
Abstract
Background:
This study aimed at presenting a prospective surveillance model of care delivered at home for women qualified for surgery due to breast cancer under the epidemic-related restrictions.
Methods and Results:
Women (age ≥18 years, diagnosed with breast cancer, no clinical features of upper limbs lymphedema, and a volume difference between the limbs <5%, not using any prophylactic compression products) will be provided with comprehensive education in the field of self-measurements and lymphedema prevention. The outcome measures include limb volume (circumferential measurements with a tape at 4 cm intervals), simplified protocol of three measurement points combined with the symptoms monitoring (according to the physical section of Lymphedema Quality of Life Inventory [LyQLI]). We propose a new calculation method as the RACI (relative arm circumference increase) in accordance with previous research—RAVI (relative arm volume increase) and the new proposal—the RACD (relative arm circumference difference). According to cylinder formula it can be calculated that 5% increase in limb volume results in ∼2% change in RACI. Regular appointments will be planned at 3, 6, 9, and 12 months after the enrollment. Additional urgent appointments will be arranged after the home or phone “red flags” (an increase circumference by ≥2%, positive pitting test, and any new symptoms) detection. We hypothesize that performing only three measurements combined with the typical symptoms monitoring would be accurate for lymphedema diagnosis based on the RAVI of ≥5%. Moreover, RACI/RACD increments combined with positive symptoms would correlate with RAVI.
Conclusions:
The new proposal of protocol can be the optimal solution in COVID-19 pandemic.
Introduction
Breast cancer-related lymphedema (BCRL) of the upper limb remains one of major long-term complications among people treated for breast cancer, which occurs most often within the several months after surgery. Conservative treatment of BCRL based on complex physical therapy using compression, manual lymph drainage, and physical exercise is widely used, 1 but access to physiotherapy during the COVID-19 pandemic is strongly limited. Therefore, education of people at risk and prevention of this chronic disease play a special role. The patients who are at high risk (undergoing radical surgery combined with lymphadenectomy, complementary radiotherapy) as well as patients with an elevated body mass index need individually tailored prophylactic procedures and education in the field of skin care, selection of physical exercises, and may require timely application of compression, in the early course of the illness. 2
It is shown that the early detection of BCRL, leading to earlier physiotherapy, may improve outcomes. There are several different methods commonly used to detect and monitor lymphedema. Limb volume measurements (by Perometer) may be as accurate as bioimpedance spectroscopy. 3 However, measuring limb volumes, even under optimal condition at the clinic, is not easy and dependent on the observer. 4 For practical home situations, based on lay carers or patients, an easy, objective, and reliable method of early BCRL diagnosis is still lacking. Patients' experiences of fullness, heaviness, limb achiness, the sensation that clothing is becoming tighter, or cluster signs typical for tissue edema (as pitting, firmness, response to limb elevation, or skin changes) seem to be insufficient for accurate diagnosis. 5 Undoubtedly some limb size monitoring is necessary and highly valuable for patients at risk of developing BCRL. This burden of systematic evaluation for all indicators is central to further care timing.
The circumferential tape measurement has been used most commonly as an inexpensive, reliable, and highly accessible diagnostic method. 6 Having access to preoperative limb measurements is crucial to accurately diagnose subclinical lymphedema determined as 5% of the relative arm volume increase (RAVI) 3 from the preoperative baseline. 7 Home limb circumference measurements have been already documented in BCRL: first as a figure-of eight for hand swelling, 8 and lately for arm monitoring. 9 Both methods are reliable, valid, and comparable with volume changes performed by Perometer among women with and also without BCRL.
Segmental limb volume measurement appeared to be better predictor of lymphedema onset than the whole limb monitoring. 10 According to cylinder formula it can be calculated that 5% increase in limb volume results in ∼2% change in its circumference (relative arm circumference increase [RACI]). 9 Based on these data we hypothesize that self-performing three measurements only (one on the hand, one at the forearm, and one at the arm level) combined with monitoring of the typical symptoms and signs (according to the physical section of Lymphedema Quality of Life Inventory [LyQLI] 11 ) by patients after breast cancer surgery, would be sufficient and accurate for the early (subclinical) lymphedema diagnosis.
