
Abstract
Background:
Sclerotherapy is the first-line therapeutic method for lymphatic malformations (LMs). This retrospective cohort study evaluated the effectiveness and safety of a novel combined foam sclerosant: polidocanol and pingyangmycin foam (PPF), for treating cervicofacial macrocystic LMs.
Methods and Results:
From July 2018 to October 2020, 51 patients with cervicofacial macrocystic LMs were enrolled in this study. All patients received intralesional 3% polidocanol or PPF injections. The outcome was evaluated regarding demographic and clinical characteristics, degree of treatment response, and post-treatment complications. Overall, 16 patients (31.4%) underwent PPF sclerotherapy. All these patients (100%) showed remarkable reduction in lesion size within three sessions. Excellent responses were shown in 88.5% of these patients within three sessions, which is higher than single polidocanol sclerotherapy (80%). The average sessions (duration) of PPF sclerotherapy were 2.5, which was significantly shorter than the single foam sclerotherapy (p < 0.05). Treatment duration was significantly associated with age, lesion location, lesion size, and number of cysts (p < 0.05). No severe complications were noted in this study. Local or systemic complications, such as swelling and mild fever occurred but subsided without any specific treatment.
Conclusions:
PPF is a safe, and effective combined foam sclerosant for the treatment of cervicofacial macrocystic LMs. This combined foam can improve treatment response and reduce treatment duration compared with a single sclerosant. It can be broadly used if further large-scale clinical trials verify its efficacy and safety.
Introduction
Lymphatic malformations (LMs) are benign masses composed of dilated lymph-filled cysts. 1 The pathogenesis of LMs has not been thoroughly elucidated. Generally, they originate from the erroneous embryological development of lymphatic structures.2,3 Recent evidence found that somatic PIK3CA mutations might be the major cause of LMs.4,5 LMs primarily develop in the head and neck region, approximately accounting for 75% of all patients. 6 In most cases, clinical presentation, ultrasonography, and magnetic resonance imaging (MRI) are widely used to diagnose LMs. 7 The typical presentation is a noncompressible flesh-colored or bluish mass, which possibly affects not only skin and superficial soft tissue, but also deep-situated organs. 8 Hence, ultrasonography and MRI are recommended to evaluate LM extension and relationship to adjacent structures. 9
LMs can be classified into macrocystic (>2 cm in diameter), microcystic (<2 cm in diameter), or mixed cystic LMs. 10 Macrocystic LMs commonly induce head and neck asymmetry, with different extents of disfigurement. Moreover, the swelling also generates other functional disturbances, such as airway obstruction, visual dysfunction, and swallowing difficulties. 11 Since most of the lesions do not exhibit spontaneous regression, it is crucial to develop effective treatment for macrocystic LMs. Surgery, sclerotherapy, pharmacological therapy, and laser therapy are all selective therapeutic options.12–15 Because of comparatively fewer complications and lower recurrence rate, sclerotherapy has gradually become the first-line therapeutic option for macrocystic LMs.
Sclerosing agents reported previously include bleomycin, pingyangmycin, OK-432, polidocanol, etc.16–18 As a nonionic detergent, polidocanol can be applied as a foam-sclerosing agent to induce cytolytic reaction of endothelial cells. 19 Polidocanol foam relatively reduces the dose of sclerosants used, thus it has fewer potential risks of severe complications owing to overdose. 20 Furthermore, microfoams will occupy dilated lymphatic vessels and increase the lasting surface contact. 21 Hence, endothelial cytolytic reaction can obtain maximum therapeutic effects. Since polidocanol is not as potent as the traditional sclerosant ethanol, 22 a single agent cannot always achieve excellent response regarding macrocystic LMs with large cysts. In our department, polidocanol and pingyangmycin foam (PPF) has been applied for treating certain macrocystic LMs.
It is worthwhile to testify whether sclerotherapy using multiple agents can achieve promising effects without safety concerns. This retrospective cohort study aimed to evaluate and summarize the effectiveness and safety of intralesional injection of PPF for treating head and neck macrocystic LMs.
