
Abstract
Background:
Recent guidelines recommend avoiding venipuncture to prevent lymphedema for breast cancer patients. This study investigated whether single or multiple sterile venipuncture procedures develop a systemic inflammation or infection and increase lymphedema in the rabbit ear lymphedema model.
Methods and Results:
Eighteen New Zealand white female rabbits were included. The right ear lymphedema model was created by surgical procedure; then, rabbits were divided into three randomized groups. Single and multiple venipuncture procedures were applied at least the 60th day after surgery for Group I and II, respectively. Group III was a control group. C-reactive protein (CRP) and procalcitonin (PCT) levels were analyzed to determine inflammation and infection. Ear thickness measurements were applied using a vernier caliper to assess the differences in lymphedema between the ears. All rabbits were euthanized on the 90th day after surgery. Histopathological analysis was performed to evaluate lymphedema by measuring tissue thicknesses. Ear thickness measurements showed that ear lymphedema was developed and maintained with surgical operation in all groups (p < 0.05). There was no difference in the ear thickness measurements between and within-groups results (p > 0.05). CRP and PCT levels were below the lower detection levels in all groups. According to the differences of histopathological ear distances, there were significant differences within-groups for all groups (p < 0.05), and no differences were identified between groups (p > 0.05).
Conclusion:
This experimental study demonstrated that single or multiple sterile venipuncture procedures did not trigger infection or inflammation and did not exacerbate ear lymphedema in the rabbit ear lymphedema model.
Introduction
Lymphedema is the accumulation of protein-rich fluid in the intercellular space due to the failure of the lymphatic system to transport intercellular fluid effectively. 1 Breast cancer (BCa) patients who have undergone sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND) have an increased risk of lymphedema development. 2 The lymphedema incidence was shown to be ∼21% for the women with BCa in a meta-analysis. 3
Notably, guidelines, including anecdotal and limited scientific evidence, contain several recommendations on preventing BCa-related lymphedema. 4 The most common recommendations are to avoid (1) being taken blood from the affected extremities, (2) receiving any intravenous intervention, or (3) any needle sticks (vaccinations, blood-drawing, intravenous lines, and acupuncture) for BCa patients who received SLNB and or ALND. 5 The main aim underlying these recommendations may be to reduce the risk of developing or increasing lymphedema.
However, there is no consensus in the current literature on whether these anecdotal recommendations disrupt skin integrity or lead to the development of lymphedema. 5 The strict advice, including not to perform venipuncture on the affected side, may be abandoned because there are no scientific data based on a high level of evidence for this advice. Studies on the subject generally consist of case reports, retrospective, or methodologically flawed studies.6–8 The evidence base studies are severely lacking in this area. For this reason, there is a paucity of evidence to support avoiding venipuncture in literature.
C-reactive protein (CRP) is one of the most potent acute-phase reactants, with plasma levels rising to 1000-fold in response to stress, trauma, infection, inflammation, surgery, or proliferation. 9 The molecular and physiological characteristics of rabbit CRP are strikingly similar to human CRP in various ways.10,11 In addition, rabbit CRP has been demonstrated to be very comparable with human CRP, in terms of its overall features and the conditions that influence its emergence in the blood. 11 For example, rabbit CRP acts as a vital acute phase reactant or inflammatory marker. Rabbit CRP levels rise to about 100 mg/L upon inflammatory stimulation and are expected as <3 mg/L without any inflammation. 12 CRP elevation is expected to occur 24–48 hours after the initial inflammatory response. 13
Procalcitonin (PCT) has attracted attention as a possible infection marker concerning the acute-phase response. 9 The blood level of PCT rises in response to any pro-inflammatory stimulus above the detection limit (10 pg/mL). PCT levels increase with bacterial infections despite viral or noninfectious inflammation. 14 PCT induction occurs at ∼2–4 hours after the onset of sepsis and peaks at 24–48 hours. 15 The results of blood samples obtained at 12, 24, and 48 hours demonstrated that the sensitivity of PCT was >90% in an experimental rabbit appendicitis model. 16
The main aim of this study was to investigate whether single or multiple sterile venipuncture procedures develop a systemic inflammation or infection in a rabbit ear lymphedema model. The second aim was to determine whether these venipuncture procedures exacerbate lymphedema.
Materials and Methods
This study was conducted in the Laboratory Animal Breeding and Experimental Research Center, Gazi University. Because the local Ethics Committee for Animal Experiments (Approval date and number: 29/01/2018-E.17872) allowed a maximum of 6 rats for each group due to 3Rs principles (replace, reduce, and refine), 18 New Zealand white female rabbits, 2.5–3 months old, were included in the study. All the rabbits were fed ad libitum with standard pellet feed and central water. The ambient temperature was regulated between 18°C and 20°C, and the humidity of the environment was ∼40%.
