
Abstract
Background:
To demonstrate the magnetic resonance lymphangiography (MRL) imaging findings of lymphatic diseases and the clinical outcomes of lymphatic embolization in pediatric patients.
Methods and Results:
This retrospective study included 10 consecutive pediatric patients who underwent MRL for lymphatic diseases between June 2017 and June 2021. Nine patients underwent dynamic contrast-enhanced MRL with bilateral inguinal lymph node injection of diluted gadolinium, and one patient underwent nonenhanced MRL with a heavily T2-weighted image. The etiology of lymphatic disease was classified into three categories based on the magnetic resonance findings. The resolution of chylous fluid and weight-adjusted amounts of chylous fluid collected from a drainage tube were evaluated as outcomes. Patients were classified as postoperative lymphatic leak (n = 3), pulmonary lymphatic perfusion syndrome (n = 3), central lymphatic flow disorder (CLFD; n = 3), and primary lymphatic dysfunction (Gorham–Stout syndrome; n = 1). Three patients underwent radiological lymphatic intervention, and one CLFD patient underwent surgical intervention. In patients with postoperative lymphatic leak, the median chest tube drainage decreased significantly after the intervention [from 87.9 to 12.4 mL/(kg·d); p = 0.02]. However, in one CLFD patient, the amount of chylous fluid did not decrease until 7 days after intervention.
Conclusion:
The etiology of lymphatic disease in pediatrics can be recognized on MRL, and lymphatic intervention can be performed for cessation of lymphatic leak, even though the treatment outcomes may differ according to the underlying etiology. MRL can play an important role in classifying lymphatic disease, and in planning treatment on the basis of the lymphatic anatomy and underlying etiology.
Introduction
A
The traditional technique of interventional pedal or intranodal lymphangiography has limitations with respect to obtaining an understanding of the anatomical structure of the lymphatics because of its relatively low spatial resolution, weak contrast between lymphatics, and background structures when enhanced. 5 Although three-dimensional (3D) images could be acquired during the intervention using cone-beam computed tomography scanner, ionizing radiation exposure is inevitable. Furthermore, the embolic property of lipiodol, through inflammatory and granulomatous reaction resulting in fibrosis when extravasated, 6 could result in the lymphatic obstruction worsening the condition. The noncontrast enhanced T2-weighted magnetic resonance lymphangiography (MRL) has limited resolution of images and suboptimal for depicting anatomic details of lymphatic system and adjacent structures. Dynamic contrast-enhanced MRL (DCMRL) enables visualization of central lymphatics with a time course of contrast agent flow, and can reveal reflux, obstructions, and the degree of collateralization with 3D anatomy. 5
Recently, a study on DCMRL in patients with congenital heart disease investigated various pediatric lymphatic diseases, with the outcomes differing after lymphatic intervention performed according to the underlying etiology. 7 In that study, two causes of chylothorax, pulmonary lymphatic perfusion syndrome (PLPS) and central lymphatic flow disorder (CLFD), were suggested on the basis of the DCMRL findings. The underlying intactness and patency of the central lymphatics differ in each condition, and therefore the outcome of lymphatic intervention differed according to the underlying pathophysiology. In CLFD patients with a damaged or small thoracic duct, the traditional lipiodol-only embolization did not achieve an effective decrease in the amount of chest tube drainage. 7 This result implies the need to evaluate the etiology of chylothorax before determining the treatment plan.
DCMRL can help to understand the mechanism of lymphatic diseases and guide intervention by showing lymphatic anatomic structures and flow dynamics. However, DCMRL is not widely performed in pediatric patients because it requires an anesthesiology unit for general anesthesia or sedation. Recently, we performed DCMRL on pediatric patients suspected to have lymphatic disease before we planned lymphatic intervention. In this study, we describe DCMRL on 10 pediatric patients with various lymphatic disorders, reporting their clinical outcomes after lymphatic intervention.
Materials and Methods
Patient population
This study included 10 consecutive pediatric patients who underwent MRL for lymphatic diseases between June 2017 and June 2021. Nine patients underwent DCMRL with bilateral inguinal lymph node injection of diluted gadolinium, and one patient underwent nonenhanced MRL with a heavily T2-weighted magnetic resonance (MR) sequence. This retrospective observational study was approved by our Institutional Review Board (approval number: 2019-1327), and the requirement for informed consent was waived because of the retrospective nature. Patient demographics, clinical information, including underlying diseases, history of prior surgery or intervention, types of medical treatments for chylous fluid, MRL findings, types, and results of lymphatic intervention or surgery, and clinical courses after intervention or surgery were thoroughly reviewed. The presence of chylothorax or chylous ascites was defined when a high concentration of triglycerides was present in aspirated or drained fluid and/or when the fluid was lymphocyte predominant (>70%).