Materials and Methods
Patient enrollment
From July 2018 to October 2020, 51 patients with macrocystic LMs in the head and neck region were recruited in the Department of Oromaxillofacial Head and Neck Oncology, Shanghai Ninth People's Hospital, College of Stomatology, Shanghai Jiao Tong University School of Medicine.
Inclusion criteria included: Patients with cervicofacial LMs. The diagnosis was verified by clinical examination, Doppler ultrasonography scan, and MRI according to ISSVA definition. Exclusion criteria comprised: Patients with cervicofacial microcystic, or mixed cystic LMs; cervicofacial macrocystic LM patients with treatment history; patients with severe systematic diseases who could not tolerate sclerotherapy; and patients who were allergic to sclerosants.
The treatment protocol was approved by the Institutional Review Board of Shanghai Ninth People's Hospital Ethics Committee (SH9H-2019-TK168-1) and informed consents were signed by all patients or guardians. This study was conducted in accordance with the ethical guidelines of the Helsinki Declaration.
Sclerotherapy regimen
Fifty-one patients were divided into two groups retrospectively based on whether they received multiple foam sclerosants. All patients first underwent a thorough physical examination, and Doppler ultrasonography scan or MRI investigation. Three percent (60 mg) polidocanol (Aethoxysklerol; Kreussler Pharma, Wiesbaden, Germany), 8 mg pingyangmycin (Jilin Aodong Pharmaceutical Group Co., Ltd., Jilin, China), and 1% (25 mg) sodium hyaluronate (Sofast; Shandong Bausch-Fruida Pharmaceutical Co., Ltd., Shandong, China) were prepared. Since there is no consensus regarding the sclerosant volume for macrocystic LMs, this regimen is the modification of treatment protocols from previous studies.
PPF preparation and injection procedure are described below. First, 8 mg pingyangmycin was dissolved in 2 mL polidocanol solution, 0.5 mL sodium hyaluronate solution, and 1 mL dexamethasone (5 mg). The sclerosant foam was produced using the modified Tessari method. Briefly, two 10-mL syringe and one three-way taps were used to extract 3.5 mL combined solution and 10.5 mL ambient air, respectively (liquid:air ratio of 1:3). Syringes were subsequently pushed back and forth 20 times to prepare the sclerosant foam. The volume of a single treatment was determined by the lesion size and dose limitation. The maximum dosage of pingyangmycin per session was limited to 8 mg for adults and 4 mg for children. 7 The maximum volume of 3% polidocanol solution per session should not exceed 2 mL. 23
After appropriate sterilization, percutaneous insertion of separate transfusion needles was performed under ultrasound visualization using double or multiple syringe systems. After needles reached the cyst, the cyst was aspirated to ensure that the content was lymph fluid. Lymphatic fluid should be aspirated as much as possible. Subsequently, the combined sclerosant foam was directly injected into the cyst through one or more needles, until foam was excreted from the other one or more needles. It indicated that the cyst was filled with foam when this excretion happened and the lesion was slightly expanded with pressure. The injection sites were compressed locally and patients were carefully observed for 15 minutes. Compression pads were applied and kept on for the first 3 days.
All patients received sclerotherapy at an outpatient clinic and they were asked for follow-up examination or treatment 4 weeks later. Generally, one treatment circle consisted of one to three sessions based on individual response, size, and number of cysts. Sclerotherapy was considered completed when the cysts resolved and no lymph fluid was aspirated. The total dose of pingyangmycin was recommended not to exceed 40 mg, 24 whereas the maximum dose of polidocanol should be limited to 2 mg/kg. 23 After treatments were finished, the patients were suggested to revisit at an interval of 3 months.
Outcome measurement
Outcome measurement mainly included demographic and clinical characteristics, treatment response, and post-treatment complications. 25 All patients were evaluated by the other three independent physicians. Any presentation of complications was recorded and treatment response was assessed by clinical examination and imaging findings after each session. The treatment response was classified as follows24,26: Excellent response (completely cured and reduction of lesion size ≥90%), moderate response (remarkable improvement in appearance and reduction of lesion size ≥50%, <90%), and poor response (improvement in appearance and reduction of lesion size <50%). All patients were followed up for an average of 16.5 months.