The rabbit ear lymphedema model, a 94% reliable method for developing lymphedema, was created with surgical intervention for all groups. 17 Before the surgery, anesthesia was provided through intramuscular ketamine (45 mg/kg) and xylazine (5 mg/kg) injections and the operation site of the ear was shaved. Only the right ears of the rabbits were operated on. Under sterile conditions, auricular lymph nodes and lymph collectors located to the dorsum of the rabbit's ear were dissected from the main vascular body. 17
After the operation, rabbits were divided into three equally randomized groups: Group I (n = 6), Group II (n = 6), and Group III (n = 6). Single and multiple venipuncture procedures were performed to the distal part of the lateral ear vein with a standard sterilization process for rabbits in Group I and Group II, respectively. In literature, it has been reported that edema remains stable from the 60th day after surgery. 18 To focus on lymphedema and eliminate edema that develops secondary to surgery, a single venipuncture procedure was performed on the 60th day after the surgery for Group I; multiple venipuncture procedures were performed for Group II on 60th, 62nd, and 64th days after surgery. To confirm penetration into the distal part of the lateral ear vein, 0.05 mL of blood was received from the rabbits during venipuncture. No intervention was applied on rabbits in Group III. The study was conducted on 18 rabbits without any dropout.
Outcome measures
CRP and PCT analysis
Three milliliters of blood samples were received from vena saphena magna of the rabbits in all groups in sterile conditions on the 60th and 62nd days after the surgery. Extra blood samples were received for Group II on the 64th and 66th days after surgery. A yellow-capped gel tube was used to analyze CRP and PCT levels for determining systemic inflammation and bacterial infection, respectively. The tubes were centrifuged at 3000 rpm for 10 minutes after 30 minutes of clotting time.
Serum CRP measurement was performed on the Beckman Coulter AU680 autoanalyzer system (Beckman Coulter, Inc., Brea, CA), using the immunoturbidimetric method, with the same manufacturer's CRP kit. Serum PCT measurement was performed on the Roche Cobas e 601 autoanalyzer system (Roche Diagnostics GmbH, Mannheim, Germany) using the electrochemiluminescent immunoassay method, with the Elecsys Brahms PCT kit of the same manufacturer. The assays used for CRP and PCT measurements in the study have lower detection limits of ≤0.18 mg/L and ≤0.02 ng/mL, respectively.
Measurement of ear thickness
The rabbits' right and left ear thicknesses were measured on the 60th and 90th day after surgery for all groups using a vernier caliper from 1 cm distal to the medial border of the skin bridge (Fig. 1). Both ears were measured three times to obtain an average value. A 15-year experienced veterinarian applied each measurement. Differences in the right and left ear thicknesses were calculated for each rabbit.

Measurement position of the ear thickness.
Histopathological analysis
The rabbits in all groups were euthanized on the 90th day after surgery. The tissues from the ear bridge area were placed in a 10% buffered neutral formaldehyde solution for histopathological analysis. After fixation for 1 week, samples from the middle portion of each ear were taken and processed for histopathological analysis. Tissues were embedded in paraffin and cut into 3 μm thick sections. Individual sections of each ear were deparaffinized, stained with hematoxylin and eosin, and examined at 40 × , 100 × , or 200 × magnification under a light microscope (Bx53F2; Olympus, Tokyo, Japan). The same pathologist evaluated the tissues for lymphedema and any inflammatory reaction.
Tissue thicknesses were measured from the anterior to posterior total thickness in the middle of each ear (Figs. 2 and 3). Tissue thicknesses of regions with or without lymphedema were measured by cellSens Entry-Microscopy Imaging Software (Manufacturer Olympus Life Science) using Olympus DP23 camera. In addition, immune system cells, including macrophages, were observed with the same camera to detect whether an inflammatory reaction occurred. The same pathologist performed all the histological analyses, and observations followed a single-blind method.

Measurement areas of anterior to posterior total thickness in the middle of the ear. The black lines show the obtained histopathological samples from the ears.