The etiologies of the lymphatic diseases were classified according to a previous study describing the DCMRL findings of 25 pediatric patients with postoperative chylothorax 7 : (1) postoperative lymphatic leak; (2) PLPS, a congenital condition in which the lymphatic flow is away from the thoracic duct to aberrant lymphatic vessels in the lung parenchyma, contrary to normal lymphatic flow; and (3) CLFD, a condition with abnormal lymphatic flow, presence of effusion in more than one compartment, and dermal backflow through lymphatic collaterals. The primary outcome was a complete resolution of chylothorax or ascites with consequent removal of the drainage catheter. The secondary outcome was defined as a reduction in the amount of chylous fluid from the drainage tube, with the weight-adjusted drainage of chylous fluid from the drainage tube being measured over 7 days before and after the intervention or operation.
Dynamic contrast-enhanced MRL
Before acquiring the MRL, the patient was laid in a supine position on an MR-compatible table outside of the magnetic resonance imaging (MRI) suite. First, patient was sedated by inhaling a mixture of oxygen and sevoflurane through facial mask by the anesthesiologist to minimize physical discomfort and movement. Then, needle positioning was performed by cardiovascular and pediatric radiologists (K.H.J. and Y.H.M.) through inserting a 26-gauge spinal needle into the cortex–medullar junction or the centers of the medulla of both inguinal lymph nodes under ultrasonographic guidance. Then, a 5-cc disposable syringe of a 1:1 mixture of 2–3 mL contrast material (Gadovist®, gadobutrol, Bayer, Inc.; or Dotarem®, gadoterate meglumine, Guerbet) and saline was connected to the needle. The total amount of contrast media used was up to 1 mL/10 kg for Gadovist and/or 2 mL/10 kg for Dotarem. After the patient was moved into the scanner room, inhalation anesthetics were discontinued and sedation was maintained by continuous infusion of propofol during MRL. Pediatric anesthesiologists performed the sedation and closely monitored the patient during MRL acquisition.
All MRL was performed using a 3-T MR scanner (Ingenia; Philips Healthcare). After the table was placed within the scanner gantry, a heavily T2-weighted turbo spin-echo fat saturation sequence was acquired in the axial and coronal plane for overall anatomy of the entire chest and abdomen. This sequence used the following parameters: repetition time/echo time, 1744.8/650.0 ms; flip angle, 90°; Cartesian k-space acquisition with acceleration factor of 2; field of view and matrix size were adjusted to patient size (e.g., field of view, 230 × 230 mm; and matrix, 232 × 165). Unenhanced T1-weighted high-resolution imaging with 3D fast filed echo (FFE) utilizing spectral attenuated inversion recovery method was acquired with the following acquisition parameters: repetition time/echo time, 3.0/1.5 ms; flip angle, 15°; and field of view and matrix size were adjusted to patient size (e.g., field of view, 230 × 230 mm; and matrix, 144 × 144).
After the T2-weighted and nonenhanced 3D FFE sequences were acquired, an enhanced 3D FFE sequence was acquired simultaneously with an intranodal injection of mixture of contrast and saline with injection rate of ∼2 mL/min. An enhanced 3D FFE sequence was then acquired every 1 minute until the contrast media passed the thoracic duct and drained into the left subclavian vein with systemic circulation.
Lymphatic intervention
Two interventional radiologists (S.J.H. and C.H.H.) performed conventional lymphatic interventions. Conventional intranodal lymphangiograms were performed using lipiodol, and when a leak was identified, thoracic duct embolization or lymphatic embolization using n-butyl cyanoacrylate was performed. For surgical intervention, one plastic surgeon (H.J.P.) performed lymphovenous anastomosis. Follow-up chest or abdominal radiography was performed in all patients.
Statistical analyses
The weight-adjusted volume of chest tube drainage in the 7 days before intervention or surgery was compared with the weight-adjusted volume of chest tube drainage in the 7 days after intervention (or until removal of the chest tube if it was removed before 7 days) using the Wilcoxon signed-rank test. All statistical analyses were performed using SPSS Statistics version 24.0 (IBM, Armonk, NY). p-Values <0.05 were taken to indicate statistical significance.