Materials and Methods
Participants
Those eligible to participate in this trial will be of the following criteria: (1) age ≥18 years, (2) diagnosed breast cancer, (3) no clinical features of upper limbs lymphedema, (4) a volume difference between the limbs <5%), (5) not using any prophylactic compression products, and (6) given written consent to participate. Exclusion criteria will include poor performance status as defined by Karnofsky Performance Status Scale ≤60 (requires at least occasional assistance). Research staff will recruit the participants from the patients admitted to the oncology center before the surgical treatment of breast cancer; further evaluation will take place at the Lymphedema Treatment Clinic.
Intervention and monitoring
Patients enrollment and education
An experienced physiotherapist will measure subjects' body weight, limbs volumes—based on circumferential calculations at 4 cm intervals starting from the wrist up to the axilla. In addition, hand circumference will be taken.
Enrolled patients will be educated in lymphedema prevention by a trained physiotherapist, supported by written instructions. Physical exercise program for upper limbs will include aerobic exercises (flexion, extension, abduction and adduction of the shoulder, shoulder rotation, flexion and extension of the elbow, and fist clenching) combined with breathing exercises for 15 minutes a day. Proper skin hygiene will be obtained by daily washing with hypoallergenic soap, exact drainage, especially places between fingers and skin moisturizing.
Patients will be provided with comprehensive education in the field of self-measurements. They will receive brochure instructions on performing the pitting test and checking circumference measures on one's own: In the sitting position with their arms supported on the table with 35° elbow flexion participants will measure with a tape the forearm 15 cm above the wrist and the arm 10 cm above the elbow. Difficulties in keeping the tape at a constant and replicable tension will be minimized using the tape that tightens with the push of a button provided by the same manufacturer. All the data will be collected weekly (always the same weekday) and written down in the home diary. Patients will be told to contact immediately the physiotherapist, to make an ambulatory appointment, if they notice one of the “red flags”:
An increase in any RACI by ≥2%—quantified individually (Table 1) Positive pitting sign of the limb skin Any new symptom or sign indicating for the risk of an early lymphedema it means: pain, discomfort, limb heaviness, weakness, tingling, numbness, and visible skin changes.
Limb Circumferences and Corresponding Its 2% Increments (in cm, Rounded to One Decimal Place)
Telephone assessment
Researchers will contact participants once a month to motivate and encourage patients to continue self-management, remind about self-measurements, and collect information about the presence or absence of symptoms and signs and report circumference values. Ambulatory appointment will be immediately provided if any of the home “red flags” are detected or the difference between the corresponding limb circumferences (relative arm circumference difference [RACD]) rises ≥2% above the enrolment, baseline time (so called phone “red flag”).
Ambulatory assessment
Regular appointments will be planned at 3, 6, 9, and 12 months after the enrolment. Physiotherapist will perform pitting test, measure body weight, limb volumes based on circumferential calculations at 4 cm intervals starting from the wrist up to the arm. In addition, hand circumference will be taken. Additional urgent appointments will be arranged after the home or phone “red flags” detection. The diagnosis of the lymphedema will be based on the RAVI of ≥5%. In this case, the end point of the study will be achieved and the 18–21 mmHg compression sleeve will be prescribed to be worn during a day.
Outcomes
The primary outcome for this intervention is to validate assumptive subclinical lymphedema screening, based on limb circumference self-measurements combined with symptoms and signs monitoring. We expect that >90% of home “red flags” will be confirmed as subclinical lymphedema measured ambulatory.
We will consider that the intervention has adequate feasibility if at least 70% of eligible patients provide consent and be enrolled in the study. As a result of assumptive retention strategy (written instructions, follow-up phone calls, and immediate appointments at the clinic) the expected retention rate after 1 year of observation will be not <85%. 12
Sample size
According to type I (α = 0.05) and II (β = 0.20) errors given for the agreement between home and ambulatory measurements by using intraclass correlation coefficient of not <0.85 a sample size of 31 persons will be necessary. 13 Assuming that lymphedema incidence among breast cancer survivors is ∼30% 3 and anticipating 10% dropouts, a group of 99 enrolled women will be needed.
