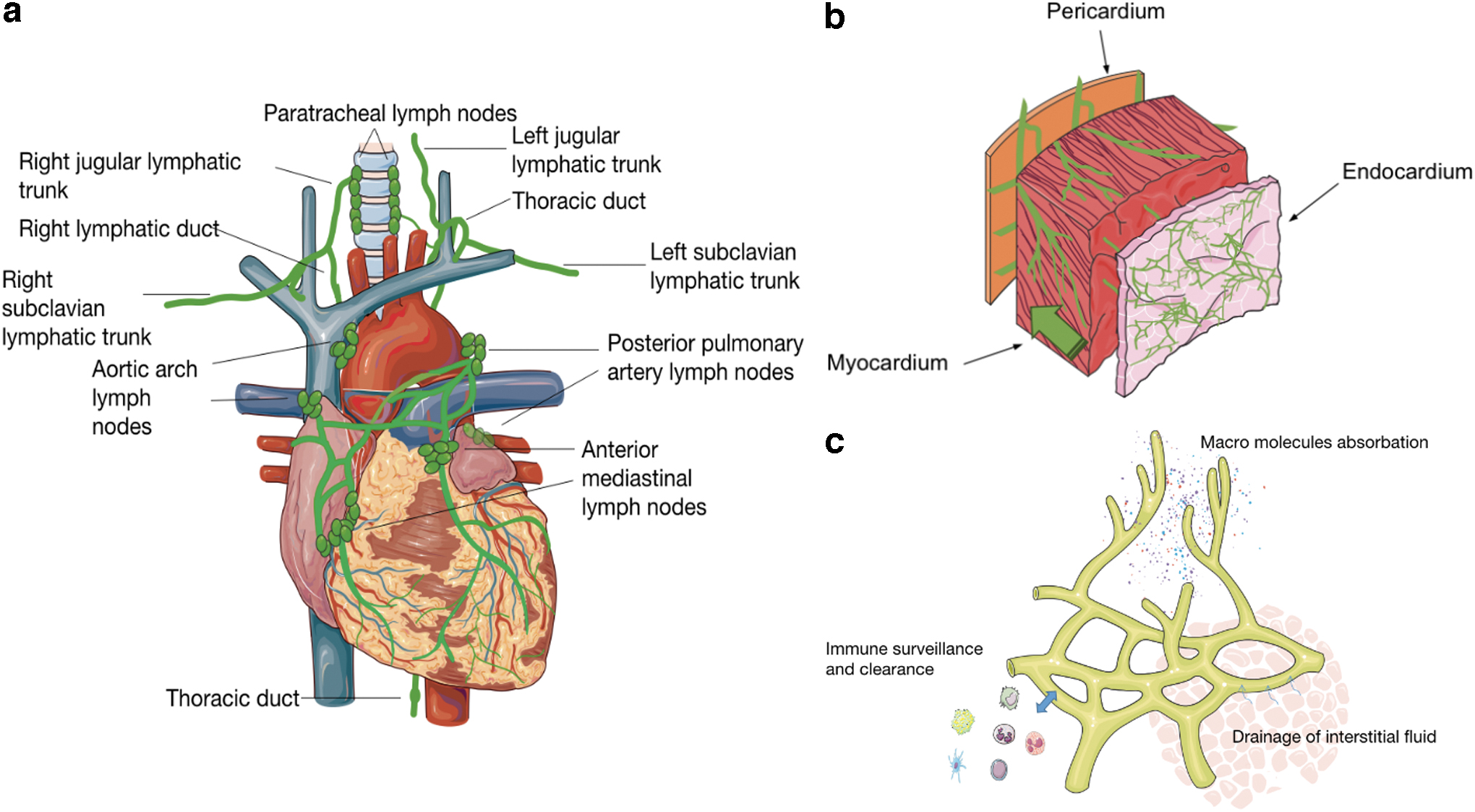
Structure and functions of Cardiac lymphatic vessels.
Lymph is actively conveyed to the lymph nodes (LNs), where the immune cells are gathered, activated, and stayed (lymphocyte homing). The lymph, consisting of interstitial fluid (ISF), immune cells, and macromolecules such as high density lipoprotein (HDL), flows into the thoracic duct and the right lymphatic duct, then is injected into the left and right venous angle, and eventually spills out back into the blood circulation.
Functions
The basic functions of human lymphatic vasculature are intestinal fat absorption, unidirectional drainage of ISF, and tissue immune surveillance (antigen clearance, inflammatory resolution, etc.), which associates the lymphatic vasculature with lipid metabolism and immune-related diseases (Fig. 1c). Besides, the lymphatic vessel has specific characteristics that are dependent on the unique local microenvironments of distinct organs,7,8 suggesting its strong plasticity and functional adaptability and its varied roles in different stages of diseases in various systems.