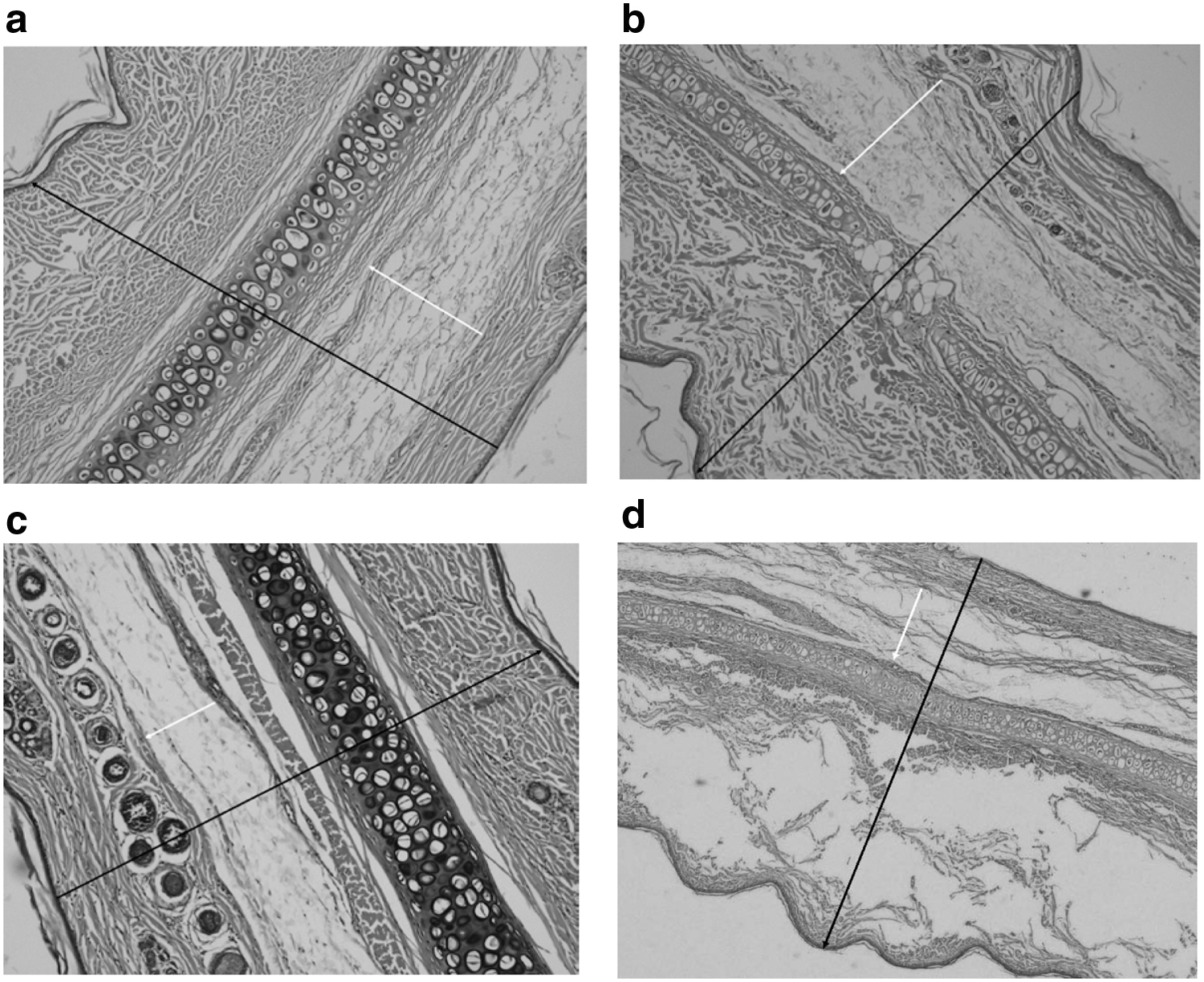
Histopathological analysis from anterior to posterior total thickness in the middle of the ear. Samples from the tissues of right ears for Group I, Group II, and Group III represents in the images of
Statistical analysis
It was performed using the SPSS version 15.0 software (SPSS, Inc., Chicago, IL). Descriptive data were stated as median (minimum to maximum). The Kruskal–Wallis and Wilcoxon tests were used for between and within groups comparisons, respectively. Statistical significance was considered p < 0.05 for all tests.
Results
The rabbit ear lymphedema model was successfully created in all rabbits according to ear thickness evaluations on the 60th day after surgery (Table 1 and Fig. 4). Table 1 demonstrates statistically significant differences (p < 0.05) between the right and left ear thickness on the 60th and 90th days after surgery in all within-groups measurements. In addition, the differences (Δ) of ear thickness evaluations between the right and left ears of the rabbits showed that there were not statistically significant differences (p > 0.05) between and within-groups analyses on the 60th and 90th days after surgery (Table 1).