Ethics
In this study, we will follow Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 14 recommendations (Fig. 1). Protocol for the research project has been approved by the local ethics committee (No. 60/KBL/OIL/2021).
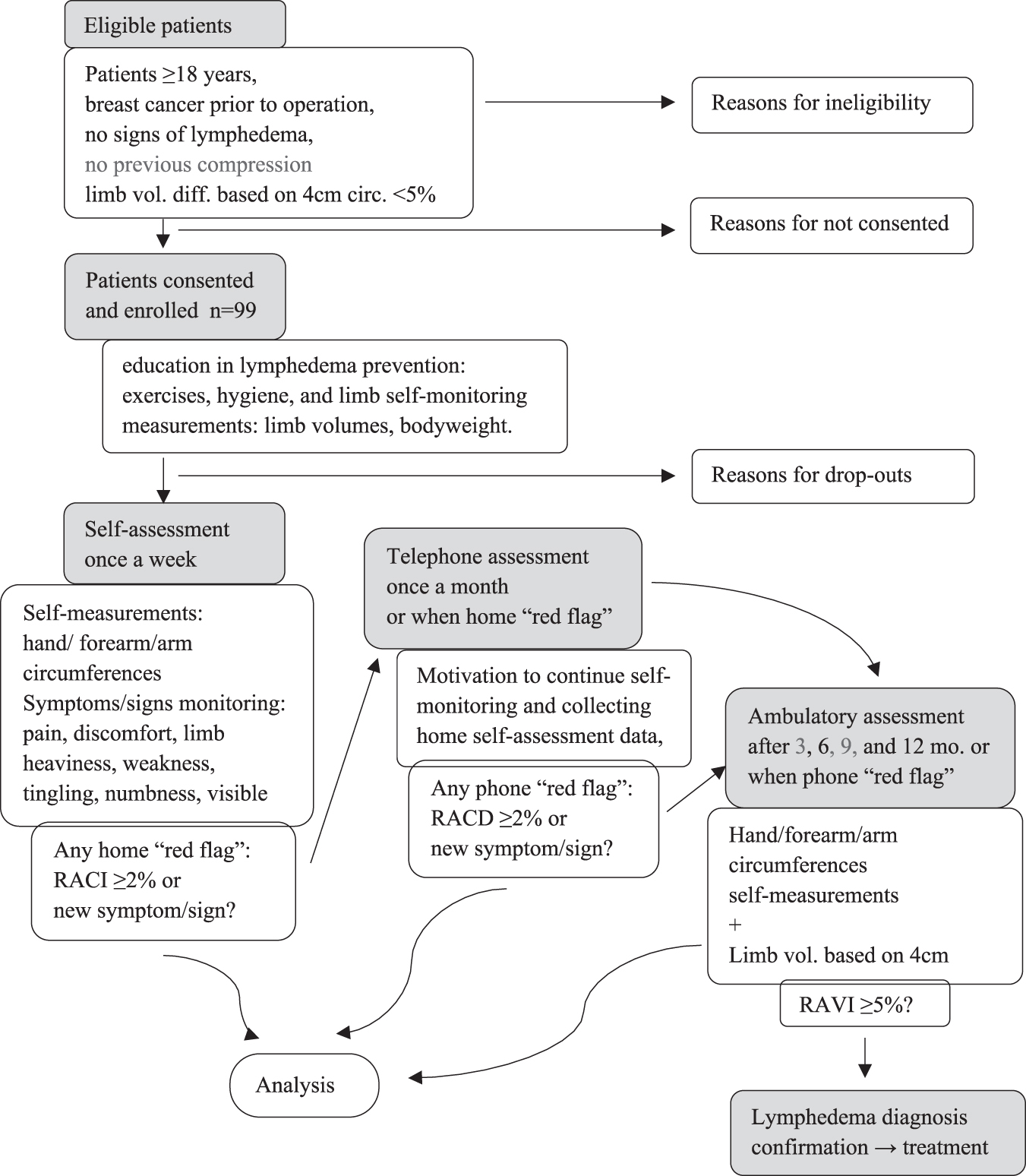
Recruitment and follow-up flow diagram. RACI, relative arm circumference increase; RACD, relative arm circumference difference; RAVI, relative arm volume increase.