Factors Related to Lymphangiogenesis in AS
Major factors with clarified effects of lymphangiogenesis in AS
Vascular endothelial growth factor-C/D and vascular endothelial growth factor receptor–3
Receptor tyrosine kinase vascular endothelial growth factor (VEGF) receptor–3 (VEGFR-3) is widely expressed on the surface of lymphatic endothelial cells. VEGFR-3, along with its main secreted ligand, VEGF-C, is regarded as a most vital driver of lymphangiogenesis,9,10 while VEGF-D, another known ligand of VEGFR-3, can only produce the partial effect of VEGF-C. 11 The hydrolyzed VEGF-C can be converted to an active form and then bind to VEGFR-3, which promotes the development of lymphatic vessels with the participation of extracellular protein collagen and calcium-binding EGF domain-containing protein 1 (CCBE1), the disintegrin-like, and metalloprotease with thrombospondin type 1 motif, 3 (ADAMTS3).12,13
VEGF-D can also induce lymphangiogenesis in inflammatory conditions through another proteolytic pathway. 14 Most of these signals are active during embryonic development but significantly decreased after adulthood, but in some pathological conditions (like tumor and AS), those pathways can be reactivated. 15 Notably, in embryonic development, cardiac lymphatic vessels are mainly transdifferentiated from venous precursors, 16 whereas there are a few parts considered to be formed independently of venous sprouting 17 as well. VEGF-C/VEGFR-3 pathway is involved in lymphangiogenesis of both physiological embryonic development and pathological reactivation.
The overexpression of VEGF-C/VEGFR-3 mediated by various factors is the central mechanism underlying lymphangiogenesis. 18 For example, with the action of VEGF-C/VEGFR-3, the accumulated water between tissues increases the tension in the tissues, thus activating integrin β1 on LEC and promoting the LEC proliferation.19,20 Lymphangiogenesis induced by VEGF-C/D and VEGFR-3 pathway also contributes to increased inflammation and decreased oxygen or nutrition supply, which are considered as the most common adaptive regulations for the body to adapt to the pathological changes of lymphatic functions. 21
Secreted CCBE1 and disintegrin-like and metalloprotease with thrombospondin type 1 motif, 3 (ADAMTS3)
CCBE1, a secreted protein composed of 2 EGF domains and 2 collagen repeats, 22 has been identified in animal models during early cardiac development, and the knockdown of it can lead to cardiac developmental defects.23,24 In the dermis, the key role of CCBE1 related to VEGF-C/VEGFR-3 in the lymphatic development of LECs and embryonic progenitor cells has been reported.10,25–27 Some studies have pointed out that it also affects the budding of vein deriving from lymphatic endothelial cells. 26 A large number of studies have revealed that CCBE1 promotes lymphangiogenesis by synergizing and enhancing VEGF-C signal and VEGFR-3 quantity on LEC surface.26,28–30 This process is mainly realized by the formation of a complex with ADAMTS3 (ADAMTS14 probably participates in).14,31
Interestingly, in several cancer studies, CCBE1 was negatively correlated with tumor progression (CCBE1 level decreasing in tumor occurrence area, and downregulated in patients with LN metastasis), which contradicted the conclusion that CCBE1 overexpression promoted lymphangiogenesis in normal tissues.32,33 The mechanism determining the phenotypic difference of CCBE1 between tumor and normal cells deserves further exploration. The role of CCBE1 in atherosclerotic region is rarely investigated. But the role of CCBE1 as an important hydrolytic element of VEGF-C needs detailed burrowing.
VEGF-A and VEGFR-2
At the end of the last century, the interaction between VEGFs and VEGFRs to promote lymphangiogenesis has been confirmed.34–37 VEGF-A and VEGFR-2 play a regulatory role in the development of lymphangiogenesis, such as inducing abnormal lymphangiogenesis 38 However, VEGF-A/VEGFR-2 is considered as a minor pathway that cannot replace the major function of VEGF-C and VEGFR-3. 39 Meanwhile, VEGFR-2 also receives the signal of VEGF-C. In the atherosclerotic vascular area, soluble VEGFR-2 may competitively bind to VEGF-C in the stroma, thereby inhibiting the formation of peripheral lymphatic vessels and accelerating the progression of AS. 30 The role of this essential molecule in embryonic development and lymphangiogenesis of plaque area is intriguing.