A rabbit ear lymphedema model sample on the 60th day after surgery.
The Results of Right and Left Ear Thickness Measurements of the Rabbits
The bold values show the statistical significance.
p < 0.05.
Group I: Rabbits received single venipuncture, Group II: Rabbits received multiple venipunctures, Group III: No venipuncture (control group).
Wilcoxon test.
Kruskal–Wallis test.
According to the biochemical analyses, CRP and PCT levels were below the lower detection values (<0.18 mg/L and <0.02 ng/mL, respectively) in blood samples obtained from all rabbits.
Histopathological analysis based on the entire surface distance of the ears showed that there were significant differences between the right and left ears in within-groups analysis for Group I (p = 0.043), Group II (p = 0.028), and Group III (p = 0.043). In addition, there were no differences between-groups analysis according to the histopathological measurements of ear tissue thickness results (p > 0.05). The detailed results are shown in Table 2. In addition, the pathologist did not detect any immune system cells, including macrophages, in either ear.
The Results of Histopathological Distance Measurement
The bold values show the statistical significance.
p < 0.05.
Group I: Rabbits received single venipuncture, Group II: Rabbits received multiple venipunctures, Group III: No venipuncture (control group).
Wilcoxon test.
Kruskal–Wallis test.
Discussion
To the best of our knowledge, this is the first experimental study in the literature to investigate the effects of single or multiple venipuncture procedures on the rabbit ear lymphedema model. This study demonstrates that no systemic inflammation or infection occurred in the rabbit ear lymphedema model after single or multiple venipuncture procedures. Moreover, the single or multiple venipuncture procedures did not appear to exacerbate the rabbit ear lymphedema in this study.
There is a conventional assumption that venipuncture may trigger lymphedema. 19 Several guidelines have various recommendations based on only an expert opinion; however, no high evidence-based guidelines exist for lymphedema prevention. After surgery, women diagnosed with BCa are recommended to avoid venipuncture, cannulation, capillary blood glucose monitoring, and blood pressure measurements from the ipsilateral arm. 4 However, these recommendations could cause anxiety and decrease the patient's quality of life. Still, some patients have begun wearing bracelets with the words (e.g., “do not touch this arm”) warning people about having a risk for developing or triggering lymphedema. 20 We conducted this evidence-based study mainly to reveal whether inflammation and infection are the underlying concern of these recommendations in the literature.
This study was utilized as an experimental design involving rabbits because the methodology of the study, (1) creating lymphedema and (2) applying venipuncture to increase lymphedema, was not ethically viable for humans. The rabbit ear lymphedema model 18 was preferred for this study because the rabbit ear has some anatomical advantages for surgery. For example, the main blood vessels and principal lymphatics are located in the rabbit ear's external base. 21 This advantage makes surgical dissection much easier. In addition, operating on ears is not as time-consuming as operating limbs. 22 This model was used in studies with several different methodologies, including lymph node transplantation, 18 lymphovenous anastomoses, 23 fibrosis, 24 and gene therapy. 25
According to the right and left ear thickness measurements using vernier caliper on the 60th and 90th days after surgery, the ear lymphedema was developed and maintained in all groups. In addition, there were no differences between groups according to the right and left ear thickness differences (Δ) on the 60th and 90th days after surgery. These results showed that the single or multiple venipuncture procedures did not increase the rabbit ear lymphedema compared with the control group. However, the findings of this study could not discuss the literature thoroughly because there has been no experimental study investigating the effects of venipuncture procedures in literature to our knowledge.
In literature, the role of venipuncture procedures in lymphedema has not been proven. In theory, venipuncture carries a small risk of infection that may cause recurrent or prolonged cellulitis, further damaging lymphatics. 26 This assumption has been queried in recent years because no evidence-based guidelines exist for lymphedema prevention. 4 Greene et al. reported that the risk is nearly zero due to the sterilization procedures applied before the venipuncture. 27 In addition, venipuncture for a rapid blood sample seems less likely to cause side effects (e.g., inflammation or infection) than intravenous infusion, lymphangiography, lymphoscintigraphy, acupuncture, or carpal tunnel surgeries applied affected side in lymphedema patients.
It was reported that sterile breakage of the skin during lymphangiography, lymphoscintigraphy, or even operative volume reduction does not cause infection in patients with lymphedema.28–31 Besides, Fulford et al. stated that hand surgery on the affected side of BCa patients received ALND does not increase the risk of lymphedema. 32 According to our results, both single and multiple venipuncture procedures applied in sterile conditions did not exacerbate lymphedema on rabbit ear lymphedema models. With this aspect, this study supported the recent literature as minimally invasive medical procedures, including venipuncture, may not trigger inflammation or infection and aggravate lymphedema in the rabbit ear lymphedema model.