Results
Ten patients who underwent MRL were included in this study, with nine of these undergoing DCMRL. One patient (Tables 1 and 2) who suffered from severe respiratory distress caused by chest wall lymph edema underwent only nonenhanced MRL with a heavily T2-weighted sequence to minimize scan time. Four patients underwent lymphatic interventions using a radiological or surgical approach. The patient demographics, underlying diseases, and surgical or medical treatments are described in Table 1. The MRL findings, etiologies of the lymphatic diseases based on the imaging findings, and type of lymphatic intervention and its outcomes are summarized in detail for each case (Table 2; Fig. 1).
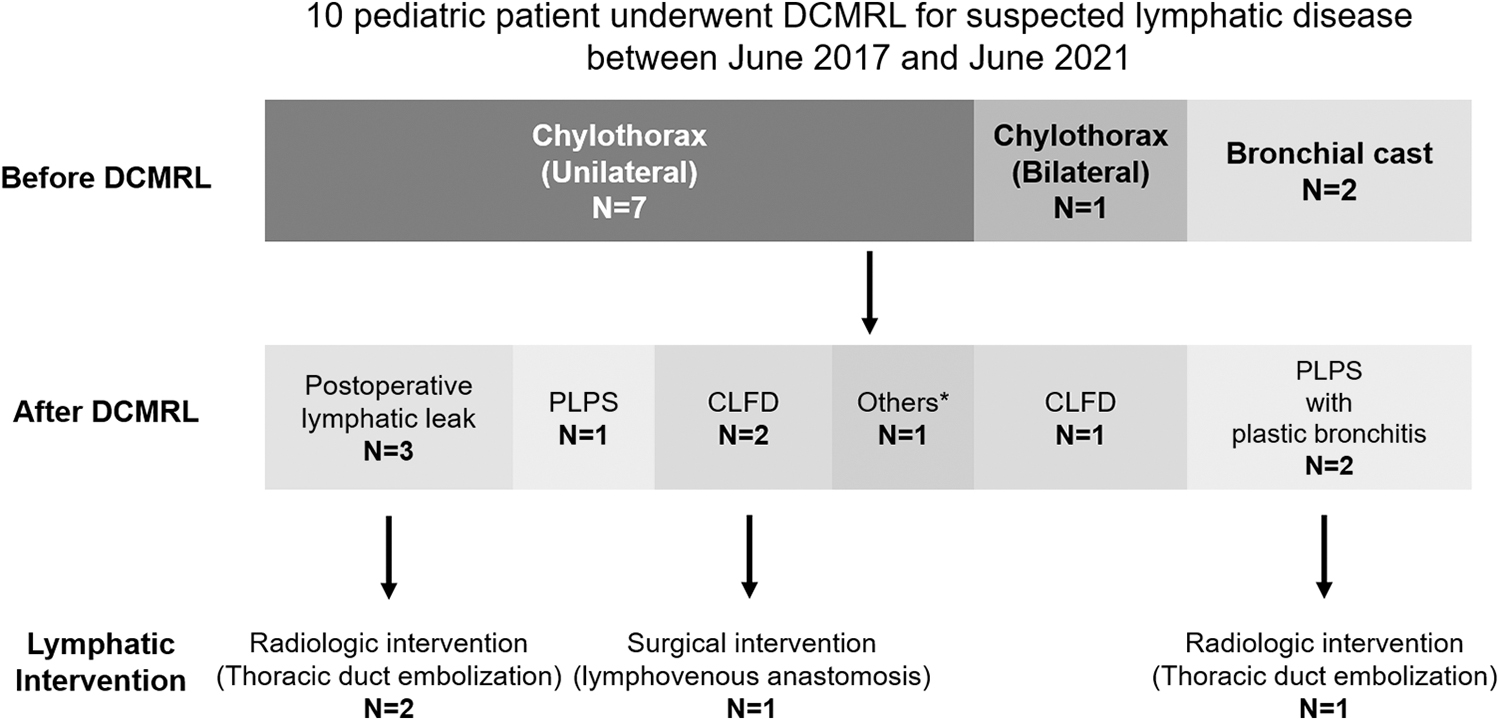
Etiology and treatment decisions based on DCMRL. *Finally diagnosed as Gorham–Stout syndrome, one of the causes of primary lymphatic disorder. CLFD, central lymphatic flow disorder; DCMRL, dynamic contrast-enhanced magnetic resonance lymphangiography; MRL, magnetic resonance lymphangiography; PLPS, pulmonary lymphatic perfusion syndrome.