SRY-related HMG-box 18 and prospero homeobox protein 1
SRY-related HMG-box 18 (SOX18) is an important transcription factor in the development of cardiovascular and lymphatic vessels during embryonic development and AS. 40 As a sufficient and necessary transcription factor to promote lymphangiogenesis, prospero homeobox protein 1 (PROX-1) is regulated by upstream SOX18 transcription factor, 41 an important marker of the lymphatic vessel and a key switch of lymphatic vessel development. The loss of PROX-1 can cause lymphedema, which may lead to abnormal accumulation of fat and subsequent obesity (an important risk factor of AS). 42 Epicardial fat accumulation provides a good inflammatory environment for lymphangiogenesis. At the same time, abnormal development and expression of lymphangiogenesis also promote epicardial fat accumulation. 43 Besides, PROX-1 can be used as a marker of lymphangiogenesis.
CCR7
CCR7 is the receptor of chemokine ligands CCL19 and CCL21 expressed on a variety of immune cells. 44 CCR7 participates in lymphocyte transport and LN homing.45,46 It plays multiple roles related to the inflammatory response in AS, such as mediating immune cell trafficking46,47 and activating specific leukocytes, 48 and it is also involved in lymphangiogenesis.49,50 There is evidence that intervention against CCR7 may promote the regression of AS, 51 suggesting it as a promising drug target.
Sphingosine 1-phosphate
Sphingosine 1-phosphate (S1P) burdens key functions in the immune and cardiovascular systems. 52 S1P can affect lymphangiogenesis through a specific pathway. 53 After the deletion of Sphk1 (in which case S1P is no longer expressed in lymph, but still expressed in plasma) in mice, the development of lymphatic capillaries and the cell/cell junctions is impaired. 54 Some studies have proved that S1P protects against AS,55–57 but a few studies believe that it can also promote AS. 58 The disparity may be caused by the different roles of S1P in different target organs, such as cardiac lymphatic vessels and intestinal lymphatic vessels. The relationship between S1P bioavailability and HDL indicates its potential vital connection with lipid metabolism.59–62
Prospective factors of lymphangiogenesis in AS
Podoplanin
Podoplanin, expressed in many cells or tissues, such as many carcinomas and aortic atherosclerotic lesions, is a sialomucin-like single transmembrane glycoprotein consisting of a short cytoplasmic domain and an extracellular domain glycoprotein.63,64
The combination of C-type lectin-like receptor 2 (CLEC-2) and podoplanin during early lymphatic development promotes the separation of blood vessels and lymphatic vessels, 65 which is of decisive significance for the early separation of lymphatic vessels from venous endothelial cells. The combination of CLEC-2 on the surface of platelets and podoplanin on the surface of cancer cells can induce platelet aggregation and promote hematogenous metastasis of tumor cells. 66 Endothelial injury in AS progression may lead to thrombosis and produce many inflammatory factors, resulting in the upregulation of podoplanin expression on the surface of endothelial cells and macrophages in the plaque area.
Podoplanin on the surface of LECs is also regulated by nuclear transcription factor PROX-1. Yet, whether the inflammatory microenvironment in the atherosclerotic region will induce its overexpression on the LECs transdifferentiated from macrophages remains to be confirmed, which may be one mechanism of lymphatic proliferation in AS.
LYVE-1
LYVE-1, a specific marker of lymphatic vessel structure, is widely used to distinguish lymphatic vessels from blood vessels, although it seems not essential for the development and maturation of the lymphatic vessel system. 67 It is expressed on the surface of lymphocytes and participates in the uptake of interstitial hyaluronic acid. Importantly, it is related to the migration of leukocytes into lymphatic vessels68–70 by combining with CD44 expressed on the cells. 69 So it may play an important role in the immune clearance in plaque regression.
EphrinB2/EphB4
Human ephrinB2 is encoded by the transmembrane protein EFNB2 gene. EphrinB2 has a transmembrane domain, an extracellular receptor-binding domain (RBD), and an intracellular PDZ domain. The increased expression of EphinB2 in monocytes can increase the adhesion between monocytes and endothelial cells, and promote the development of plaque. 71 EphrinB2/EphB4 plays an important role in angiogenesis, 72 and its role in lymphangiogenesis has been found in recent years. It may enhance the expression of VEGFR-3 73 as it does in angiogenesis.74,75 In addition, it may interact with a variety of cytokines, 72 but with limited published evidence. EphrinB2/EphB4 pathway is characterized by a two-way signal transduction, so there may exist more complex regulatory mechanisms.
EphrinB2/EphB4 is also found to be distributed in a variety of immune cells, lymphatic endothelial cells, parietal cells, and arteriovenous endothelial cells, despite the differences in the distribution of different subsets. The role of lymphatic vessels in the AS-related inflammatory environment is still unknown, for example, the gene and molecular mechanism behind the upregulation of EphB2, EphB4, ephrin-B1, and ephrin-B2 during AS, which needs further elucidation.