Rabbit CRP leads to the idea that rabbits can be an ideal model for studying physiological and pathophysiological roles of human CRP. 33 Oohashi et al. reported that CRP has good sensitivity to inflammation in rabbits. 34 In addition, serum PCT has emerged as a more accurate biomarker for diagnosing systemic bacterial infections than clinical features or commonly used laboratory parameters (e.g., CRP concentrations).35,36 Although there are several studies about the inflammatory 37 and infectious markers16,38 in rabbits, we have not found any studies specifically about these markers on rabbit ear lymphedema model in the literature. Serum CRP and PCT analyses were used in this study to determine the systemic inflammation and bacterial infection after the venipuncture procedures, respectively.
The results of this experimental study indicated that none of the animals showed abnormally high blood inflammatory or infectious markers because CRP and PCT levels were below the lower detectable limits in all groups. According to the results of our study, in which we investigated whether lymphedema is triggered by inflammatory/infectious origin after venipuncture, there was no statistical difference in the amount of lymphedema after venipuncture. These findings demonstrate that no systemic inflammation or infection developed in the rabbit ear lymphedema model after the single/multiple venipuncture procedures compared with the control group. It may be explained that CRP and PCT concentrations remain relatively low in nonsevere, localized, or nonsystemic inflammation and infections.39,40 Further studies should examine the local effects (e.g., local inflammation or infection) of venipuncture procedures on lymphedema.
Based on experimental and clinical studies, inflammation is critical in lymphedema pathophysiology. 41 Macrophages perform multiple functions related to lymphedema progression, including regulation of lymphatic vessels, 42 inflammation, immunity, and tissue repair. 43 However, in an experimental study, including lymphovenous anastomosis on a rabbit ear lymphedema model, histopathological analysis investigating the accumulation of macrophages was performed on tissue samples obtained postanastomosis (on the 20th day) and post-ear lymphedema model surgery (on the 35th day).
The authors stated that they were unable to observe macrophages due to the rapid ability of rabbits to heal. 23 Similarly, according to the histopathological analyses in this study, no immune system cells, including macrophages, were detected on tissue samples obtained from rabbits. These results also could be due to the rapid healing process of rabbits. 44 Although an increase in the number of macrophages was reported in the early stage of lymphedema, a decrease in the number of macrophages was stated in the chronic stage in literature. 45 We did not euthanize the rabbits in the acute stage after venipuncture procedures in this study.
Therefore, we could not present the results of the histopathological analysis in the acute stage. We recommend performing histopathological analysis on tissue samples received during the acute stage of the venipuncture procedures to gain more insight into the process in future studies. In addition, the distance measurements of the histopathological analysis showed that there was still lymphedema on the 90th day after surgery in all groups; however, there were no differences between groups regarding the amount of lymphedema. These results supported to the ear thickness measurements measured with a vernier caliper in this study.
Conclusion
This study showed that single or multiple sterile venipuncture procedures did not seem to trigger infection or inflammation and increase the rabbit ear lymphedema. Unfortunately, we cannot directly predict the results of this experimental study to human subjects; it can only be extrapolated for humans. However, it can be speculated that the current anecdotal and strict recommendations, especially avoiding venipuncture for BCa patients who received ALND/SLNB, may be changed according to the results of this study. We speculated that sterile venipuncture procedures be applied to take a blood sample if there are no convenient veins or is an emergency involving BCa-related lymphedema patients. Much more evidence is needed to develop standardized evidence-based recommendations for venipuncture in BCa-related lymphedema patients.
Footnotes
Acknowledgments
The authors thank Vet. Med. Elif Erguvan Kaya and M.D. Tuba Saadet Deveci Bulut for their contributions to the study.
Authors' Contributions
All authors have read and approved the submission of this article. All authors contributed to the study concept and design. S.D. and O.K. performed surgical procedures. S.D. performed the ear thickness evaluations by a caliper. O.G. analyzed CRP and PCT levels. K.O. and I.K. delivered the blood samples and histopathological materials to the laboratory. P.U.G. evaluated histopathological analysis. O.G. and P.U.G. interpreted the biochemical and histopathological data, respectively. K.O. drafted the article and did the acquisition, analysis, and interpretation of data. I.K. and S.C. contributed to critical revisions of the article for important intellectual content. K.O. was responsible for statistical analysis. All authors provided study supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Projects of Scientific Investigation at Gazi University (grant No. 47/2018-07).