Patient Information
ASD, atrial septal defect; BCS, bidirectional cavopulmonary shunt; DORV, double outlet right ventricle; PA, pulmonary atresia; PDA, patent ductus arteriosus; PS, pulmonary stenosis; TOF, tetralogy of Fallot; VATS, video-assisted thoracoscopic surgery; VSD, ventricular septal defect.
Lymphatic Images, Interventions, and Outcomes
CLFD, central lymphatic flow disorder; DCMRL, dynamic contrast-enhanced magnetic resonance lymphangiography; PLPS, pulmonary lymphatic perfusion syndrome.
Etiology and MRL findings
In three patients who were classified as postoperative lymphatic leak, two showed a leak of contrast media to the pleural space (Figs. 2 and 3; Supplementary Videos S1 and S2), but no definite leak was identified in the other patient (#7). Three patients were categorized as PLPS (Fig. 4), and three other patients were suggested to be CLFD (Fig. 5; Supplementary Video S3). One remaining patient (#1) showed no identifiable abnormality on DCMRL: the thoracic duct was intact and there was no demonstrable abnormal lymphatic flow, except for a small amount of left pleural effusion. Initially, the patient was considered as idiopathic chylothorax but was finally shown to have Gorham–Stout syndrome, one of the causes of primary lymphatic disorder.
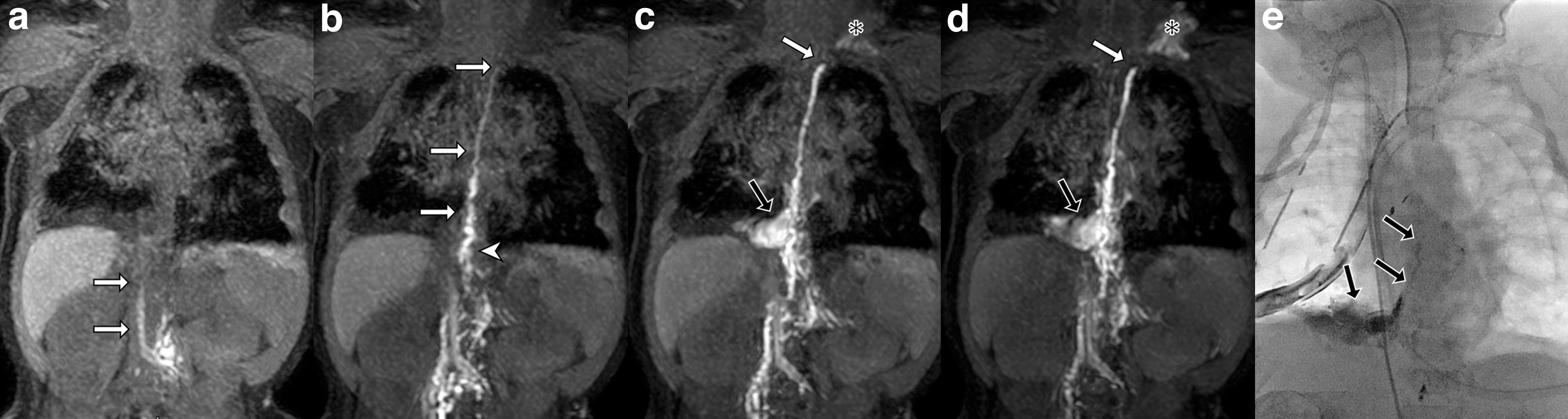
Postoperative lymphatic leak (Supplementary Video S1). A 10-month-old girl presented with postoperative chylothorax after right lower lobe lobectomy. DCMRL was performed on postoperative day 24. Coronal 3D T1-weighted image with thin MIP reconstruction obtained

Postoperative lymphatic leak (Supplementary Video S2). An 11-month-old boy presented with postoperative chylothorax after left aortic arch division and patent ductus arteriosus ligation. DCMRL was performed on postoperative day 8. Coronal 3D T1-weighted imaging with thin MIP reconstruction at immediate
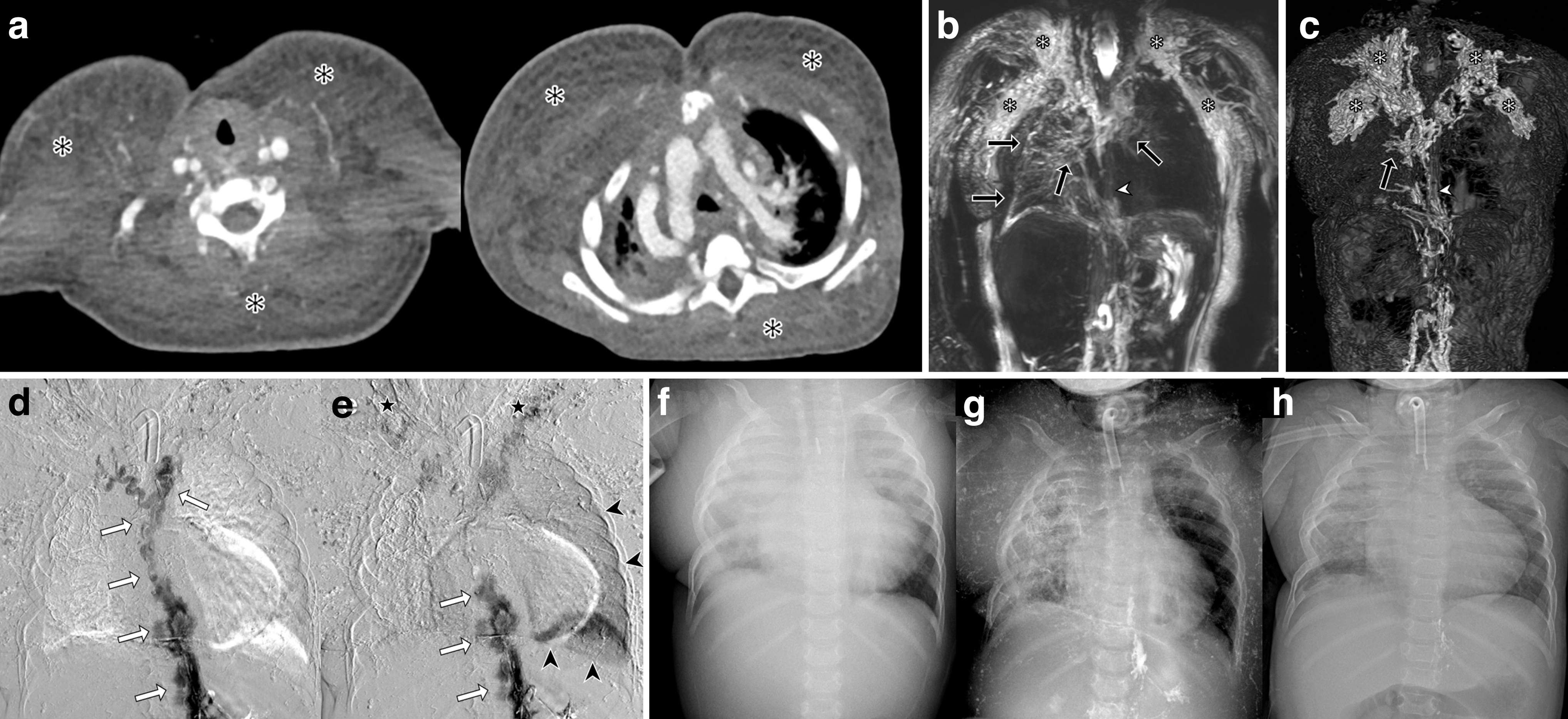
Pulmonary lymphatic perfusion syndrome. Plastic bronchitis in a 2-year-old boy after a Rastelli operation. Enhanced chest CT