Discussion
The COVID-19 pandemic has significantly reduced the availability of outpatient care provided to BCRL. To support patients, traditional forms of physiotherapy ought to be replaced by alternative remote forms enabling early diagnosis and implementation of proper prophylactic management in breast cancer survivors.
This study aims to present a prospective surveillance model of care delivered in home. It consists of limb volume and symptoms monitoring, education, and support to promote self-management and physical activity for women qualified for surgical treatment due to breast cancer under the epidemic-related restrictions.
A prospective surveillance and intervention model of care has been recognized as an optimal framework for the early detection and management of subclinical lymphedema. Recommended practice requires that individuals at risk of developing lymphedema regularly attend clinics on a 3–6 monthly cycle for 3 years for detecting subclinical lymphedema, 15 but the number of face-to-face outpatient appointments should be reduced due to growing spread of COVID-19.
To improve the clinical outcome in breast cancer survivors at risk of lymphedema who do not have access to a physiotherapist specialized in lymphedema therapy, we propose self-managed surveillance that can be maintained after the pandemic era. This program includes fulfillment recommendations, self-monitoring of the limb size combined with the typical self-perceived symptoms and signs monitoring at home for 12 months for early lymphedema diagnosis. Proposed weekly self-assessment within the same weekday can be recognized as a compromise between close surveillance and the excessive burden for the patient.
Currently there is no consensus and diagnostic criteria are not standardized concerning the best measuring tool to detect both subclinical lymphedema and early established lymphedema. 3 Different investigators use different methods, which can delay intervention to prevent or alleviate lymphedema. In this study protocol we have chosen the circumferential tape measurement as an inexpensive, reliable, and highly accessible diagnostic method. 6
Circumferential limb measurements have been used most commonly to assess lymphedema, as this approach is widely available and has no specific space or equipment requirements. Lymphedema incidence rates vary by definition. Previous evidence suggests a ≥ 10% limb volume change criterion be used for lymphedema evaluation. 16 However, even a 5% increase in limb volume may have a negative impact on daily activities, reducing the quality of life. 17 In our protocol we suggest a more precise and clinically meaningful criteria for diagnosis BCRL with ≥5% of relative volume change from the preoperative baseline. 3
Preliminary reports indicate that it is possible to take self-measurements of the limb at risk of lymphedema with a tape, after appropriate training of women treated for breast cancer and the support of a physiotherapist. High correlations were reported between self-measurements and measurements performed by a physical therapist. 9 We propose a simplified protocol of three measurement points and a new calculation method as the RACI in accordance with previous research 9 and the new proposal—the RACD. We hypothesize that performing only three measurements combined with the typical symptoms and signs monitoring would be sufficient and accurate for early lymphedema diagnosis.
Some studies confirm that self-reported assessment of symptoms (e.g., swelling, heaviness, redness, and tenderness) and limb function change by breast cancer survivors can be an effective component of assessment for lymphedema.16,18 We expect that RACI/RACD increments combined with positive symptoms/signs would correlate with RAVI-based volume increase. We, therefore, believe that this new approach would have a high clinical utility to promote independence in detecting changes in arm size, and give easily interpreted outcomes by using low-tech measurement tools at home.
A major benefit of self-managed surveillance for patients is to provide cost-efficient early detection of onset of BCRL, which can lead to earlier treatment and better prognosis. Self-managed surveillance for BCRL is also associated with the less progress of disease and can support the self-efficacy. 9 Women being more actively involved in their care become more independent in a daily life. Self-efficacy is also a key factor linked to long-term adherence to treatment, increasing motivation and leads to greater well-being in breast cancer survivors.
Conclusions
The new proposal of protocol based on simplified self-measurements combined with monitoring of the typical symptoms and signs can be sufficient for the subclinical lymphedema diagnosis and the optimal solution in COVID-19 pandemic.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Publication financed by the Ministry of Science and Higher Education under the 2019–2022 Regional Initiative of Excellence programme, project number: 022/RID/2018/19.