Angiopoietins and TIEs
There are four subtypes of angiopoietins (ANGs), which can interact with TIE2 on the surface of LECs and induce LEC phosphorylation, thereby promoting the germination and growth of lymphatic vessels.74,76 Studies have shown that the embryonic heart of mice with deletion of ANG2 subtype develops well, but with lymphatic dysplasia, chylous ascites, and lymphedema. 77 ANG1 can be produced by smooth muscle cells (SMCs) and fibroblasts, therefore, it may affect lymphatic vessels around the plaque by the paracrine way. ANG2 is mainly produced by ECs. 76 The rise of ANG2 is found in perivascular adipose tissue (PVAT) around the plaque, 43 which contributes to inflammation and fibrosis and may promote lymphangiogenesis.
Semaphorins and neuropilins
Semaphorins (SEMAS), the ligands of neuropilins (NRPs), play an important role in AS. 78 NRP2 can promote lymphangiogenesis independently or by forming a coreceptor with VEGFR-3 and accepting VEGF-C/D binding, 79 whereas NRP1 combines with VEGFR-2 by accepting VEGF-A. 80 There is a broader interaction between NRPs and VEGFs. 81 In addition, NRPs are associated with lymphangiogenesis, and abnormal smooth muscle attachment occurs in the lymphangiogenesis region of NRP1.82–84 NRP2 deficiency in embryos does not seem to affect the development of large lymphatic vessels in the cardiac vascular system, but it suppresses the formation of small lymphatic vessels and lymphatic capillaries. 85 The mechanisms underlying the actions of these molecules in the atherosclerotic region remain to be studied.
FGF2
The FGF family consists of 23 members that regulate a variety of biological functions in different tissues. FGF2 can act by directly binding with FGFR1 in LECs, 86 or by stimulating the expression of VEGF-C in vascular endothelial cells and SMCs. 87 LVFE-1 can also bind to it to promote FGF2-induced signal binding and promote lymphangiogenesis. The role of FGF2 in the lesion area of AS needs to be further revealed.
BMP9/10 and activin receptor-like 1
BMP9 and its receptor, activin receptor-like 1 (ALK1), belong to the TGF-β superfamily. In mice, ALK1 block can reduce lymphatic vessel density. 88 The decrease of BMP9 is related to the decreased formation of lymphatic valve 88 through regulating relevant genes. 89 BMP10 is a ligand specially expressed in hearts. BMP10-knockout mice die during development as a result of cardiac defects before lymphatic development. 23 Therefore, it is a challenge to evaluate its specific effect on cardiac lymphangiogenesis, and more studies are needed to explain its specific role in AS.
FAT4
Recently, an interesting study has revealed the role of FAT4 (a typical cadherin) in LECs and demonstrated the effect of FAT4 in coordinating LEC polarity in response to blood flow. 90 This finding may provide new insight into lymphangiogenesis caused by hemodynamic changes in the endothelial injury stage of AS. Yet the mechanism is not clear.
A recent study has shown that RSPO2 inhibits lymphangiogenesis by acting on LGR4 on the surface of LECs, and explored its possible downstream Akt-eNOS-NO pathway. 91
Relevant Immune Cells in AS
The number and function of lymphatic vessels, as the channel of immune cells, determine the inflow and outflow of immune cells, thus affecting the function of these cells. Meanwhile, the biological molecules secreted by immune cells can induce or inhibit the formation of lymphatic vessels.
Macrophages/monocytes
Macrophages play a central role in the whole process of AS. 92 Triggered by the causative factors of AS (such as endothelial injury), impaired endothelium cells release the inflammatory signals and then collect plenty of circulating monocytes from the blood. These monocytes are then transformed into macrophages with suppressed ability of migration and thus stick in the damaged area. Due to different local microenvironment factors (like toll-like receptor ligands or interferons for M1/IL-4 or IL-13 for M2),93–95 through polarization into distinct phenotypes (such as M1, M2, Mox, M4, etc.),94,96 these macrophages not only promote inflammation and cholesterol accumulation, making the plaque unstable and prone to rupture, but also induce plaque regression and stability. 97
Lymphangiogenesis is not only the target of macrophages, but also the channel of trafficking macrophages and other immune cells, which can reduce the local immune activity and cholesterol content. 98 Macrophages promote or inhibit lymphangiogenesis by secreting factors in paracrine ways. Also, macrophages and some soluble antigens in plaques can be transported to the downstream LNs through lymphatic vessels and reactivated in LNs to stimulate further amplified inflammatory response, 6 indicating their complicated functions in immune reactions.