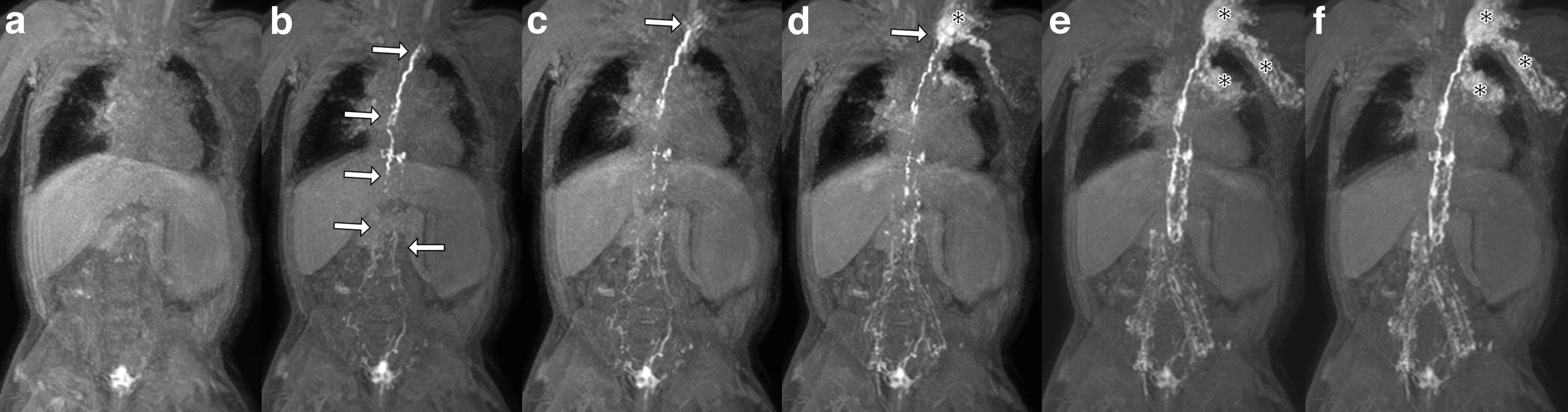
Central lymphatic flow disorder (Supplementary Video S3). A 3-year-old boy with acquired thoracic duct outlet obstruction after recurrent central venous catheter insertion to left brachiocephalic vein for hemodialysis. Coronal 3D T1-weighted imaging with thin maximum intensity projection reconstruction at 1
All patients with postoperative lymphatic leak or CLFD had pleural effusion detected on T2-weighted images. In three cases of CLFD, two patients had left-sided pleural effusion with poor visualization of the thoracic duct, and one patient had bilateral pleural effusion. Two patients with PLPS presented with plastic bronchitis, and one with bilateral pleural effusion. In these two patients, the thoracic duct was interrupted or partially nonvisualized, and increased lymphatic flows to the right perihilar area and bronchovascular bundle were observed on MRL (Fig. 4).
Ascites was detected in four of the 10 patients, two of three patients with CLFD, and two of three patients with postoperative lymphatic leak. No PLPS patients presented with ascites. The cisterna chyli, which is a possible approach route for lymphatic intervention, was identifiable on MRL in 6 of the 10 patients.
Lymphatic imaging and interventions
Conventional intranodal lymphangiography was performed in 6 of 10 patients: three with a postoperative leak, two with PLPS, and one with CLFD. In three cases of postoperative lymphatic leak, a leak of contrast media from the thoracic duct to the pleural space, or from the central pelvic or lumbar lymphatic channel to the pelvic cavity, was identified during conventional lymphangiography. In one PLPS patient, conventional lymphangiography failed to visualize the lymphatics above the L3 level, whereas visualization of the more proximal portion of the central lymphatics, including the thoracic duct, was available through DCMRL. In the other PLPS patient, conventional lymphangiography demonstrated lymphatic networks to both the lower neck and upper chest wall, which corresponded with the DCMRL findings. One CLFD patient showed faint thoracic duct and lymphatic flows in the abdominal wall on conventional lymphangiography.