Statistical analysis
The collected data were analyzed by the SPSS software package (version 21.0; SPSS, Chicago, IL). Descriptive data were depicted as frequency, percentage, or mean, range, and standard deviation. Mann–Whitney U test or multivariate ordinal logistic regression was performed to detect any differences between groups regarding nonparametric ordinal variables. Fisher's exact test and Student's t-test were used as appropriate. p-Value <0.05 was considered statistically significant.
Results
Demographic and clinical characteristics
Fifty-one patients were enrolled as eligible cases in this study. Thirty-five patients (68.6%) received polidocanol foam sclerotherapy. Sixteen patients (31.4%) underwent PPF sclerotherapy. Three percent polidocanol was used in all patients. According to previous studies, higher concentrations were correlated with better therapeutic effects, and 3% was the highest concentration used for sclerotherapy. 22 Among all patients, 28 were males and 23 were females. The gender ratio was ∼1:1. The mean age was 19.15 years (range, 0.17–63 years) at their first treatment. All patients had lesions in the cervicofacial region: 18 in the neck, 24 in the face, 6 in the parotid, 1 in the temporal region, 1 in the left cervical and temporal region, and 1 in the right face and temporal region, respectively. All were unilateral lesions.
The lesion size ranged from 2.2 to 12.5 cm in diameter, and number of cysts per lesion ranged from 1 to 3 as assessed by imaging findings. Overall, a total of 53 lesions and 72 cysts were observed in these 51 patients. In this study, patients received 1 to 5 sclerotherapies, and the average session was 2.9. The average follow-up period was 16.5 (range, 6–30) months (Table 1).
Demographic and Clinical Characteristics of Patients
PPF, polidocanol and pingyangmycin foam.
Treatment response
Twenty-eight patients (80%) who received single polidocanol foam therapy responded excellently after one treatment circle (1–3 sessions). The other seven patients showed excellent responses within five sessions. The average sessions for all these patients completely cured were 3.09. Concerning the patients receiving PPF sclerotherapy, 16 patients (100%) showed excellent or moderate responses within 3 sessions, 14 (87.5%) of which responded excellently. This is higher than patients treated with single foam sclerotherapy (p > 0.05). Among these 16 patients, 3 (18.75%) and 5 (31.25%) patients achieved excellent responses after 1 and 2 sessions, respectively.
Two of the 16 patients (12.5%) showed moderate responses after three sessions. They voluntarily continued sclerotherapy with identical combined foam sclerosants and eventually displayed excellent responses after the fourth and fifth session, respectively. The average duration for these patients completely cured was 2.5 sessions, comparatively shorter than the patients treated with single foam sclerotherapy (p < 0.05) (Table 2). The total volume of the sclerosants did not exceed the maximum volume in all patients.
Comparison of Treatment Response Between 3% Polidocanol and Polidocanol and Pingyangmycin Foam Therapy
Factors associated with PPF treatment duration were analyzed regarding age, gender, lesion location, lesion size, and number of cysts (Table 3). According to the data, treatment duration was significantly associated with age, lesion location, lesion size, and number of cysts (p < 0.05). Lesions with larger sizes or more cysts tended to require more treatment sessions. Furthermore, treatment duration decreased with the increase of age. All adults (>18 years old) achieved excellent responses within three sessions. Younger patients experienced relatively longer duration. Additionally, treatment duration of facial lesions was comparatively longer than cervical lesions. Two patients who accepted additional sclerotherapies had facial lesions. Typical images from patients before and after treatment are demonstrated in Figures 1–3.