Dendritic cells
Dendritic cells (DCs) are classified into conventional or classical DCs or plasmacytoid DCs according to their functions, and more subsets are defined based on their specific markers. 99 Although the main biological function of DCs is to present antigen and participate in specific immune response, DCs can also secrete proinflammatory factors, such as VEGF-C, FGF2, NRP1, to promote lymphangiogenesis.100–102 In terms of adaptive immunity, DCs can not only upregulate the immune response of NK cells and T cells and the expansion of Th1 cells by secreting IL-12, 103 but also induce the proliferation of Treg cells, thus mediating immune tolerance and immune regulation. 104 DCs can even absorb lipids, like macrophages, to form the core of plaque. 105
T lymphatic cell
Thymus-derived T lymphocytes play a proinflammatory role in AS formation, 106 and Th1 cells are likely to be the main undertakers. A recent study has shown that surgical destruction of the lymphatic vessels around the aorta can cause the accumulation of T cells in the adventitia and aggravate the AS lesions. 107 Therefore, the lymphatic pathway in the adventitia may be a channel for early T cell clearance. However, the rise of Treg cells in response to the decreased peripheral blood lipid level has been proved to be essential in AS regression. 108
B lymphatic cell
Although the mechanism has not yet been elucidated, the role of humoral immunity mediated by B lymphocytes is clear in AS. Immunoglobulin,109–111 which targets multiple epitopes of oxidized low density lipoprotein, has been found in plaque and plasma of mice and humans. However, the protective inhibitory effect of B cells on AS has been proved in B cell-deficient ApoE−/− mice.112,113 Like T cells, B cell subsets may play contradictory roles in AS progression. It is worth mentioning that the “tertiary” lymphoid organizations consisting of clonally expanding B cell folds, T cell complexes, and high endogenous veins can be found at AS sites.114,115 B cells are likely to be important mediators of this derivative reaction.116,117
In general, the activation of immune cells promotes plaque enlargement and vulnerability. The migration of these immune cells from plaque is an important feature of plaque regression, which is mainly achieved through lymphatic vessels, including the transmembrane pathway. The completion of this process is based on the number and function of lymphatic vessels. It seems that the specific induction, retention, or elimination of the main culprit immune cells in different stages of AS can provide novel insights into AS treatment: to block the progression of plaque and promote its regression.
Innate immunity plays a central role in lymphangiogenesis, but adaptive immunity is equally important, although the mechanisms have not been well revealed due to the late start of research on cardiac lymphangiogenesis. Although the role of lymphangiogenesis in AS remains controversial, further understanding of the crosstalk among those complicated molecules in distinguished pathological stages of AS will benefit the treatment strategies (Fig. 2).
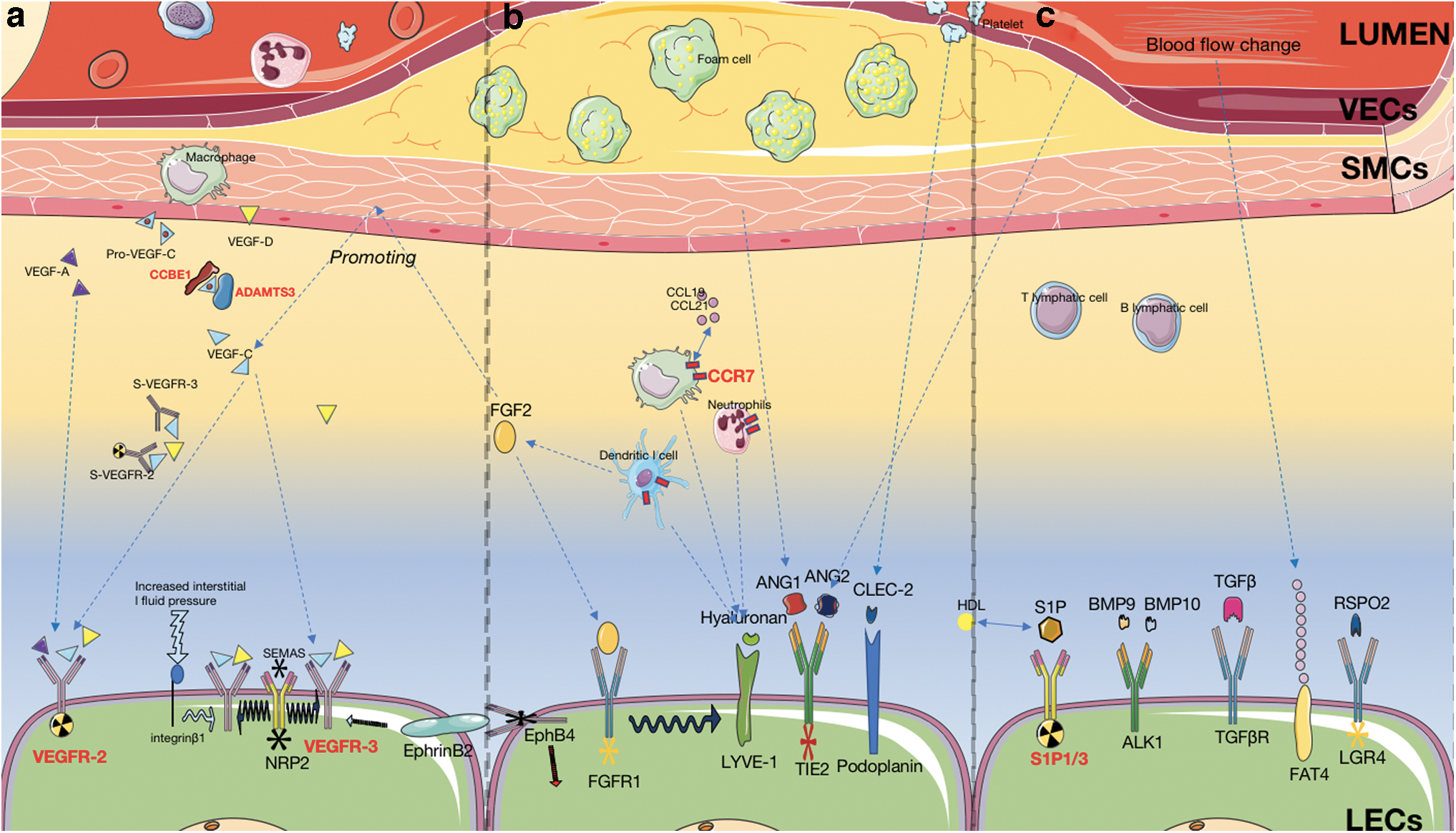
Lymphangiogenesis signals in atherosclerotic plaque area.
The Role of Lymphangiogenesis in AS
AS is a chronic inflammatory disease 118 with autoimmune characteristics. 119 The mobilizing inflammatory cells directly participate in the formation of AS plaque necrotic core, increase circulating inflammatory factors, and continuously amplify inflammatory signals through cascade reaction to aggravate the disease.