Lymphatic intervention was performed in four patients: two with postoperative lymphatic leak, one with PLPS, and one with CLFD. Among these four patients, three (two with postoperative lymphatic leaks and one with PLPS) underwent radiological intervention with lymphatic embolization. The median procedure time for lymphatic intervention (lipiodol embolization) was 69 minutes (range, 69–124 minutes). The median total air kerma dose was 59 mGy (range, 57–190 mGy), and the median total dose area product was 433 mGy/m2 (range, 433–1261 mGy/m2). One CLFD patient underwent surgical intervention, both lymphovenous anastomosis between lymphatic vessel and vein (side-to-end anastomosis) in feet dorsum area and lympho-nodo-venous microsurgical shunt between the inguinal lymph node and the superficial inferior epigastric vein (side-to-end anastomosis through direct puncture of medulla of lymph node) were performed. 8
Outcomes
The serial changes in the amount of chest tube drainage before and after lymphatic intervention were demonstrated in Figure 6. In two patients with postoperative lymphatic leak, the median weight-adjusted chest tube drainage decreased significantly from 7 days before [87.9 mL/(kg·d); range, 75.7–304.3 mL/(kg·d)] to 7 days after radiological intervention [12.4 mL/(kg·d); range, 9.5–37.8 mL/(kg·d); p = 0.02]. However, in a CLFD patient who underwent surgical intervention, the median chest tube drainage did not decrease from 7 days before [7.7 mL/(kg·d); range, 0.9–39.8 mL/(kg·d)] to 7 days after the intervention [39.7 mL/(kg·d); range, 27.5–48.7 mL/(kg·d)]. This patient finally showed partial resolution of the left chylothorax 48 days after the intervention and was discharged safely. In one PLPS patient, a comparison of the amount of drainage could not be performed because a drainage catheter was not inserted.