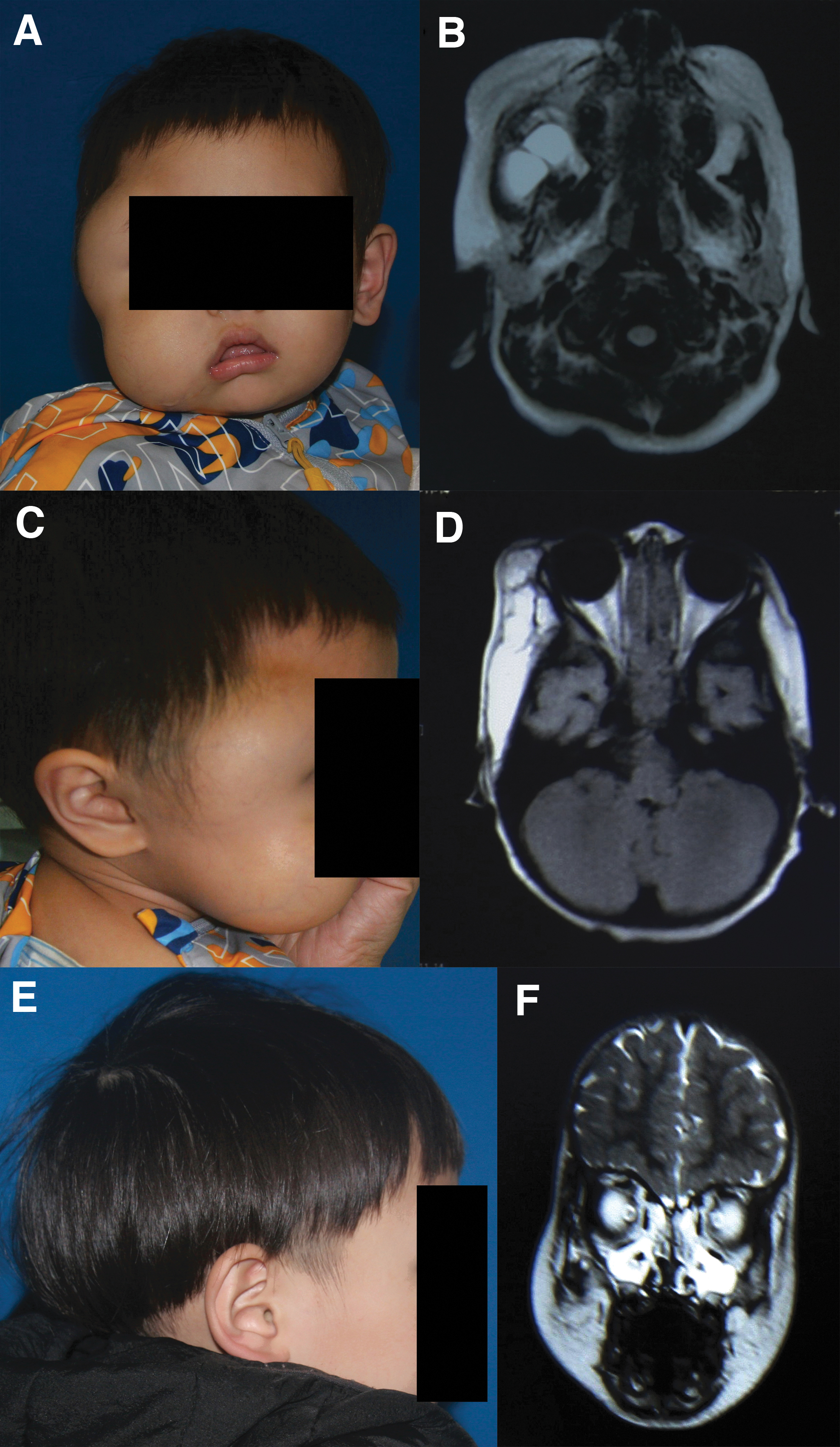
Clinical photographs and MRI images of a 2-year-old boy with macrocystic LMs.