Lymphatic vessels at sites of AS plaques derive from the adventitia of arteries adjacent to small blood vessels, which is associated with local inflammation and lipid accumulation.107,120–123 A number of lymphokines deriving from foam cells, vascular smooth muscle cells, and circulating blood produce signals that act on receptors on the surface of LECs to promote lymphangiogenesis. 114 Research evidence shows that the increase of lymphatic vessels in plaque and adventitia, and the abnormal expression of related signal molecules appear in the early stage of atherosclerotic plaque formation.107,124 However, whether increased lymphatic vessels promote plaque progression or regression remains controversial.
The increase of lymphatic vessels is conducive to edema regression and inflammation clearance
At present, the mainstream view is that in progressive AS, the increased lymphatic vessels delay the process of AS through alleviating perfusion and edema, promoting inflammatory factor efflux and cholesterol reversion. For example, Taher et al. observed atherosclerotic ApoE−/− mice and found that despite the elevated expression of VEGF-C in aorta, the lymphatic vessels in adventitia degenerated, suggesting that the degenerated lymphatic vessels promoted the progression of plaque. 30 This study also suggested that the increased soluble VEGFR-2 might competitively bind to VEGFR-2/3 on LEC surface to inhibit the formation of lymphatic vessels. Yeo et al., through a new measurement method, observed lymphatic vessel damage in AS, which affected the outward transport of inflammation-related macromolecules.
Ezetimibe can improve lymphatic vessel function and promote plaque regression. Lymphatic ligation also promotes plaque progression, confirming the therapeutic effect of lymphatic drainage on AS. 125 The effect of Ezetimibe suggests that promoting cholesterol efflux may be particularly a critical function of lymphangiogenesis. When using lymphangiogenic agents or enhancing the signal intensity of the pathway to promote lymphangiogenesis, AS was alleviated in most experiments.91,126–128 Correspondingly, the application of lymphangiogenic inhibitors showed more AS-promoted phenotypes.55,129
The abovementioned studies provide convincing evidence that lymphangiogenesis can inhibit AS progression and promote AS regression. Also, in the early studies, Eliska et al. failed to find lymphatic vessels in the endocardium, media, or adventitia of either normal people or AS patients. 130 However, in some specific areas, such as the adventitia of intramural arteries with abundant lymphatic drainages, it seems that arteriosclerosis rarely occurs. 131 These findings suggest that abundant cardiac lymphatic system contributes to the alleviation and regression of AS. However, recent studies have proved that lymphangiogenesis is common in adventitia, whether in healthy people or AS patients. 6
Increased lymphatic vessels amplify the inflammatory response and increase plaque inflammation
Lymphangiodysplasia in the heart of patients with coronary heart disease is characterized by increased quantity and disordered structures. 121 Inflammation triggers the proliferation of lymphatic vessels, which then overactivates the immune expression around the plaque and stimulates a more complex immune response, resulting in the circulation accumulation of macrophages, and proinflammatory cytokines such as IL-2 and IL-6. As a result, the plaque volume and instability are increased.