Chest tube drainage before and after lymphatic intervention. In patients with postoperative lymphatic leak (blue line), the median chest tube drainage significantly decreased after intervention [from 87.9 to 12.4 mL/(kg·d); p = 0.02], whereas there was persistent lymphatic leak in the CLFD patient (orange line); [from 7.7 to 39.7 mL/(kg·d)]. The length of the bars at each point indicates standard deviation of weight-adjusted chest tube drainage.
Among the three patients who underwent radiological intervention, two with postoperative lymphatic leak showed complete resolution while the other had partial resolution of chylothorax, respectively. The other patient with PLPS showed partial resolution of the left chylothorax. There was improvement in the unilateral chylothorax in one patient with postoperative lymphatic leak after only conventional intranodal lymphangiography without intervention. However, in the other two patients with PLPS or CLFD, intranodal lymphangiography alone was not effective. No postprocedural complications were observed in any patients.
Two of the patients suffered mortality. One patient with PLPS who was discharged 220 days after DCMRL expired because of sepsis 540 days after discharge. The other patient with postoperative lymphatic leak expired during hospitalization 99 days after conventional lymphangiography because of respiratory distress resulting from underlying bronchopulmonary dysplasia. Eight of 10 patients survived from lymphatic imaging or intervention to discharge (discharge was after a median of 9 days in three patients who underwent lymphatic imaging only, and after a median of 42 days in five patients who underwent lymphatic intervention).
Discussion
We evaluated 10 consecutive pediatric patients with suspected lymphatic disease who underwent MRL and assessed their etiology using four categories based on DCMRL findings: postoperative lymphatic leak (n = 3), PLPS (n = 3), CLFD (n = 3), and primary lymphatic disorder without demonstrable organic cause on DCMRL (n = 1). Among these patients, four underwent lymphatic interventions, and the treatment outcome was different in each group. In patients with postoperative lymphatic leak, median chest tube drainage significantly decreased after the intervention, whereas the amount of chest tube drainage significantly increased in one CLFD patient.
The differences in treatment response are related to the underlying etiology. Thoracic duct embolization could be a first-line treatment in patients with postoperative lymphatic leak or PLPS, reducing the leakage of aberrant lymphatics from the thoracic duct. However, it would not be appropriate for CLFD as it would worsen the central lymphatic occlusion. According to the definition of CLFD by Savla et al., 7 the increased lymphatic flows causing effusions and dermal backflow result from abnormal central lymphatics. The three patients classified as CLFD in our study had thoracic duct obstruction at the drainage site (#8) or a faint thoracic duct (#6, #10) on DCMRL. Because DCMRL has good sensitivity for the identification of abnormalities in antegrade central lymphatic flow and additionally demonstrates dermal backflow, we were able to classify the etiology of these patients as CLFD. In a situation of lymphatic collaterals decompressing the pressure of the central lymphatics, the thoracic duct embolization technique used for postoperative leak or PLPS could fail and worsen the effusions by increasing the pressure of the central lymphatics.
In a previous study, there was no significant improvement in chest tube drainage after lymphatic intervention (lipiodol embolization) in CLFD patients. 7 Therefore, on the basis of the DCMRL findings, our clinicians and radiologists decided to perform lymphovenous anastomosis to bypass and decompress the central lymphatic obstruction, rather than thoracic duct embolization. Although the chylous fluid draining from the chest tube seemed to increase in amount immediately after the surgical intervention, the patient was finally discharged with partially resolved left chylothorax.
The DCMRL imaging findings contributed to the treatment decisions in the patients with postoperative lymphatic leak or PLPS. A definite contrast leak was observed on the DCMRL of two of three patients with postoperative lymphatic leak. Both patients underwent lipiodol lymphangiography with or without thoracic duct embolization, and chylothorax subsequently resolved. In one patient (#7), a contrast leak from the central lymphatics was not observed on DCMRL but was detected on conventional intranodal lymphangiography. On conventional lymphangiography, a small amount of contrast leaked from the central lymphatics in the upper lumbar level, not from the thoracic duct, therefore, it may have been difficult to detect this tiny leak with insufficient contrast material and early termination of the dynamic acquisition.