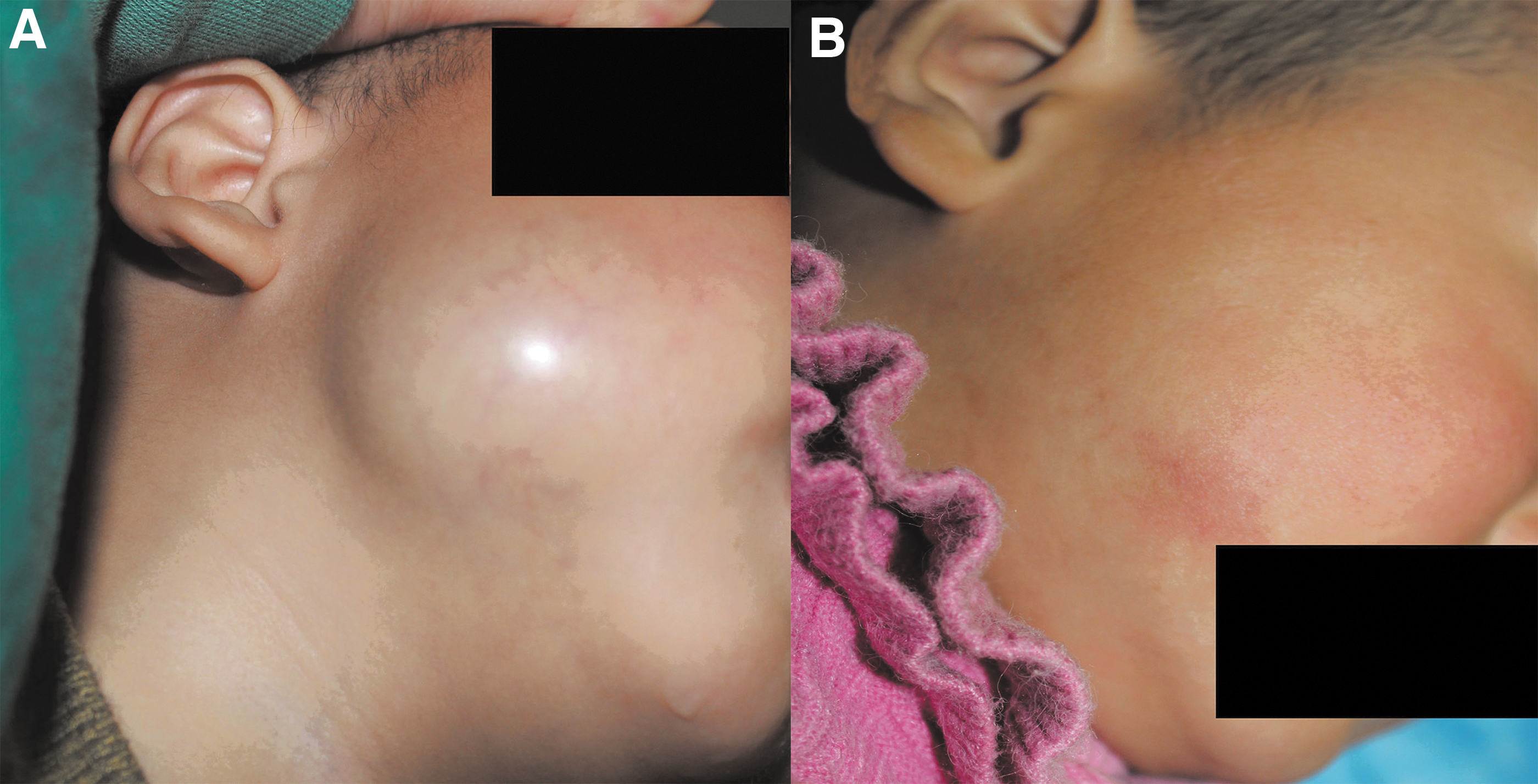
Clinical photographs of a 3-year-old boy with macrocystic LMs.

Ultrasonography of a 9-year-old boy with macrocystic LMs.
Factors Associated with Polidocanol and Pingyangmycin Foam Treatment Duration (Sessions)
95% CI, 95% confidence interval; OR, odds ratios.
Complications
No severe complications were found in all patients. No skin ulceration or necrosis, nerve damage, or deep-seated organ dysfunction was detected. Thirty-nine patients (76.5%) underwent slight swelling after sclerotherapies, the average swelling period was 5.4 days (range, 3–10). The occurrence of swelling was not significantly correlated with aforementioned factors (p > 0.05). Among patients injected with PPF, one (6.25%) developed evident swelling after injection, but this symptom relieved in 2 weeks without a sign of infection or other discernable complications. As to systemic complications, one patient (6.25%) experienced mild fever under 38.5°C in the first 3 days after sclerotherapy. Moreover, gastrointestinal reaction and sleep disorders, respectively, were found in one patient (6.25%). These mild complications subsided within 1 week without any specific treatment.