This mechanism is supported by experimental data. For example, Kholová et al. found proliferative lymphatics in AS valve, infective endocarditis, as well as acute and chronic ischemic and inflammatory heart regions, proving that the progress of heart inflammation is accompanied by the proliferation of lymphatics, which then aggravates the disease. 121 In an earlier study, Drozdz et al. found a wide distribution of lymphatic vessels in the adventitia of patients with carotid AS, and the degree of lesion (intimal thickness) was positively correlated with the increased number of adventitial lymphatic vessels. 132 They observed consistent results in the adventitia of patients with abdominal aortic AS. 133
The drug research of our group showed that the area of lymphatic vessels and aortic plaques decreased simultaneously in ApoE−/− mice, supporting that excessive lymphangiogenesis promoted AS. 134 Path and colleagues proposed “Inflammatory amplification by circulation” theory, which states that, immune cells drained to LNs through lymphatic vessels might be reactivated, and then return to lymphatic vessels to form plaque.135,136
In addition, DCs and macrophages that sense antigen signal may also act as antigen-presenting cells to activate T lymphocytes and B lymphocytes in LNs, causing adaptive immunity and further aggravating the severity and instability of AS.
Extracardiac evidence also supports the manifestation of LNs in inflammatory/autoimmune disease cases. For example, in the cases of heart or artery transplantation, lymphangiogenesis inhibition can reduce immune rejection, but has no effect on normal tissues.137–139 The inhibition of lymphangiogenesis in adaptive immunity may be attributed to its ability to reduce VEGFR-3-mediated CCL21-related immune cell efflux, thus weakening the activation of immune cells in secondary lymphoid tissues.
However, in Crohn's disease, an autoimmune disease, lymphatic vessel damage is a key factor of fat accumulation, intestinal edema, and chronic inflammation. 140 Likewise, in some skin inflammation cases, promoting the proliferation of lymphatic vessels has been proved conducive to the elimination of inflammatory cells and factors. VEGF-C/D upregulation seems to be an adaptive performance of the body to eliminate inflammation and restore homeostasis.141,142
Therefore, most existing evidence points to the negative role of lymphatic vessels in adaptive immunity (promoting adaptive immune activation) and the positive role of innate immunity (clearing immune signal and restoring homeostasis), but the conclusions in different conditions are still contradictory.
Lymphatic vessels as “drainage tube” in the recovery from MI
MI is one of the most common acute cardiovascular events in AS. Cardiac diffuse edema caused by tissue fluid accumulation after MI has a significant impact on the prognosis. 143 The positive function of lymphangiogenesis in cardiac lymphangioma related to MI seems to be clear. 17 The tissue drainage function of lymphangiogenesis can reduce cardiac edema, and therefore improve the impaired heart function. Excessive ISF produced by arterial occlusion and myocardial cell necrosis impairs heart function.
LECs are likely to sense this change through β1 integrin receptor and upregulate the expression of VEGFR-2/3 to produce more lymphatic vessels, so as to remove the burden of the heart by reducing high ISF pressure.19,20 LECs have been found to secrete reelin, a lymphoangiocrine signal, to promote the early development of neonatal myocardial cells and repair after myocardial injury, indicating that proliferative lymphatic vessels enhance not only the drainage but also myocardial recovery. This finding offers a new important research direction. 144
Lymphangiogenesis and Adipose Metabolism
Lipid accumulation, an important pathological mechanism of AS, 145 is usually caused by a high-fat diet and disordered lipid metabolism. Abnormal intestinal lipid absorption and perivascular fat inflammation seem to promote the risk of AS progression, whereas reverse cholesterol transport (RCT) is more conducive to decrease it.146,147 The crosstalk between lymphangiogenesis and adipose metabolism is a promising target for AS prevention and treatment.
Relationship between intestinal lymphatic adipose absorption and AS
In the early stage of human development, the lacteals (intestinal lymphatic vessels) grow into small intestinal villi, which promotes the absorption of chylomicrons into the lymphatic system through the intestine,148,149 and then participation in the blood circulation to provide materials and energy for the growth and development of the body. In adulthood, the body needs less lipid, but the lymphatic vessels do not degenerate and decrease. 150 Coupled with the high-fat diet, overabsorbed cholesterol and triglycerides become the source of AS.