A decreased flow caused by long-standing fat restriction could also contribute to poor visualization of the leak on DCMRL. In patients with PLPS, DCMRL helped planning management by visualizing the anatomy of the thoracic duct. In patient #2, interruption of the proximal thoracic duct and increased lymphatic flow to the right perihilar area made the interventional radiologist decide to reduce the lymphatic flow through embolization.
In patient #3, DCMRL enabled assessment of the thoracic duct, which conventional lymphangiography with contrast material of higher viscosity than gadolinium failed to visualize. Visualization of the patent thoracic duct and multiple engorged lymphatic flows to the right pleural space allowed the cause of respiratory difficulty with casts to be diagnosed as plastic bronchitis secondary to PLPS. Interventional radiologists initially decided to perform thoracic duct embolization, but this failed because of poor visualization of the thoracic duct, and the clinicians started low-dose oral azithromycin for the treatment of plastic bronchitis. DCMRL findings revealed the cause of the right chylothorax in patient #9 to be PLPS, and the chylothorax resolved with diet modification (low long-chain triglyceride diet) without additional lymphatic intervention. Conversely, in patient #1 who had primary lymphatic dysfunction (Gorham–Stout syndrome), the DCMRL finding was normal without any organic cause. Therefore, pleurodesis was performed instead of lymphatic intervention.
The DCMRL findings and their influence on decisions on lymphatic interventions suggest the importance of understanding the underlying etiology of lymphatic disease. 7 When leaking or increased lymphatic flow was identified on DCMRL in patients with postoperative leak or PLPS, thoracic duct embolization led to improvement of chylothorax. In a case of CLFD, a decision to perform lymphovenous anastomosis following recognition of a thoracic duct obstruction on DCMRL brought partial improvement of the chylothorax. If conventional thoracic duct embolization was performed instead of lymphovenous anastomosis, the chylothorax would probably have been worsened because of further impairment to the drainage of the thoracic duct. Lastly, pleurodesis was considered an appropriate plan for a patient with primary lymphatic dysfunction who had no demonstrable organic cause on DCMRL. For the reasons mentioned above, different treatment plans based on underlying lymphatics could effectively remedy the abnormal lymphatic flows, resulting in clinical success.
The outcomes of particular procedures differed according to the etiology in a previous study, 7 and the approach can be changed when the etiology and underlying anatomy of the central lymphatics are recognizable before surgery. Therefore, we suggest that evaluation of the underlying lymphatic etiology through DCMLR should be considered in pediatric patients suspected of chylothorax, chylous ascites, bronchial cast, or lymphedema.
The main limitations of our study are its retrospective design and the small number of patients. Although we collected the patients from a single tertiary referral hospital, the rarity of the disease, requirement for an anesthesiology unit for sedation, and contraindications for MRI or sedation contributed to the small patient numbers. In addition, lymphatic intervention is not widely performed in pediatric patients because of the reasons described above, and less than half of the patients underwent lymphatic intervention. The number was therefore insufficient to describe the relationships between the outcomes of lymphatic intervention within various etiologies and different outcomes across etiologies. A further large-scale study may be required to emphasize the role of DCMRL before planning treatment.
Conclusion
The different etiologies of lymphatic disease in pediatric patients can be recognized on DCMRL, and different lymphatic interventions appropriate for the underlying etiology can be adopted. DCMRL could be a useful imaging modality for the differential diagnosis of lymphatic disease, providing 3D anatomy and being free of ionizing radiation. By assessing the central lymphatics, DCMRL can play an important role in the classification of lymphatic disease and the planning of treatment based on anatomy and underlying etiology.
Footnotes
Acknowledgment
The authors offer special thanks to Gyoungro Lee (MR Application Specialist, BMDS MR Health Systems, Phillips Korea) for his support on establishment of MRI protocol.
Authors' Contributions
Y.A.: Data curation (lead), formal analysis (lead), investigation (lead), and writing—original draft (lead). H.J.K.: Conceptualization (lead), formal analysis (equal), supervision (lead), and writing—review and editing (lead). H.M.Y.: Data curation (equal), supervision (equal), and writing—review and editing (equal). J.C., D.H.Y., and J.-W.K.: Data curation (equal), supervision (equal), and writing—review and editing (equal). E.-Y.J. and M.-H.S.: Data curation (equal), resources (equal), supervision (equal), and writing—review and editing (equal). J.H.S.: Conceptualization (equal), data curation (equal), resources (lead), supervision (equal), and writing—review and editing (equal).
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This study was supported by a grant (2021IT0006) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.