Discussion
Sclerotherapy can damage the endothelium of the lymphatic vessels due to inflammation reaction, thrombotic vascular occlusion, and fibrosis, resulting in the regression of lesions. Our previous studies had confirmed that pingyangmycin was a safe and effective sclerosant for patients with microcystic LMs.7,27 However, which sclerosant is the optimal option for macrocystic LMs remains controversial.
There were massive records of polidocanol foam sclerotherapy for vascular malformations in previous studies. Blaise et al. 22 evaluated the efficacy of polidocanol foam among 24 vascular malformation cases. The results showed reduction of lesion size in 95% patients. Yamaki et al. 26 demonstrated that polidocanol foam was effective and safe for treatment in 32 LM patients, of which macrocystic LMs accounted for 56%. Excellent and moderate responses were observed in 88% of the patients, while 13% patients encountered intralesional hemorrhage. Collectively, polidocanol is a safe but relatively less potent sclerosing agent compared with traditional sclerosants. In some macrocystic LM cases, a single sclerosant cannot achieve excellent outcomes. Accordingly, this study assessed the therapeutic effect of a novel combined sclerosant PPF.
In an in vitro assay, 28 investigators testified the stability of bleomycin polidocanol foam. The study showed that the half-life of the sclerosant foam significantly increased with the addition of bleomycin. Although bubble diameter and wall thickness were increased with the addition of bleomycin, the viscosity of the combined solution simultaneously elevated, leading to stability enhancement. Pingyangmycin, one of the most frequently documented sclerosing agents, 29 is isolated from bleomycin (bleomycin A5). With similar structure and chemical components, pingyangmycin and bleomycin are widely used for treating various tumors and vascular malformations. 7 Pingyangmycin was as effective as bleomycin, and it had fewer complications and lower cost. 30
Our previous study found that pingyangmycin was effective in treating deep-seated facial and tongue microcystic LMs.7,27 Regarding macrocystic LMs, another study reported that 32 patients received pingyangmycin injection. Around 84.38% participants ultimately exhibited satisfactory recovery. The only side effect was transient fever. 24 In addition, Luo and Gan 31 validated the effective influence of pingyangmycin on curing macrocystic LMs alike. These results confirmed that pingyangmycin was a suitable sclerosing agent for combined foam sclerosant.
Hyaluronate acid (HA) is an internal glycosaminoglycan synthesized and released into the extracellular matrix and blood.21,32 Medical sodium hyaluronate is broadly used in tissue engineering and regenerative medicine. 33 Previous studies found that the addition of a small amount of HA overtly improved the stability of polidocanol foam. The principal reason for the enhancement of stability might be the increased shear viscosity. 34 Chen et al. 21 recruited 70 patients with venous malformations. After injection of polidocanol and 0.1 mL HA combined foam, the response rate was up to 100% eventually. Moreover, most of the patients did not experience complications, except for immediate swelling. 21 HA is a biodegradable, nontoxic, and nonimmunogenic substance, 33 and it is chemically compatible with polidocanol and pingyangmycin.
Since the optimal volume of HA dissolved in sclerosant foam has not been fully discussed, the current study added 0.5 mL hyaluronate in PPF. According to the result, the effectiveness and safety of the combined sclerosant foam were desirable when the volume of hyaluronate was set up as 0.5 mL. Ideally, in the PPF sclerosants, polidocanol foam thoroughly interacts with endothelium, while pingyangmycin will be dispersed in the foam and strengthen the therapeutic effect of sclerotherapy through synergy with polidocanol foam. The addition of hyaluronic acid will raise and prolong the stability of the combined foam. It is a safer choice to select pingyangmycin and polidocanol because these two substances were considered stable with respect to chemical and physical properties, and it was proved that no chemical reaction would occur after drug mixture. 28
Few studies had explored the outcomes of combined foam sclerosant sclerotherapy for vascular malformations so far. In a retrospective study, 34 patients with venous malformations received ethanol, 3% sodium tetradecyl sulfate (STS) or combination sclerotherapy. The results showed that combination treatment of ethanol and 3% STS had the highest success rate, and the lowest complication rate. 35 Another study involved two nonfoam sclerosants: OK432 and Ethibloc. Although there was no significant difference between the combination therapy and single sclerosant therapy regarding the treatment outcome, the average duration in the dual therapy group was relatively shorter than OK432 group. 36 Accordingly, combined sclerosants used for sclerotherapy might not only obtain higher success rate, but also reduce the treatment duration.