VEGF-C/VEGFR-3 has been shown to directly regulate the proliferation of the intestinal chylous duct. The upregulated VEGF-C/VEGFR-3 pathway can lead to excessive intrinsic lymphatic vessels. Correspondingly, fewer lymphatic vessels in small intestines have been proved to protect mice from high lipid intake. 11 The downstream Dll4/Notch pathway mediated by VEGFR-2/3 is responsible for the continuous regeneration of lymphatic vessels. 150 Notably, VEGF-C/VEGFR-3-targeted drugs for obesity and hyperlipidemia, which are in phase I clinical trials, 151 may become a new strategy for lipid metabolism management in the future. Pannexin-1 (Panx-1), a transmembrane protein, can promote RCT through upregulating lymphangiogenesis. 152 Interestingly, conditional knockout of Panx in macrophages and endothelial cells promotes atherosclerotic phenotype because of the lack of lymphangiogenesis. However, ubiquitous Panx deletion demonstrated an opposite result. 153 The reason is that the latter reduces the production of intestinal lymphatic vessels and the absorption of intestine-derived fat at the same time, showing that lymphatic vessels can play an antagonistic role in different organs. The interaction of gut microflora with lacteals will become an important research direction and provide constructive guidance for improving treatment and management strategies of AS. 154
Lymphangiogenesis and RCT
HDL-mediated cholesterol and macrophage efflux is a key mechanism in AS plaque regression. Cholesterol particles in plaque-loaded macrophages are carried out by HDL through ATP-binding cassette transporters ABCA1 and ABCG1 and transported to the lymphatic vessels around the plaque, 155 then circularly transported to the liver, and transformed into bile acid excretion through SR-BI receptor. The concentration of HDL in lymph is 30% higher than that in blood, indicating the key role of lymphatic vessels in loading RCT.156,157 Lim et al. and Martel and colleagues have discovered that the function of RCT is significantly reduced in the mouse model with blocked lymphangiogenesis atherosclerotic aortas.124,126
However, some studies have also shown that it could not exert the expected antiatherosclerotic effect by lymphatic vessels, 158 which may be caused by some unknown mechanisms of RCT (such as the mechanism of HDL outflow from the arterial media). Therefore, the increase of HDL or lymphatic vessels may be a necessary but insufficient condition for strengthening RCT. Another key mechanism is to remove the speed-limiting mechanism of HDL in the transmembrane process. Obviously, the research of lymphatic vessels in RCT is very insufficient.
Peripheral adipose and lymphangiogenesis
Epicardial adipose tissue (EAT) and PVAT are the most closely related fatty groups of heart and coronary artery in mediastinal adipose tissues. 158 Reactive oxygen species and inflammatory factors in the mediastinal adipose tissue increase with age or inflammatory conditions of AS.43,159
Anatomically, EAT is mainly distributed in the coronary artery, and it receives coronary perfusion like myocardial tissues. The arteriovenous branches and lymphatic branches in EAT constitute the physiological and pathological microenvironment of lymphatic vessels. Therefore, increased inflammatory factors, macrophages, and adipokines in EAT and PVAT can promote AS in an endocrine or paracrine way.159–161 The study by Ioannis Drosos et al. on human specimens confirmed that PVAT of AS patients had more extensive lymphatic vessels, inflammation, and fibrosis 43 by comparing the number of atherosclerotic vessels and PVAT lymphatic vessels of an internal lacteal artery in patients undergoing bypass grafting, suggesting that the increased inflammatory response in adventitia is a promoting factor of lymphatic vessels and is related to AS.
However, the research scale of lymphatic function in the adipose tissue is still very limited.
Conclusion and Future Research Directions
In summary, lymphatic vessels play a complex role in different stages of AS. Lymphatic vessels perform vital functions in the transport of lipids and inflammation. However, the current evidence of their benefits is contradictory, and the exact mechanism of lymphangiogenesis in AS remains unclear.
Future research should focus on the molecular mechanism of lymphangiogenesis and remodeling under pathological conditions, and clarify the role of lymphangiogenesis in various stages of AS, so as to provide valuable treatment strategies. The relationship between adipose metabolism and lymphatic vessels is also a promising research direction. Whether the change in the number of lymphatic vessels around plaques is dependent on the individual gene differences or not (i.e., whether there exist congenital anti-AS and pro-AS phenotypes of humans) is worth being studied to evaluate the susceptibility to AS in human beings exposed to the similar risk factors.
In addition, AS is a complicated disease with both inflammatory and autoimmune characteristics, so the different roles of lymphatic vessels in regulating innate immunity and adaptive immunity need further explanation. To a certain extent, promoting more functional lymphangiogenesis and reducing pathological lymphangio remodeling may be a potential therapeutic target.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (82074200; 81873117).