This study showed that PPF was an ideal combined drug for sclerotherapy. All 16 patients who received PPF treatment ended up with remarkable reduction in lesion size in one treatment circle, and 87.5% of them showed excellent treatment responses, which was relatively higher than patients treated with polidocanol sclerotherapy (p > 0.05). This cure rate was in line with, or even higher than the limited previous studies. These studies used single polidocanol foam for LM therapy.19,22,26 Moreover, PPF treatment achieved excellent responses among all patients in five sessions eventually. The average treatment sessions were significantly lower than the single sclerosant therapy. These data reflected that polidocanol and pingyangmycin exerted synergistic effects on macrocystic LM. This combined foam sclerosant improved the treatment response, and reduced the treatment duration.
The concentration of polidocanol solution chosen for this study was 3%, which was a common concentration used for sclerotherapy.23,26 According to our data, PPF treatment duration was significantly associated with age, lesion location, lesion size, and number of cysts. Patients with larger lesions or more cysts needed more sessions to achieve excellent responses. It is obvious that lesions with larger sizes or multiple cysts required more sessions to increase the interaction time between sclerosants and endothelium. Younger patients appeared to experience longer treatment duration than adults. The reason may be that growth of macrocystic LMs will be terminated with the increase of age. Among younger patients, in most cases, the lesions tend to grow consecutively before the growth termination.
Patients with facial lesions had relatively longer treatment duration than cervical lesions. This might be due to the complicated anatomy in the facial region. Although sclerotherapies were performed guided by ultrasonography, it was possible that PPF was not directly introduced into minor cysts because of image deviation, and anatomical complexity. Regarding complications, no severe complications were observed in this series. Swelling, mild fever, gastrointestinal reaction, and sleep disorder were found. All these complications gradually subsided without any specific treatment. Consequently, PPF is a safe and efficient sclerosant for treating cervicofacial macrocystic LMs. This combined sclerosant foam can improve treatment response and reduce treatment duration compared with polidocanol foam.
This retrospective cohort study investigated whether a novel combined foam sclerosant (PPF) could enhance therapeutic potency of macrocystic LMs. Nevertheless, owing to the strict inclusion and exclusion criteria, this study rendered limited cases and relatively short follow-up period. Therefore, completely designed studies with more participants, longer period, such as randomized controlled trial and prospective cohort study, should be performed to further investigate the role of combined foam sclerotherapy for macrocystic LMs or other vascular malformations.
Conclusions
In summary, PPF is a promising combined foam sclerosant. Intralesional injection of PPF is a safe and effective method for treating cervicofacial macrocystic LMs. This combined foam can be broadly used clinically if further large-scale clinical trials verify the efficacy and safety.
Footnotes
Acknowledgment
The authors thank all the lymphatic malformation patients who participated in this study.
Authors' Contributions
Q.W.: study design, data acquisition, data analysis, article writing, final approval of the version to be published, and accountable for all aspects of the work; Q.Z.: data acquisition, data analysis, article revision, final approval of the version to be published, and accountable for all aspects of the work; Z.Z.: data acquisition, article revision, final approval of the version to be published, and accountable for all aspects of the work; C.L.: data acquisition, article revision, final approval of the version to be published, and accountable for all aspects of the work; and J.Z.: study design, article revision, final approval of the version to be published, and accountable for all aspects of the work.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (No. 81771087, 81901021, and 82071130).